
Translate this page into:
X-ray Digital Linear Tomosynthesis Imaging for Artificial Pulmonary Nodule Detection
Address for correspondence: Dr. Tsutomu Gomi, School of Allied Health Sciences, Kitasato University, 1-15-1, Minami-ku, Kitasato, Sagamihara, Kanagawa-252-0373, Japan. E-mail: gomi@kitasato-u.ac.jp
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The purpose of this paper is to identify indications for volumetric X-ray digital linear tomosynthesis (DLT) with single- and dual-energy subtraction techniques for artificial pulmonary nodule detection and compare X-ray DLT, X-ray digital radiography, and computed tomography.
Keywords
Dual-energy subtraction
pulmonary nodules
tomosynthesis

INTRODUCTION
Interest in tomosynthesis and its clinical applications has been revived by recent advances in digital X-ray detector technology. In tomosynthesis, an X-ray tube and an X-ray receptor are positioned on either side of the object. Tomosynthesis captures only one set of discrete X-ray projections that can be used to reconstruct any plane of the object retrospectively. This article will review and identify indications for X-ray digital linear tomosynthesis (DLT).
CHEST PHANTOM SPECIFICATIONS
The chest phantom (N-1 type, Kyoto Kagaku Co., Tokyo, Japan) and the artificial pulmonary nodules of type N1 are depicted in the images [Figures 1 and 2]. The artificial pulmonary nodules were of the ground-glass opacity type (5 and 7 mmφ), and the spheres were of the same diameter and composition. For the dual-energy evaluation study, calcification was simulated using hydroxyapatite (powder type). The relationship between the radiation attenuation properties of glass and those of real pulmonary nodules was correlated.
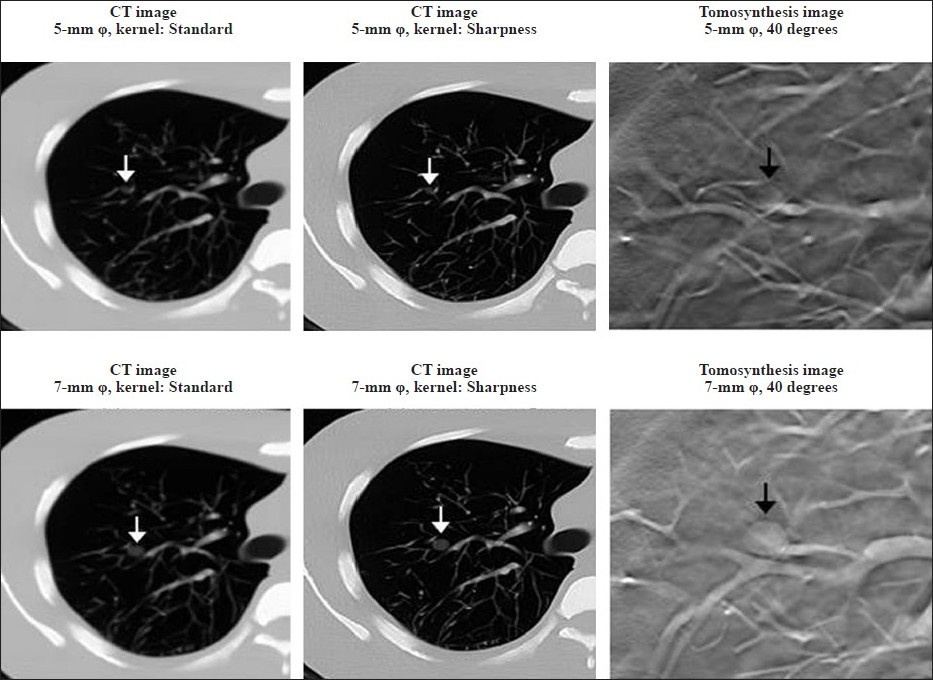
- Tomosynthesis (SonialVision Safire II, Shimadzu Co., Kyoto, Japan) and CT (64-slice SOMATOM Definition scanner; Siemens Medical Systems, Forchheim, Germany) images of the artificial pulmonary nodules (ground-glass opacity type). The quality of the images obtained by tomosynthesis imaging were clearer than those obtained by CT (CT slice thickness: 5 mm).
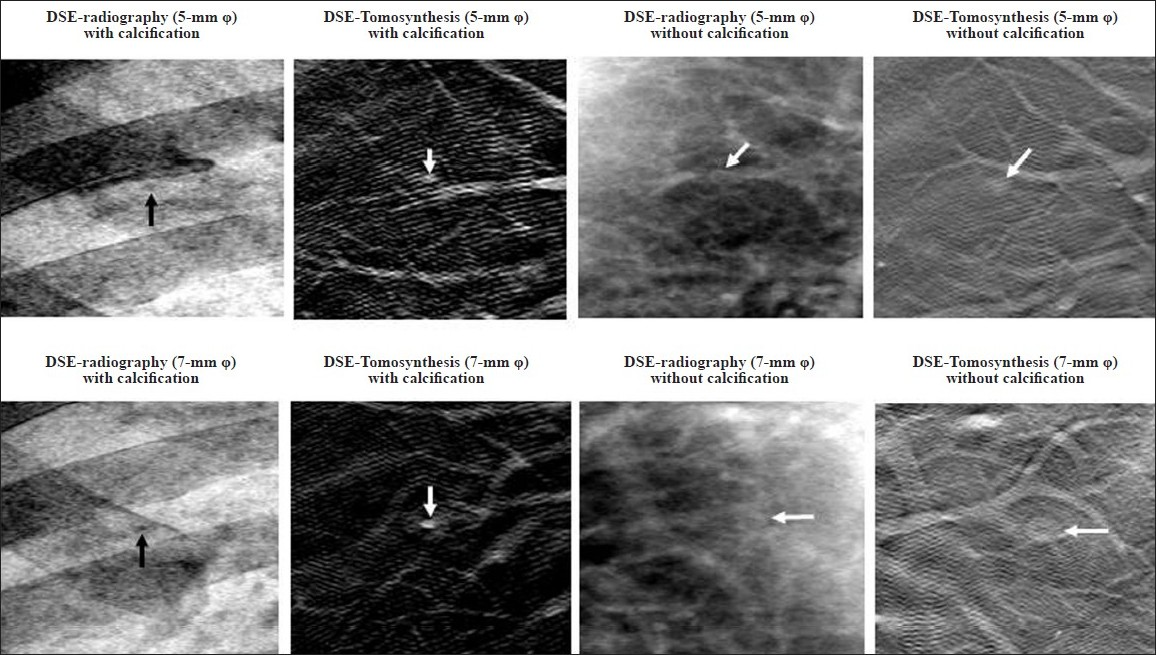
- DES-Tomosynthesis and DES radiography (SonialVision Safire II) of the same slice, demonstrates the content of the artificial pulmonary nodules with and without calcification. The high-contrast detectability phantom case having a clear, contrast detectability on DES-Tomosynthesis imaging produced for identical planes (tomosynthesis acquisition angle: 40).
APPLICATION OF TOMOSYNTHESIS IN CHEST EXAMINATION
Owing to its high sensitivity, normal-dose helical computed tomography (CT) is currently considered the gold standard for lung cancer detection. Early reports indicate that low-dose helical CT has the potential to detect early lung cancer, and thus decrease morbidity. CT has the advantage of improved detection of lesion by eliminating visual clutter of overlying anatomy [Figure 1]. However, there are disadvantages of using CT when compared with chest radiography, such as high-radiation dose and cost. On the other hand, although chest radiography has advantages such as short examination time, low cost, and easy access, there are also important disadvantages such as low sensitivity and specificity.
In chest radiography, the three-dimensional chest is projected onto a two-dimensional image. Consequently, the ability to detect pathological findings is limited by the overlapping anatomy rather than by quantum noise. Chest radiography has been shown to have a relatively low sensitivity for the detection of pulmonary nodules. The poor sensitivity of chest radiography precludes its use as a screening modality, despite its advantages of low cost, low dose, and wide distribution of devices.
DLT is a method that provides some of the tomographical benefits of CT at a reduced radiation dose and cost and with an approach that can be easily implemented in conjunction with chest radiography. Current state of DLT originates from the older technique of geometric tomography, which has largely fallen out of favor in chest imaging owing to positioning difficulty, high radiation dose, and residual blur from out-of-plane structures. DLT overcomes the difficulties of geometric tomography by permitting reconstruction of numerous slices of the image from a single low-dose acquisition of image data [Figure 1]. Although improving detection of pulmonary nodules may be an early area of emphasis for the application of tomosynthesis, it also has potential for use in other areas of thorax imaging.[1–2]
POSSIBILITY OF DUAL-ENERGY SUBTRACTION IMAGING
Presence of calcification and stability of the mass over 2 years suggest its benign nature.[3] A benign pattern of the calcifications has been considered necessary to exclude malignancy.[4] In the evaluation of diffusely disseminated pulmonary nodules, identification of diffusely disseminated pulmonary nodules and calcifications in the nodules has been helpful in limiting the differential diagnosis.[5] Conventional radiography and conventional tomography have been used to detect calcifications, but they have been largely replaced by CT.[3] However, CT has several inherent problems, including motion artifacts and the variety of reconstruction algorithms that are used by different CT scanners.
Dual energy subtraction (DES) imaging has been proposed and investigated by many researchers as a means of reducing the impact of anatomic “noise” on disease detection by chest radiography. DES involves making two radiographical projections of the patient using different energy X-ray beams. By exploiting the difference in the energy dependence of attenuation between bone and soft tissue, the bone contrast can be reduced to produce a soft tissue image and the contrast of the soft tissue can be reduced to produce a bone image.[6] DES digital radiography has been found to be useful in detecting calcifications within pulmonary masses.[78] Main drawback of the DES technique, is that its projections may result in overlap of anatomical features (e.g., calcifications superimposed over the ribs or spine).
DES DLT is a new technique, and therefore there is no guidance for its integration into the clinical practice of chest radiography. The most reliable signs for discriminating between benign and malignant masses are the growth rate of the mass and presence or absence of calcifications within the mass. Since calcifications are commonly observed in benign masses and no other radiographical characteristic is specific in characterizing a mass, it is important to detect and characterize calcification within lesions. Using DES DLT, the presence, distribution, and characteristics of calcifications in lung nodules can be assessed to an extent that is not possible with currently available CT imaging and projection-type DES techniques. In addition, this technique is not susceptible to the problems of image overlap, partial volume effect, or shifting of the image plane [Figures 2 and 3].
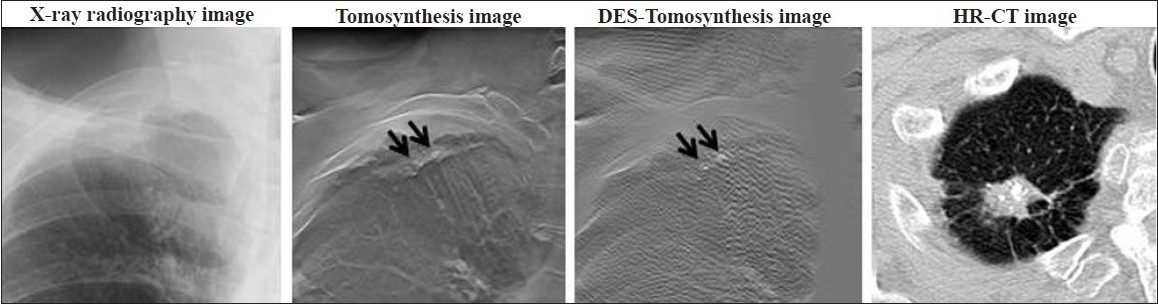
- Calcified tuberculous foci in a 74-year-old man. Comparison of the chest images obtained with X-ray radiography, digital tomosynthesis, DES-Tomosynthesis, and high-resolution CT (HR-CT). DES-Tomosynthesis and HR-CT appear to have similar accuracy in detecting calcification in the pulmonary nodules. However, DES-Tomosynthesis has a greater clinical potential.
POTENTIAL ARTIFACTS
Ideally, structures in a given plane of interest should be clearly displayed in the corresponding tomosynthesis reconstruction plane, whereas structures located outside of that plane should not be visible. Essentially, the limited angular range of the tomosynthesis image acquisition geometry dictates that spatial resolution is limited in the dimension perpendicular to the detector plane. As a result, out-of-plane structures cannot be completely removed from the reconstruction plane and are present in every such plane. However, most of these structures are not visible because various low-amplitude structures from projections overlap in the reconstruction plane, and therefore, appear blurred. Out-of-plane structures from high-attenuation features cannot be blurred and appear as multiple replicates in every reconstruction plane, except for the one in which the actual high-attenuation feature (e.g., rib) is located. At one projection angle, these ghosting features are distributed along the line made by the X-ray source and the actual feature [Figure 4].
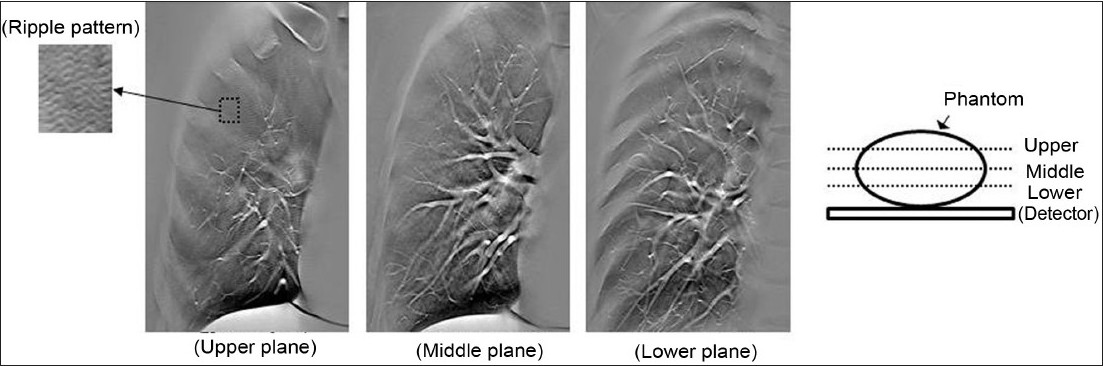
- Out-of-plane structures are present in every reconstruction plane, but most are not visible because the various low-amplitude structures from projections overlap each other in the reconstruction plane, and therefore are blurred.
CLINICAL RELEVANCE
Tomosynthesis is worthy of further evaluation because it is flexible and can accurately reproduce the shape of an artificial pulmonary nodule. Tomosynthesis can be considered the modality of choice to detect and investigate simulated artificial pulmonary nodules with and without calcification. Understanding the imaging potential of tomosynthesis will lead to significant improvements in diagnostic accuracy.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp? 2011/1/16/76694
REFERENCES
- Comparison of chest tomosynthesis and chest radiography for detection of pulmonary nodules: Human observer study of clinical cases. Radiology. 2008;249:1034-41.
- [Google Scholar]
- Effect of clinical experience of chest tomosynthesis on detection of pulmonary nodules. Acta Radiol. 2009;50:884-91.
- [Google Scholar]
- Calcification in pulmonary nodules.detection with dual-energy digital radiography. Radiology. 1986;160:595-601.
- [Google Scholar]
- Differential diagnosis in conventional radiology. Berlin: Thieme Verlag; 1991.
- A method for selective tissue and bone visualization using dual-energy scanned projection radiography. Med Phys. 1981;8:659-67.
- [Google Scholar]
- Dual-energy digital radiographic quantification of calcium in simulated pulmonary nodules. AJR Am J Roentgenol. 1987;148:19-24.
- [Google Scholar]
- One-shot dual-energy subtraction chest imaging with computed radiography. Radiology. 1988;168:67-72.
- [Google Scholar]




