
Translate this page into:
Evaluation of Normal Morphology of Mandibular Condyle: A Radiographic Survey

*Corresponding author: Bhupender Singh, MDS, Oral Medicine and Radiology, Senior Resident, Department of Oral Medicine and Radiology, Government Dental College, Kottayam Kerala, India. negibhupender13@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh B, Kumar NR, Balan A, Nishan M, Haris PS, Jinisha M, et al. Evaluation of normal morphology of mandibular condyle: A radiographic survey. J Clin Imaging Sci 2020;10:51.
Abstract
Objectives:
The temporomandibular joint (TMJ) is a complex, highly specialized joint. Along with the teeth, these joints are considered to be a “tri-joint complex.” Mandibular condyle morphology is characterized by a rounded bone projection with an upper biconvex and oval surface in axial plane. Anatomical knowledge of the TMJ is one of the basic foundations of clinical practice, allowing the understanding of TMJ pathologies and fabrication of condylar prostheses. The cross-sectional descriptive study was undertaken to evaluate normal variation in the condylar morphology on radiographs in persons without TMJ symptomatology and its relation to age, gender, dentition status, chewing habits, parafunctional habits, history of orthodontic treatment, and denture wearing was assessed.
Material and Methods:
A total of 350 subjects without TMJ symptomatology included in the study were further grouped by age, gender, dentition status, chewing habits, parafunctional habits, history of orthodontic treatment, and denture wearing history. Panoramic radiograph was taken for the assessment of condylar morphology.
Results:
A significant association between dentition status and bilaterally similar condylar morphology was noticed. Bilaterally similar condyles were seen in 81.4% of subjects. Round-shaped condyles were seen in 176 (62%) persons. Loss of bilateral occlusion tends to alter the condylar morphology. Association between normal chewing habits and bilaterally similar condyle shapes was significant.
Conclusion:
The study describes the normal morphology of mandibular condyles in a population attending the tertiary dental care center, Kozhikode. The dentition status and chewing habits of individuals had a significant role in determining condylar morphology.
Keywords
Panoramic radiograph
Mandibular condyle
Morphometry

INTRODUCTION
The temporomandibular joint (TMJ) is one of the most complex articulations of the human body. Working bilaterally and simultaneously, it connects the mandible to the cranium. Specific anatomic components of the TMJ include the mandibular condyle, the mandibular fossa and articular eminences of the temporal bone, and the soft-tissue components of the articular disk, its attachments, and the joint cavity.[1]
The function and health of TMJ is vital to life. The functions of the TMJ are to provide smooth, efficient movement of the mandible during mastication, swallowing, and speech and to provide stability of mandibular position and prevent dislocation from external or unusual forces. The condyle is very special because expression of the mandibular growth is provided by mandibular condyle.[2] Mandibular condyle varies considerably both in size and shape. When viewed from above, the condyle is roughly ovoid in outline. It is 15–20 mm side to side and 8 to 10 mm from front to back.[3]
A normal variation of the condylar morphology occurs with age, gender, facial type, occlusal force, functional load, malocclusion type, and between right and left sides. The most prevalent morphologic changes are detected in the TMJ of elderly persons due to the onset of joint degeneration. TMJ morphology has been studied on dry and autopsy human skulls, radiographic examinations,[4,5] magnetic resonance, computed tomography, and cone-beam computed tomography methods. The basic morphology of mandibular condyle is thought to be established early and modified throughout life according to functional load.
Panoramic radiography is a simple, low-cost method to evaluate the bony structures of the TMJ and is one of the most commonly used techniques by dentists and dental specialists. Its principle is based on the tomographic concept of imaging a section of the body while blurring images outside the desired plane so that the TMJ and teeth are in focus, but adjacent structures are blurred.
Imaging of the TMJ may reveal osseous or positional abnormalities, but even when abnormalities are seen, it is not clear how frequently these radiograph influence a clinician’s decision-making and how they impact on patient care. Interpreting TMJ imaging studies require an understanding of the pathophysiology of the joint and knowledge of both normal and pathologic anatomy of the joint and surrounding structures. Therefore, it is essential to present details about the joint anatomy, joint physiology, and function before highlighting the joint dysfunction and joint pathology.
The appearance of mandibular condyle varies greatly among different age groups and individuals. Computed tomography and MRI are helpful to overcome limitations of panoramic radiography, however, their use is limited to a small number of patients, and are usually used as a second choice.
The present study was undertaken to assess the frequency of different shapes of mandibular condyle on panoramic radiographs without TMJ symptomatology. Assessment of condylar morphology in patients without temporomandibular joint disorders (TMDs) in relation to age, gender, dentition status, normal chewing habits, parafunctional habits, history of orthodontic treatment, and history of usage of denture with the aid of panoramic radiograph was done. No such studies have been undertaken in the Kerala population.
MATERIAL AND METHODS
Persons who attended the radiology clinic in the department of oral medicine and radiology, a Tertiary Care Center North Kerala, over a period of 16 months (March 2015–June 2016) were screened. A Descriptive ,Cross-sectional study has been undertaken to assess the condylar morphology. All subjects who had no symptoms TMD and were having their panoramic view for other oral disorders were included in the study.
The main features of TMDs encompass pain in the masticatory musculature and/or joint which can radiate, locking of the jaw, inability to open the mouth fully, dislocation, noises like clicking and crepitus during joint movement, headache, tightness around the face in the morning; and referred pain to the ear.
TMD symptoms
Classic triad of symptoms – pain, joint sound and restriction/ deviation of joint movements. Others – headache, tinnitus, ear ache, fullness of ears, altered hearing, trigger zones of pain on orofacial region, neck pain etc.
Double TMJ view was taken only for those subjects whose panoramic view showed doubtful condylar morphology. This is a special radiographic investigation done for TMJ with a Panoramic unit, that depicts a lateral tomographic section of both joints in open and closed position of mouth, in single image. Main advantage is that, we can efficiently compare joint position and its morphology.
Technique
The patient is positioned with their Frankfurt plane angled 5° downwards within a panoramic unit with their mouth closed but using a special nose/chin support, instead of the bite-peg.The head is accurately positioned using the light beam markers and immobilized using the temple supports, the distance from the external auditory meatus to the canine light is measured and the anteroposterior position of the chin support adjusted manually to ensure that the condyles appear in the middle of the image. During the exposure, first the left and then the right condyle is imaged in the closed position. The equipment automatically returns to the start position, the patient is instructed to open the mouth.
The left and right condyles are then exposed in the open position and the resultant image.
Diagnostic information
The information provided includes: The shape of the condylar heads and the condition of the articular surfaces from the lateral aspect, the range of movement of the condyles when the mouth is open, A direct comparison of both condylar heads. Main advantage is that, we can efficiently compare joint position and its morphology.[6] All radiographs were acquired in the same machine (PLANMECA 2002 CC PROLINE, FINLAND) at the department of oral and maxillofacial radiology, a tertiary care center North Kerala. Visualization of condyles on both sides was possible on radiograph.
A total of 650 persons over the age of 18 years without clinical features of TMJ symptoms were examined in detail. Out of 650 persons, 350 individuals who satisfied the inclusion criteria were included in the study after obtaining the informed consent. Prior approval from the ethical committee, Government Dental College Kozhikode has been taken before the procedure.
Persons who were asymptomatic for TMJ pain and were advised panoramic view for other oral disorders and orofacial pain. They were further grouped by age and dentition status. Chi-square test was used to evaluate normal condylar morphology associated with age, gender and dentition status, chewing habits, parafunctional habits, and history of usage of denture.
Specification of radiographic machine and used radiographic view
Advanced panoramic and cephalometric machine (PLANMECA 2002 CC PROLINE, FINLAND), with an 80 kVp and 12 mA provided with a total filtration of 2.5 mm aluminum and an effective focal spot of 0.5 × 0.5, was used to take panoramic view and double TMJ view.
Exclusion criteria
Persons below 18 years of age, patients with TMDs, patients with maxillofacial trauma and history of condylar fracture, patients with degenerative bone diseases, patient with oral malignancy, patients with severe malocclusion, patients with a history of orthodontic treatment having with skeletal deformity, and persons whose radiographs do not reveal the condylar anatomy clearly were excluded from the study group.
Dentition status clinically examined and classified into three classes using Eichner index[7,8] [Figure 1] (dentition status of antagonist jaws serves as the basis for the Eichner index) [Figure 1]. The zone is called supporting if it has at least one contact in the region. The maximum number of supporting zones is four. Molar and premolar contacts define the classification: Class A contains four support zones in the premolar and molar zones; Class B contains one to three support zones in the molar or premolar region or support in the frontal region only; and Class C is no occlusal contact, although there might be a few remaining teeth [Figure 1].[9] Interpretation of radiograph was done by principal investigator followed by research staff, Professor and Head of the Department in Oral Radiology with more than 30 years of teaching experience, An Oral Medicine and Radiology specialist (A Post graduate Degree in Dentistry). Decision was made after discussion and consensus between interpreters. The investigator analyzed the radiographs on a view box, in a dim light environment. The condyles were further classified into four groups according to their shape: (a) Flat, (b) pointed, (c) angled, and (d) round [Figure 2].[10]
![Examples of the original Eichner index (Eichner, 1955) in the natural dentition: Class A has four contacts in premolar or molar zones, Class B has 1–3 contacts in premolar or molar, or in the frontal zone only, and Class C has no contact.[6-8]](/content/12/2020/10/1/img/JCIS-10-51-g001.png)
![Examples of condyle outlines grouped, according to the shape as: (a) Flat, (b) pointed, (c) angled, and (d) round.[9]](/content/12/2020/10/1/img/JCIS-10-51-g002.png)
- Examples of condyle outlines grouped, according to the shape as: (a) Flat, (b) pointed, (c) angled, and (d) round.[9]
Data collection
The need and design of the study as well as potential benefits of undergoing clinical, radiographic investigations was explained and informed consent was obtained from the participants. The sociodemographic data and clinical settings of the persons fulfilling the criteria were recorded in a pre-designed and structured pro forma. All appropriate radiographs required for the diagnosis were taken. Clinically relevant variables were categorized and verified for analysis.
Data management
Data entry was done using SPSS version 18 for Windows. Clinically relevant variables were categorized and verified for analysis.
RESULTS
Panoramic radiographs of 350 subjects were included in the study, corresponding to a total of 700 mandibular condyles. The sociodemographic data and clinical settings of the individuals fulfilling the criteria were recorded in the pro forma. A single observer analyzed the radiographs on a view box, in a dim light environment. Findings in panoramic view and double TMJ view were taken for the final assessment. Search of available literature does not show any study which established the relationship between normal condylar morphology to dentition status and chewing habits of the individuals.
Demographic distribution of age
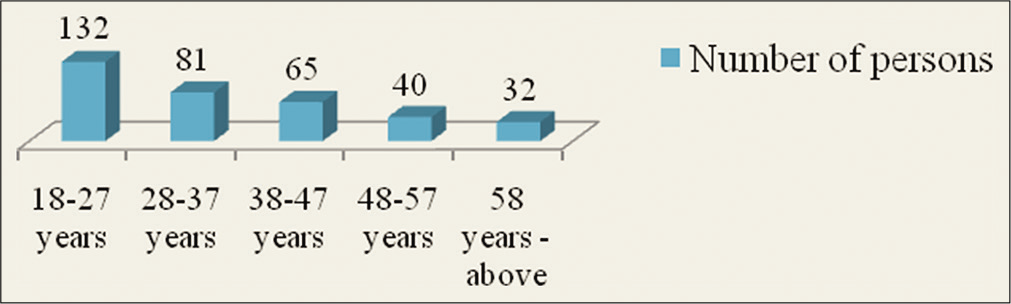
Persons above 18 years were selected for the study. The individuals were divided into five subgroups according to age. Majority of the persons belonged to the age group of 18–27 years, 132 persons (38%). Eighty-one persons (23%) were found to be in the age group 28–37 years. Sixty-five persons (18.6%) were found among the age group of 38–47. Forty individuals (11.4%) were found in the 48–57 age groups and in the 58 and above age group, there were 32 persons (9%) [Graph 1].
- Distribution of persons according to age.
Gender distribution
Out of total 350 individuals, 155 (44%) were male and 195 (56%) were female with a female-to-male ratio of 1.25:1.
Age and gender distribution
The maximum number of individuals was found in the age group of 18–27 years, 132 (38%) persons of which 58 (44%) were male and 74 (56%) were female and the least number of individuals in the age group 58 years and above, 32 persons (9%), of which 19 persons (59.4%) were male and 13(40.6%) were female [Table 1].
| Age groups | Gender | Total | |
|---|---|---|---|
| Male | Female | ||
| 18–27 | 58 | 74 | 132 |
| 28–37 | 30 | 51 | 81 |
| 38–47 | 27 | 38 | 65 |
| 48–57 | 21 | 19 | 40 |
| 58 and above | 19 | 13 | 32 |
Distribution according to dentition status
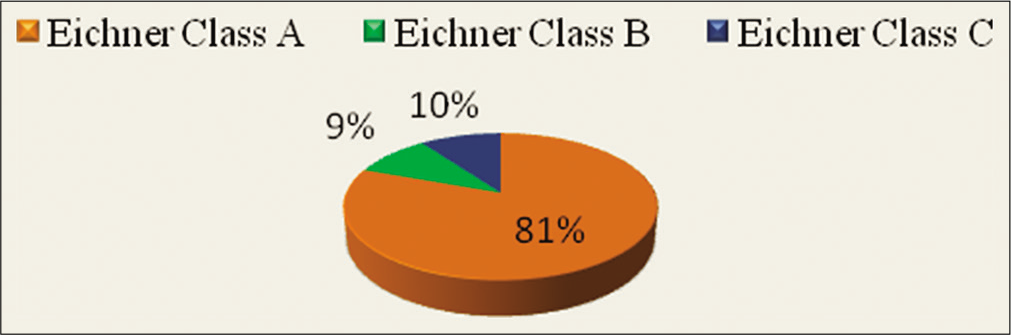
The dentition status among the individuals was further divided into three classes, Eichner Class A, Eichner Class B, and Eichner Class C. A total of 282 persons (81%) came under Eichner Class A, 33 persons (9%) under Eichner Class B, and 35 persons (10%) under Eichner Class C [Graph 2 and Figure 1].
- Dentition status of the study group.
Distribution of dentition status among age groups
A statistically significant relationship between age groups and dentition status was noticed (P = 0.00). As the age advances, the dentition status tends to move toward Eichner Class C [Table 2 and Figure 1].
| Age groups | Dentition status | Total | ||
|---|---|---|---|---|
| Eichner Class A | Eichner Class B | Eichner Class C | ||
| 18-27 | 129 | 3 | 0 | 132 |
| 28-37 | 65 | 10 | 6 | 81 |
| 38-47 | 46 | 9 | 10 | 65 |
| 48-57 | 26 | 6 | 8 | 40 |
| 58 and above | 16 | 5 | 11 | 32 |
| Total | 282 | 33 | 35 | 350 |
Distribution of dentition status according to age and gender
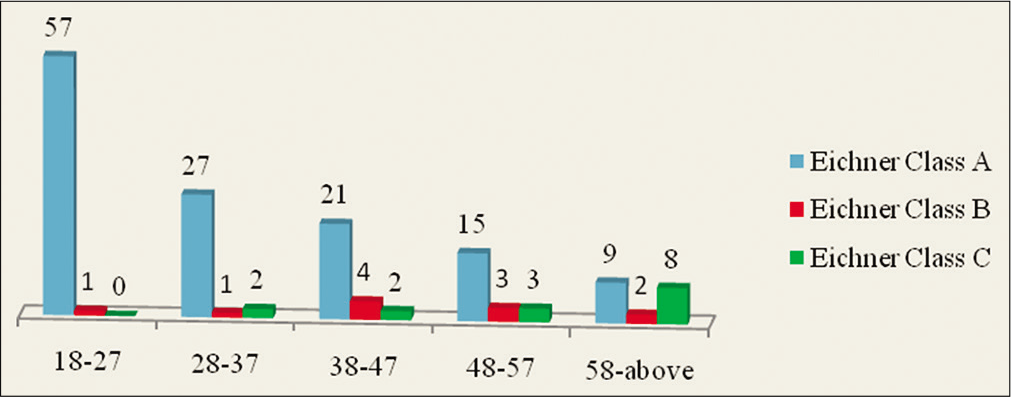
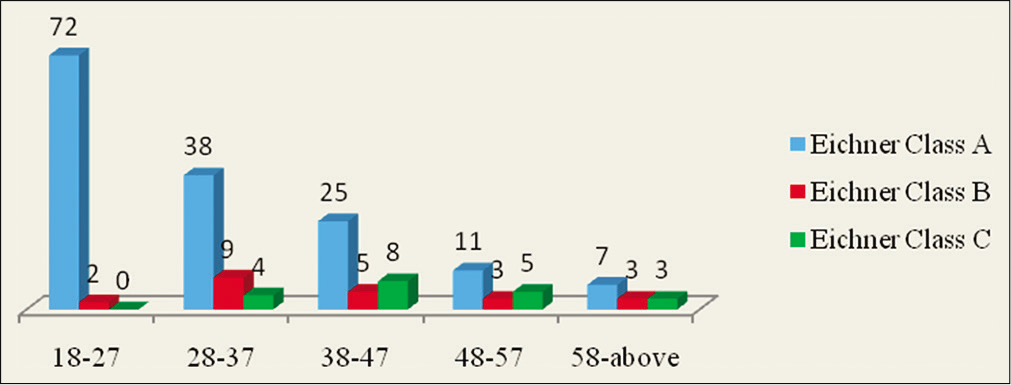
The maximum number of persons was found to have Eichner Class A, that is, 282 (81%) persons, among which 129 (45.7%) were male and 153 (54.3%) were female, with female-to-male ratio of 1.19:1. Eichner Class A was maximum in the age group of 18–27 years, 129 persons, out of them 57 persons, 44% were male and 72 persons, 56% were female [Graphs 3 and 4 and Figure 1].
- Age groups and dentition status in males.
- Age groups and dentition status in females.
Distribution according to parafunctional habits
Majority of the individuals had no parafunctional habits 317 (91%). Only 2 males (1%) had the habit of bruxism in the age group of 18–27 years. Nineteen persons (5%) had habit of clenching out of which seven were male and four females in the age group of 18–27 years. Twelve persons (3%) had habit of grinding, maximum being in the age group of 28–37 years with two males and females each [Graph 5].
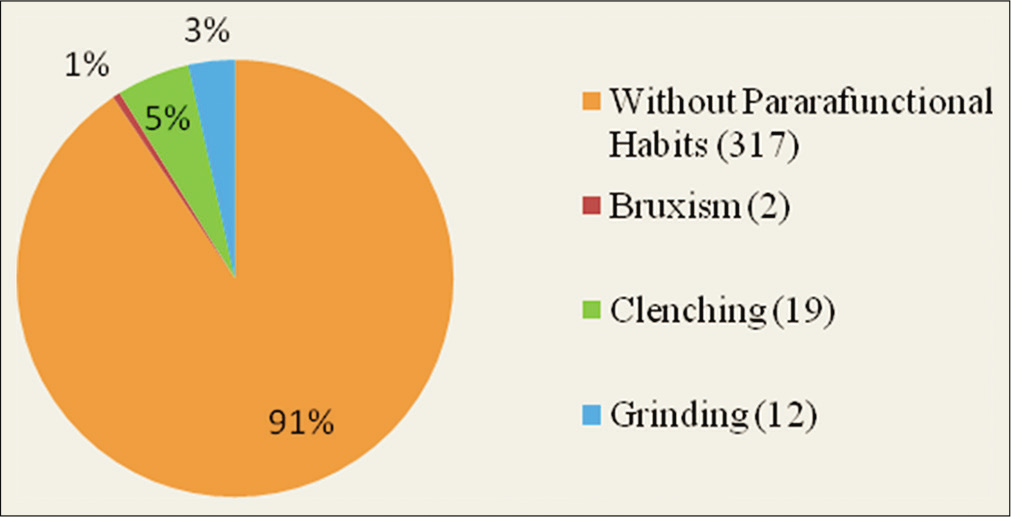
- Distribution according to parafunctional habits.
History of orthodontic treatment
Only 25 (7%) persons had the history of orthodontic treatment for mild malocclusion 10 of whom were male and 15 were female.
History of usage of denture
Out of 350 subjects, 26 (7.4%) had the history of wearing removable partial denture for maxillary anterior edentulism and there was no person wearing complete denture in the study group. Majority of the individuals wearing removable partial denture were found in the age group of 58 years and above, that is, 10 persons of which 8 were male and 2 were female [Graph 6]. There were no individuals wearing complete denture and removable partial denture below the age group of 28 years in the study subjects. The relationship between age groups and denture wearing history was found statistically significant (P = 0.00). This signifies that with denture usage in the older age groups, there is more likely chance for TMJ pathologies.
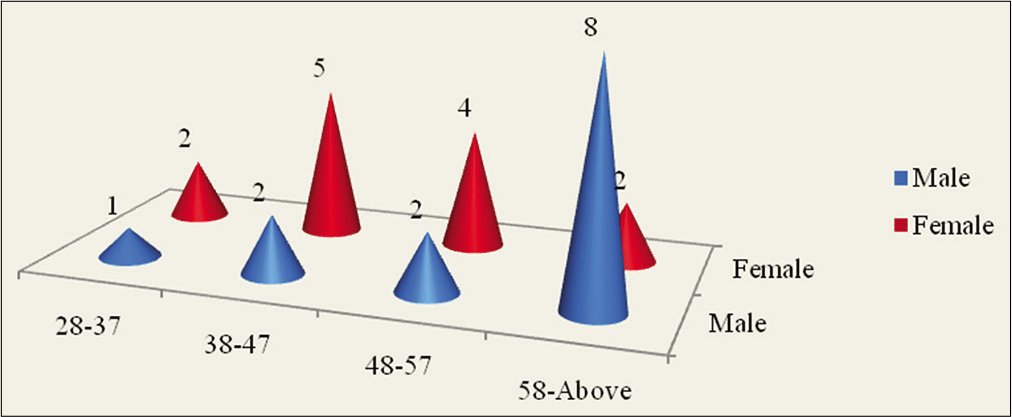
- Age and gender wise distribution of denture wearers (RPD).
Distribution according to chewing habits
Most subjects had no specific chewing habit 242 (69%). Ninety-three persons had bilateral chewing habit (27%). Unilateral chewing habit on the left side was found in 7 persons (2%) and unilateral right side chewing habit was in 8 persons (2%) [Graph 7]. Persons with bilateral chewing habits were found to be maximum in the age group of 18–27 years, that is, 49 persons out of which 24 persons were male and 25 were female. Least number of the individuals with bilateral chewing habits were in the age group of 58 years and above, that is, two persons unilateral left side chewing habit in the age group 18–27 years was found only in three persons out of which two were female, and among the age group of 48–57 years, two persons were female and one male, 58 years and above, no males had unilateral left side chewing habits.
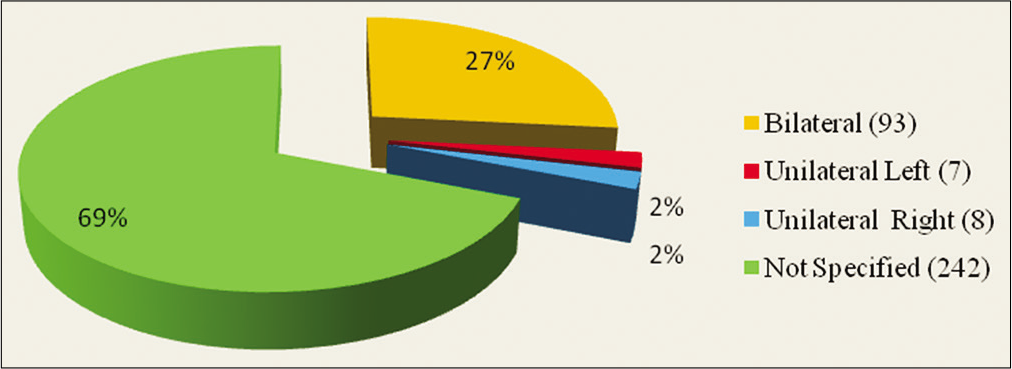
- Distribution according to chewing habit.
Unilateral right side chewing habits were found in 4 persons (50%) between the age group of 38–47.
Radiographic appearance of condyle
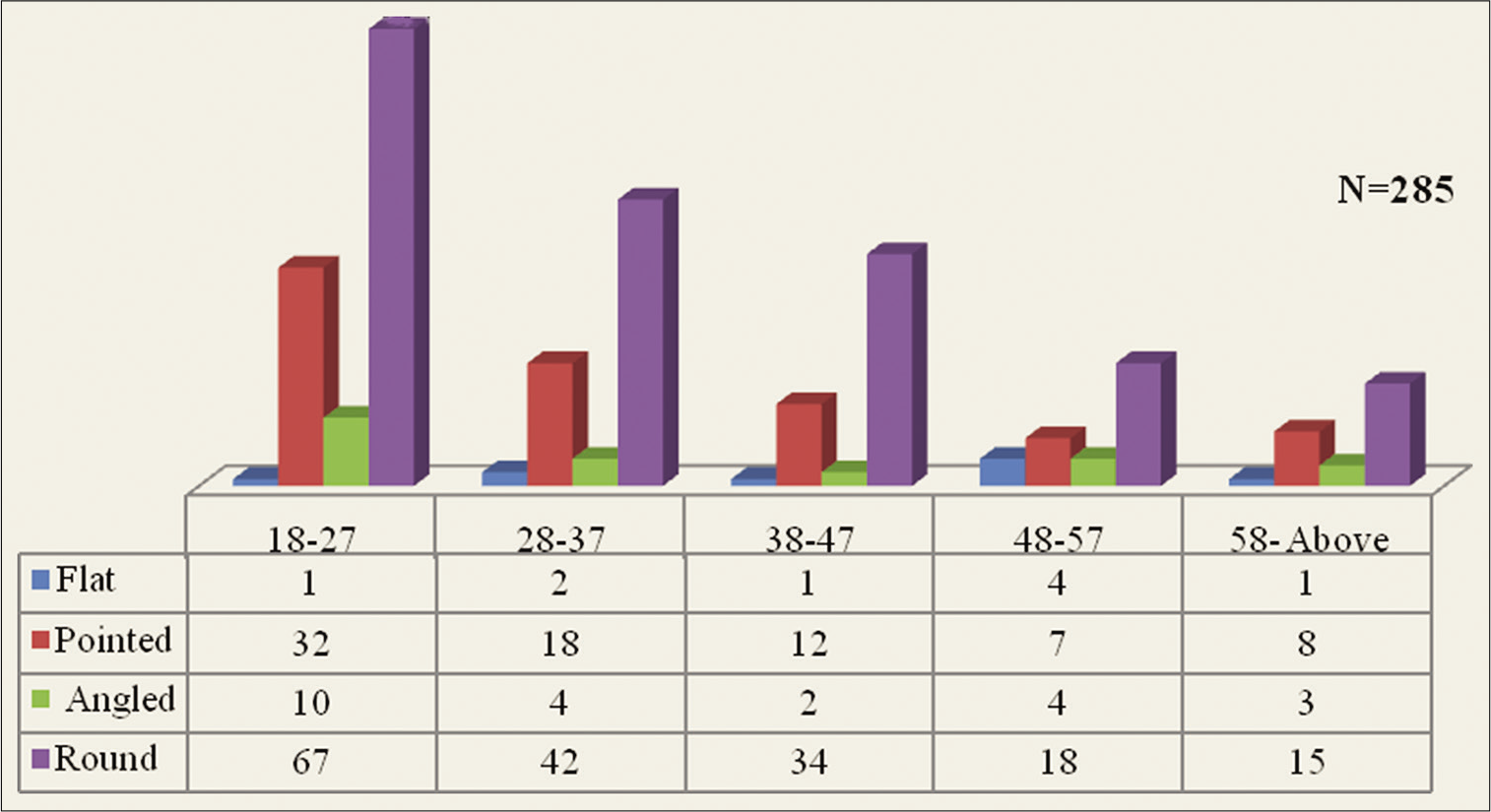
The bilateral occurrence of the same shape of the condyles represented four-fifth of the subjects 285 (81.4%) and 65 (18.6%) individuals had different shapes of each condyle.
Frequency of bilateral similar condyles
The variation among the condyle shapes in the study groups was divided into six types: Flat, pointed, angled, round, bifid, and other variations. The frequency of bilaterally similar flat- shaped condyle was found in 9 persons (3%) and pointed was found in 77 (27%), angled shaped was in 23 persons (8%), and round-shaped condyle was seen in maximum number of persons, 176 persons (62%) [Graph 8 and Figure 2].
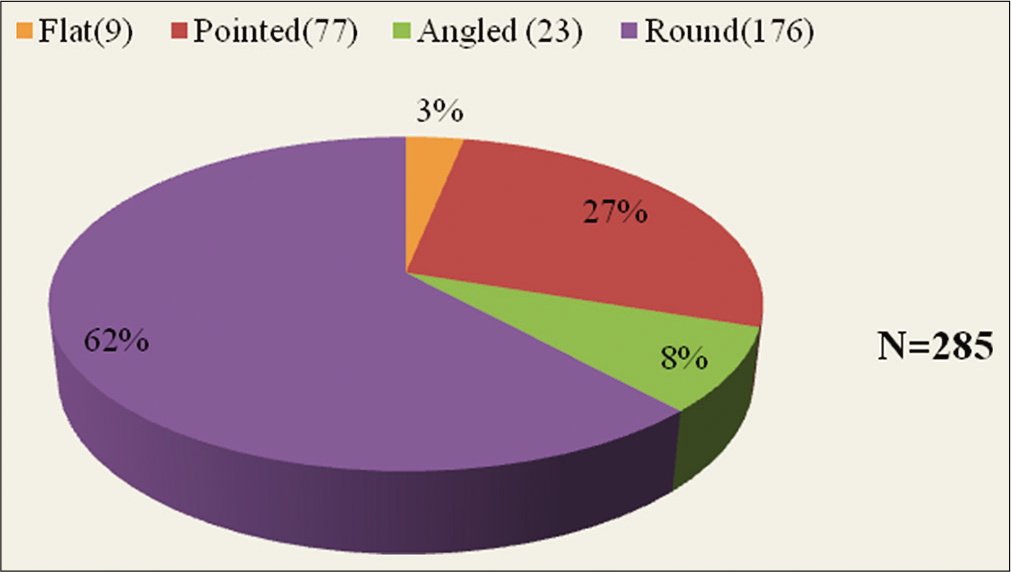
- Bilaterally similar shaped condyle: Frequency of shapes.
Frequency of dissimilar condylar shapes according to side
In the 65 individuals, with non-identical shaped condyles, pointed shaped condyle was seen in 25 persons (38.5 %) on the right and left side. Round-shaped condyle on the right side was found in 25 persons (38.5%), and the round- shaped condyle of the left side was seen in the 21 persons (32.3%), flat-shaped left condyle, in 2 persons (3%), and flat- shaped right condyle in 10 persons (15.4%). Angled shaped condyle on the right side was found in 5 persons (7.6%) and on the left was seen in 17 persons, that is, (26.2%). There was no bifid or other variation of condyle shape among the study group. Only four variations of condylar shapes, flat, pointed, angled, and round were seen in the study group [Graph 9].
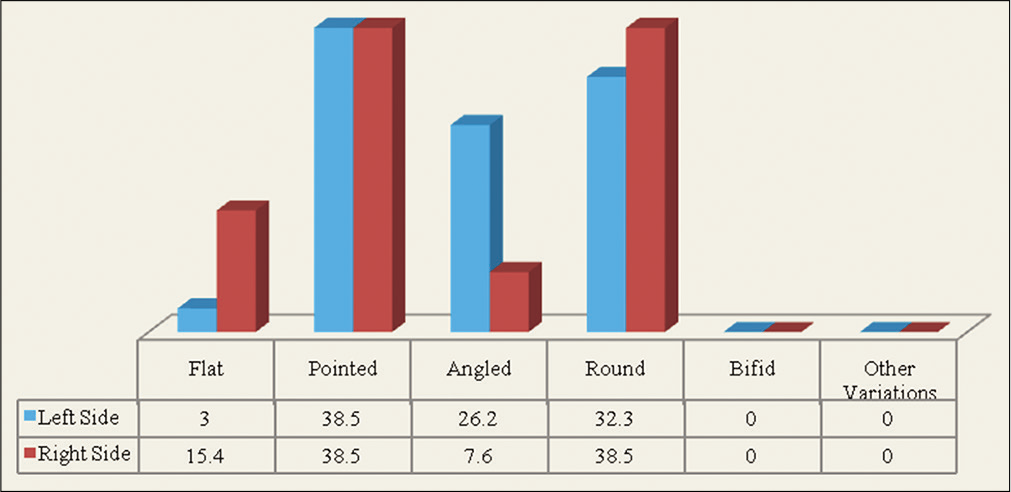
- Frequency of dissimilar condylar shapes according to side in percentage.
Correlation of bilaterally similar condyle shape with age groups
Bilaterally similar shape of the condyles was found to be maximum in the age group of 18–27 years, that is, 110 persons (38.5%), least were found among the age group of 58 and above, that is, 27 persons (9.5%) [Graph 10].
- Correlation of bilaterally similar shaped condyle with age groups.
Correlation of dissimilar shaped condyle with age groups
Majority of individuals in the age group of 18–27 years (83.33%) had bilaterally similar condyles. Dissimilar condyles were observed in only 16.67% of individuals. Among the age group of 58 and above, 15.6% had dissimilar condyles. The percentages of dissimilar condyles in the different age groups were almost similar. Overall dissimilar combinations of round right side and pointed left side condyle were found to be maximum, that is, 16 persons (25%). Combination of round right side, flat left side, angled right side, and round left side was seen least in the study group, that is, two persons in each (3%) [Graph 11 and Figure 2].
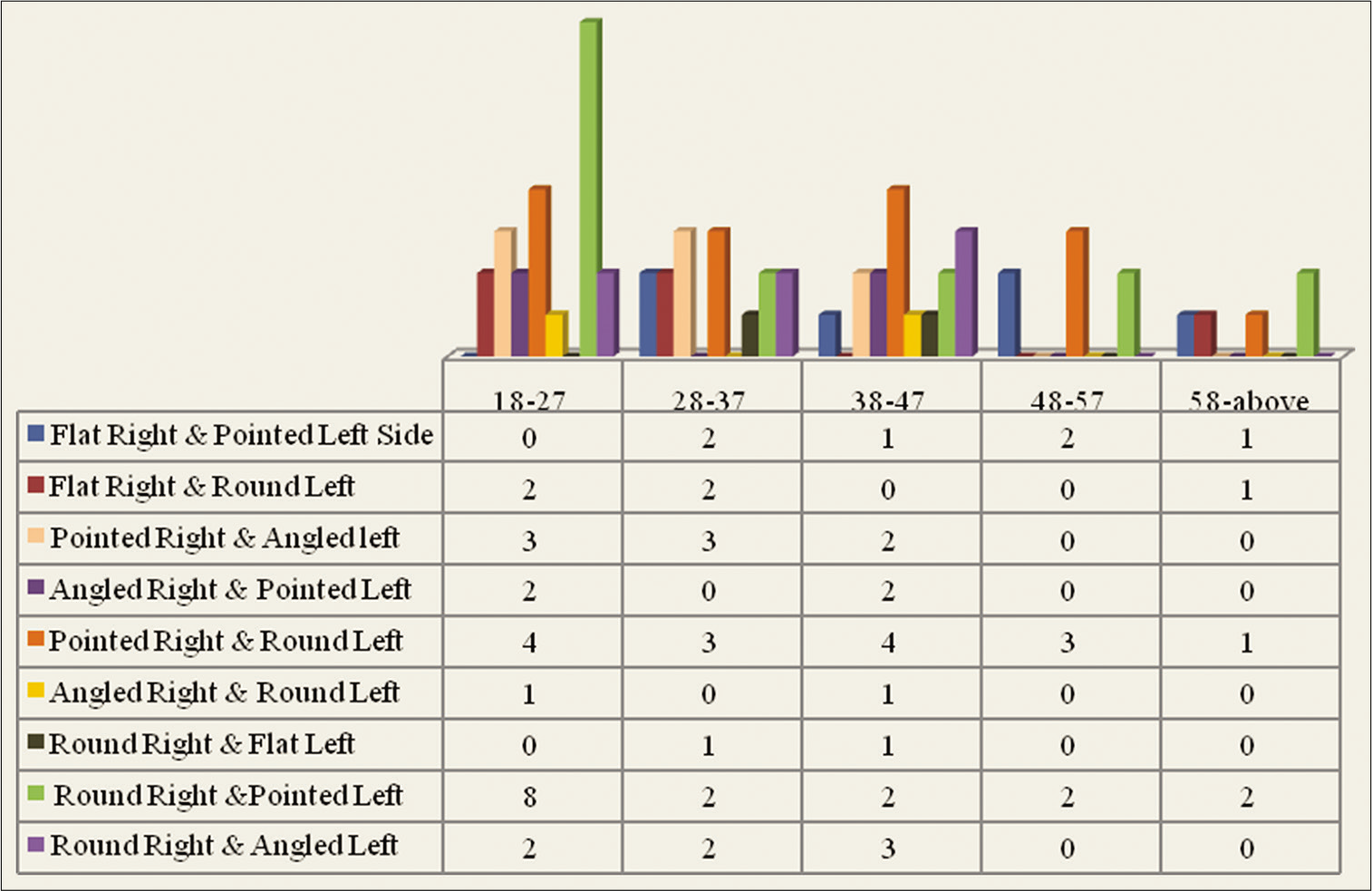
- Correlation of dissimilar shaped condyle with age groups.
Frequency of condylar shapes on the left side with age groups
A total of 132 individuals were found in the age group of 18–27 years, among which flat-shaped condyle was found in one person, pointed was found in 41 persons (31.1%), angled shaped was observed in 16 persons (12%), and round shaped in 74 persons (56.1%). Between the age group of 28–37 years, among 81 persons, flat shaped was found in 3 persons (4%), pointed was found in 22 persons (27%), angled was found in 9 persons (11%), and round was in 47 persons (58%). Among the age group of 38–47 years, 65 persons were observed. Out of these, flat-shaped condyle was found in 2 persons (3%), pointed in 17 persons (26%), angled shaped in 7 persons (11%), and round in 39 persons (60%). Within the age group of 48–57 years, among a total of 40 individuals, the flat-shaped condyle was found in 4 persons (10%), pointed in 11 persons (27.5%), angled in 4 persons (10%), and round in 21 persons (52.5%). In the age group of 58 years and above, a total of 32 persons were sighted out which flat- shaped condyle was found in 4 persons (12.5%), pointed in 1 person (3.1%), angled in 11 persons (34.4%), and round in 16 persons (50%). Round-shaped condyle, left side frequency, is more in every age groups and flat-shaped left was least in age groups of 18–27 years and 58 and above [Graph 12 and Figure 2].
- Frequency of condylar shapes on the left side with age groups.
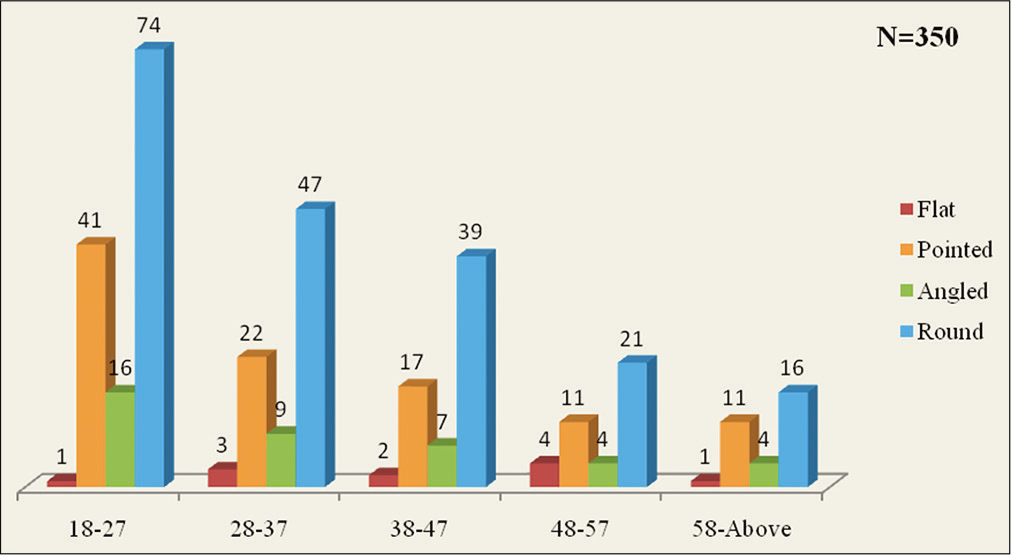
Frequency of condylar shapes on the right side with age groups
Out of the 132 individuals in the age group of 18–27 years, the frequency of flat-shaped condyle on the right side was found in 3 persons (2.3%), pointed was found in 40 persons (30.3%), angled shaped in 12 persons (9.1%), and round shaped in 77 persons (58.3%). Among the age group of 28–37 years, 81 were sighted of which flat shaped was found in 6 persons (7%), pointed shape was found in 24 persons (30%), angled was found in 4 persons (5%), and round shaped in 47 persons (58%). Among the age group of 38–47 years, which had 65 persons, 2 persons (3%) were found with flat-shaped condyle, pointed in 18 persons (28%), angled in 5 persons (8%), and round in 40 persons (61%). Within the age group of 48-57 years, 40 persons were found and of which the flat-shaped condyle on the right side was found in 6 persons (15%), pointed in 10 (25%), angled in 4 (10%), and round in 20 (50%). In the age group of 58 years and above, a total of 32 persons were seen, of which flat- shaped condyle was found in 2 persons (6.25%), pointed in 10 (31.25%), angled in 3 (9.4%), and round in 17 (53.1%). Round-shaped condyle on the right side is more in every age group, and flat-shaped right side was least in the age group of 38–47 years and 58 years and above [Graph 13 and Figure 2].
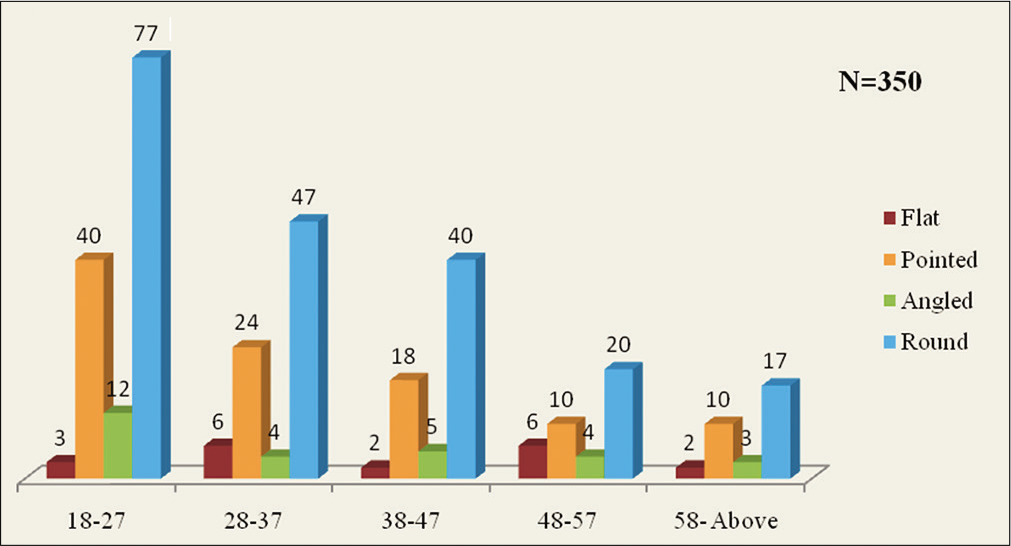
- Frequency of condylar shapes on the right side with age groups.
Association of condylar shapes with age and gender
Among the age group of 18–27 years, female-to-male ratio with bilateral same shapes of condyles was found to be 1.2:1, the male individuals were 49 and female 61, and in the age group of 28–37 years, females were 41 and males were 25. Between the age group of 38–47 years, female individuals were 29 and males were 20. Within the age group of 48–57 years, 15 individuals were female and 18 were male (0.8:1) and 58 years and above age group 11 were female and 16 males were found with bilateral similar shape condyles. Combinations of the non- identical condyle shapes were found in 65 subjects (18.5%), of which 27 individuals were male and 38 individuals were female and were found least in the age group (58 years and above) with a total of five persons, two females and three males [Figure 2].
Age- and gender-wise distribution of condylar shapes on the right side
Flat-shaped right condyle was not found among the female individuals in the age group of 38–47 years and 58 and above. The angled shaped right side condyle was not found among the male individuals in the age group of 48–57 years. Round shape of the right side condyle was found in 89 males (25.4%) and 112 females (32%). In all the age groups, round-shaped right condyle was found most commonly without the distinction of age and gender [Table 3 and Figure 2].
| Unilateral right | Age groups | Gender | |
|---|---|---|---|
| Male | Female | ||
| Flat | 18–27 | 2 | 1 |
| 28–37 | 3 | 3 | |
| 38–47 | 2 | 0 | |
| 48–57 | 3 | 3 | |
| 58 and above | 2 | 0 | |
| Pointed | 18–27 | 12 | 28 |
| 28–37 | 11 | 13 | |
| 38–47 | 7 | 11 | |
| 48–57 | 6 | 4 | |
| 58 and above | 7 | 3 | |
| Angled | 18–27 | 7 | 5 |
| 28–37 | 1 | 3 | |
| 38–47 | 2 | 3 | |
| 48–57 | 0 | 4 | |
| 58 and above | 1 | 2 | |
| Round | 18–27 | 37 | 40 |
| 28–37 | 15 | 32 | |
| 38–47 | 16 | 24 | |
| 48–57 | 12 | 8 | |
| 58 and above | 9 | 8 | |
Age- and gender-wise distribution of condyle shapes on the left side
Flat-shaped condyle on the left side was also not found in the age group of 38–47 years and 58 years and above among the female individuals. The flat-shaped left condyle was not found in male individuals among the age group of 18–27 years and also the left side angled shaped condyle was not found in the age group of 48–57 years in male individuals as resulted on the angled shaped right side. Nearly similar result was found for the round shape and pointed shape as on the right side round without the significant distinction of age and gender [Table 4 and Figure 2].
| Unilateral left | Age groups | Gender | |
|---|---|---|---|
| Male | Female | ||
| Flat | 18–27 | 0 | 1 |
| 28–37 | 2 | 1 | |
| 38–47 | 2 | 0 | |
| 48–57 | 2 | 2 | |
| 58 and above | 1 | 0 | |
| Pointed | 18–27 | 16 | 25 |
| 28–37 | 9 | 13 | |
| 38–47 | 5 | 12 | |
| 48–57 | 5 | 6 | |
| 58 and above | 8 | 3 | |
| Angled | 18–27 | 8 | 8 |
| 28–37 | 3 | 6 | |
| 38–47 | 4 | 3 | |
| 48–57 | 0 | 4 | |
| 58 and above | 2 | 2 | |
| Round | 18–27 | 34 | 40 |
| 28–37 | 16 | 31 | |
| 38–47 | 16 | 23 | |
| 48–57 | 14 | 7 | |
| 58 and above | 8 | 8 | |
Correlation between dentition status and condylar shapes
There was statistically significant association between dentition status and condylar morphology (P = 0.02). A total of 285 individuals with bilaterally similar shape condyles were found in the study group, of which 227 (79.6%) persons were having the Eichner Class A, with bilateral round shaped condyles in 146 persons (64.3%). Flat-shaped condyle was found in the 4 persons (1.7%), which is least, pointed shape was found in 61 persons (27%) and angle shaped was in 16 persons (7%). In the Eichner Class B, 28 persons (9.8%) were found with bilaterally similar condyles, out of which flat- shaped condyle was found in 1 person (4%), pointed was in 6 (21%), angled was in 4 (14%), round-shaped condyle was in 17 (61%), and in 5 persons (8%), non-identical condyles were found. In Eichner Class C, 30 persons (10.5%) were found with bilaterally similar condyles, of which flat was in 4 (13.3%), pointed was in 10 (33.3%), angled was in 3 (10%), round shaped was found in 13 (43.3%), and combinations of non-identical shaped condyles were found in 5 persons (8%). Bilaterally round-shaped condyles were found more in the persons with dentition status Eichner Class A, than Eichner Class B and Eichner Class C. As the dentition shifted to Eichner B and Eichner C, the condylar morphology appeared to be altered [Graph 14 and Figures 1-7].
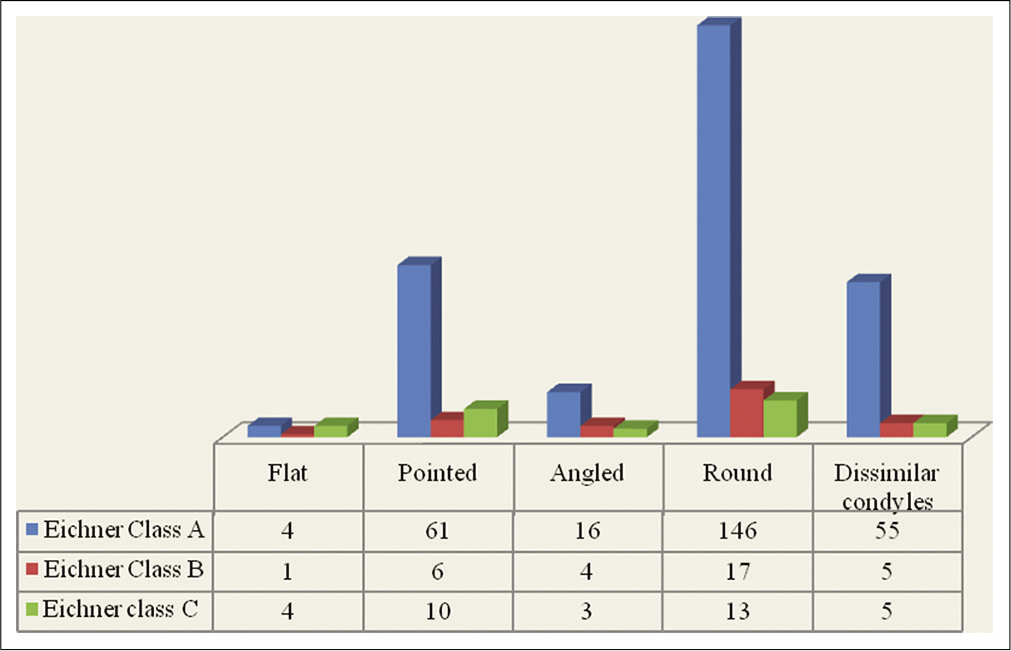
- Correlation between dentition status and condylar shapes.
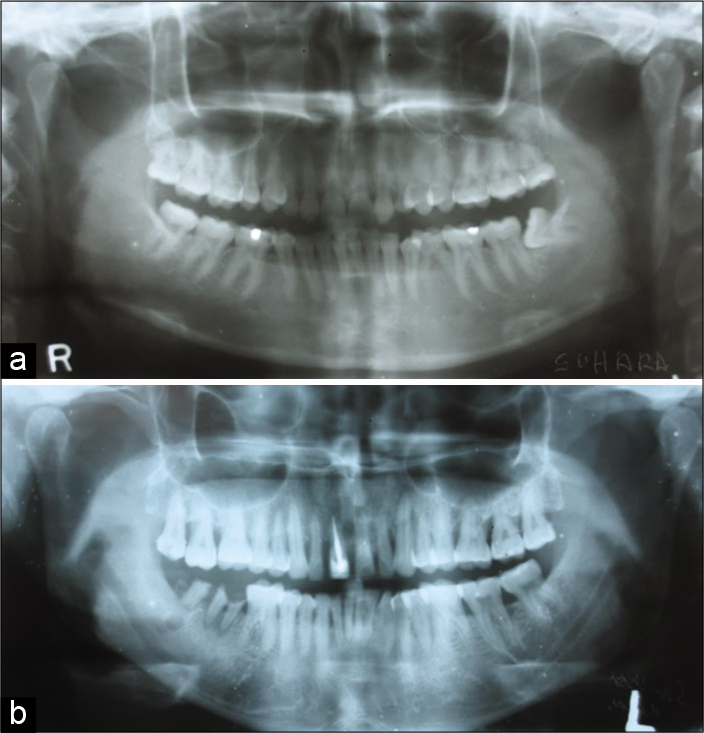
- (a and b) Panoramic view shows bilaterally pointed shaped condyles with Eichner Class A (e.g., Figure 1a and 2b).
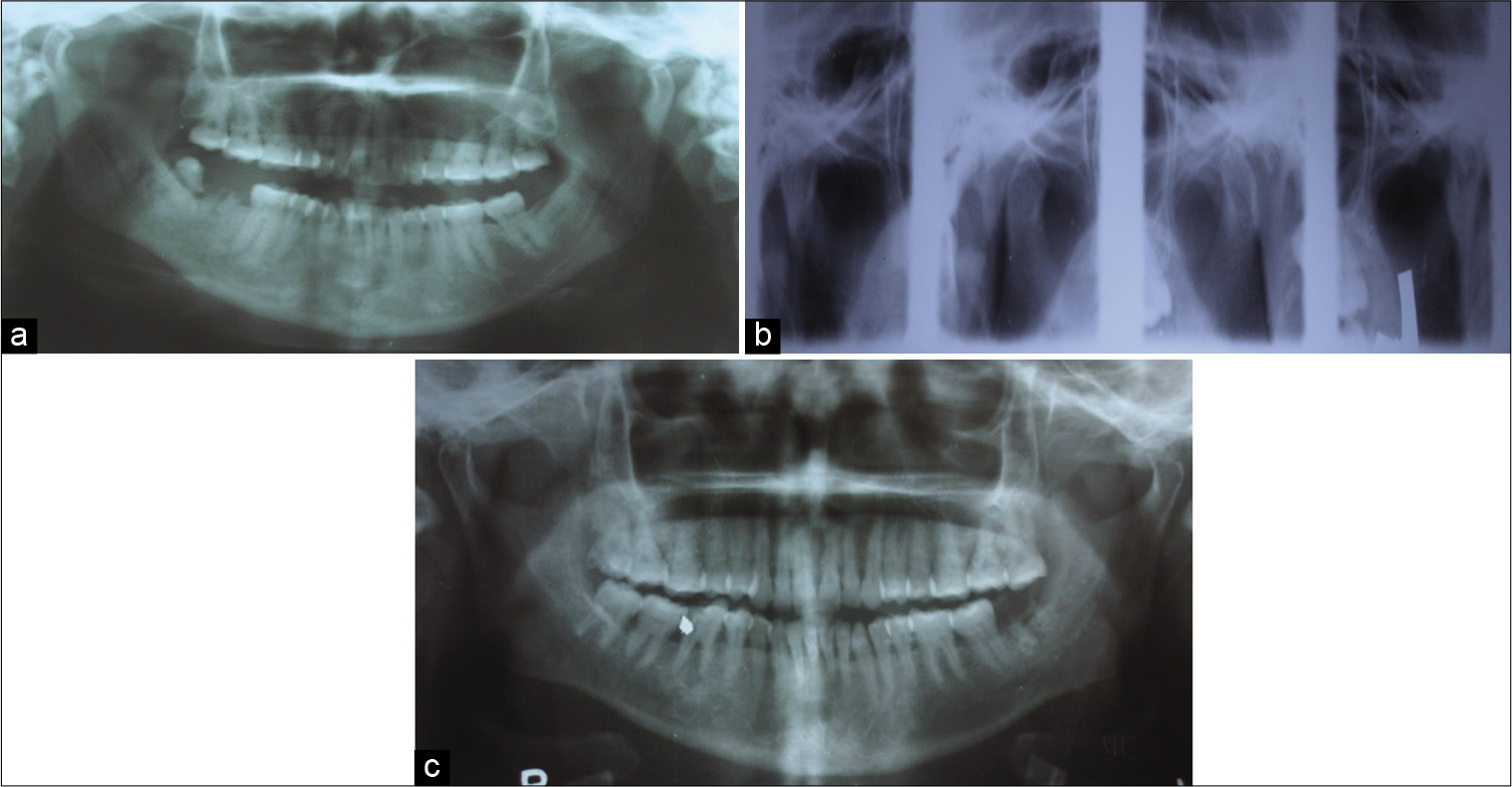
- (a) Panoramic view shows bilaterally flat shaped of condyles with Eichner Class A (e.g., Figure 1a and 2a). (b) Double temporomandibular joint view showing flat-shaped condyles (e.g., Figure 2a). (c) Panoramic view shows bilaterally flat-shaped condyles with Eichner Class A (e.g., Figure 1a and 2a).

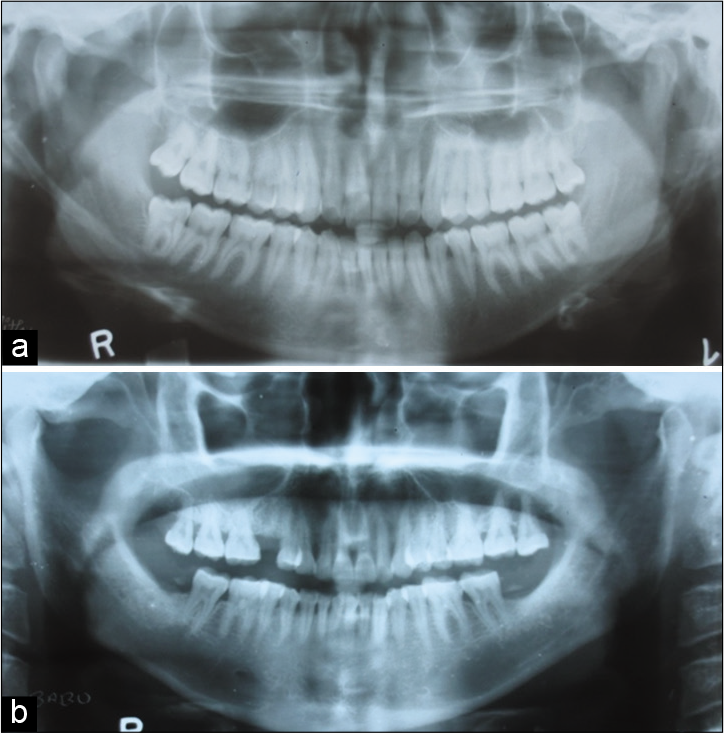
- Panoramic view shows bilaterally angled shaped condyles with Eichner Class B (e.g., Figure 1b and 2c).
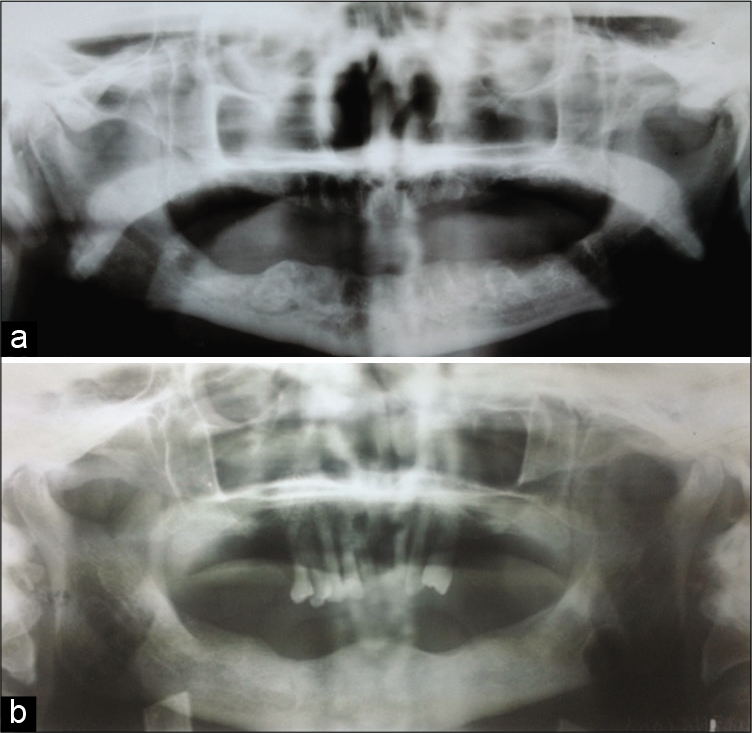
- (a) Panoramic view shows bilaterally pointed shaped condyles with Eichner Class C (e.g., Figure 1c and 2b). (b) Panoramic view shows bilaterally round-shaped condyles with Eichner Class C (e.g., Figure 1c and 2d).
Association between dentition status and bilateral similarly shaped condyles
The statistically significant relationship between the dentition status and bilaterally similar shaped condyles (P = 0.016) was observed. A total of 285 (81.4%) individuals were having bilateral same shaped condyles. Among them, 227 persons were found in the Eichner Class A (79.6%), 28 persons in Eichner Class B (9.8%) and 30 persons in Eichner Class C, that is, 10.5%. As the dentition status shifted to Eichner Class B and C, the frequency of round-shaped condyle was decreased, that is, 64.3%, 61%, and 43.3%, respectively [Figures 1-7].
Dentition status with dissimilar condyle shapes
A total of 282 persons had Eichner Class A, of which 55 persons (19.5%) were found with dissimilar condyle. Of the 33 persons who had Eichner Class B, 5 persons (15.15%) had dissimilar condyles. Out of 35 persons with Eichner Class C, 5 persons (14.3%) were found with dissimilar condyles. The distributions of individuals with dissimilar condyles were numerically similar in all the Eichner classes [Figures 1,8-10].
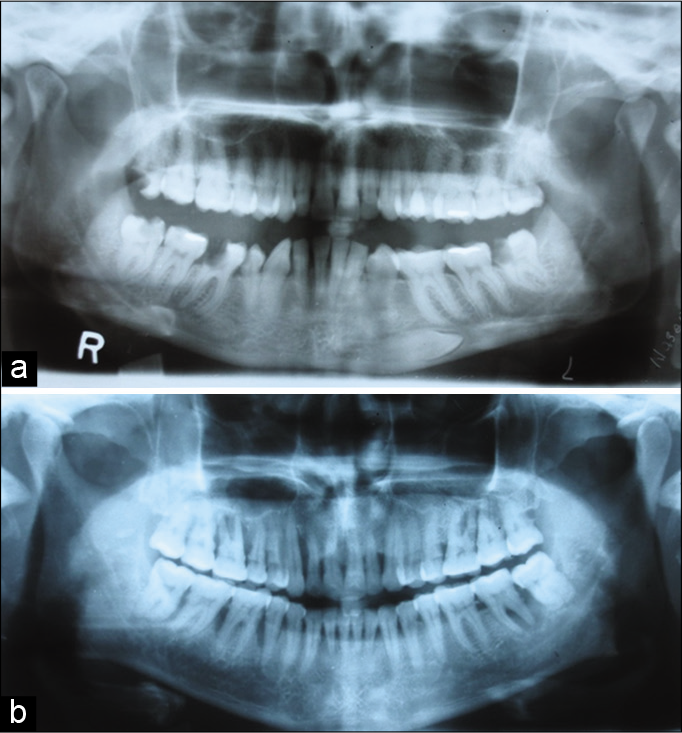
- (a) Panoramic view shows angled shaped right and round- shaped left side condyle with Eichner Class A (e.g., Figure 1a and 2c and d). (b) Panoramic view shows pointed shaped right and round-shaped left side condyle with Eichner Class A (e.g., Figure 1a and 2b and d).
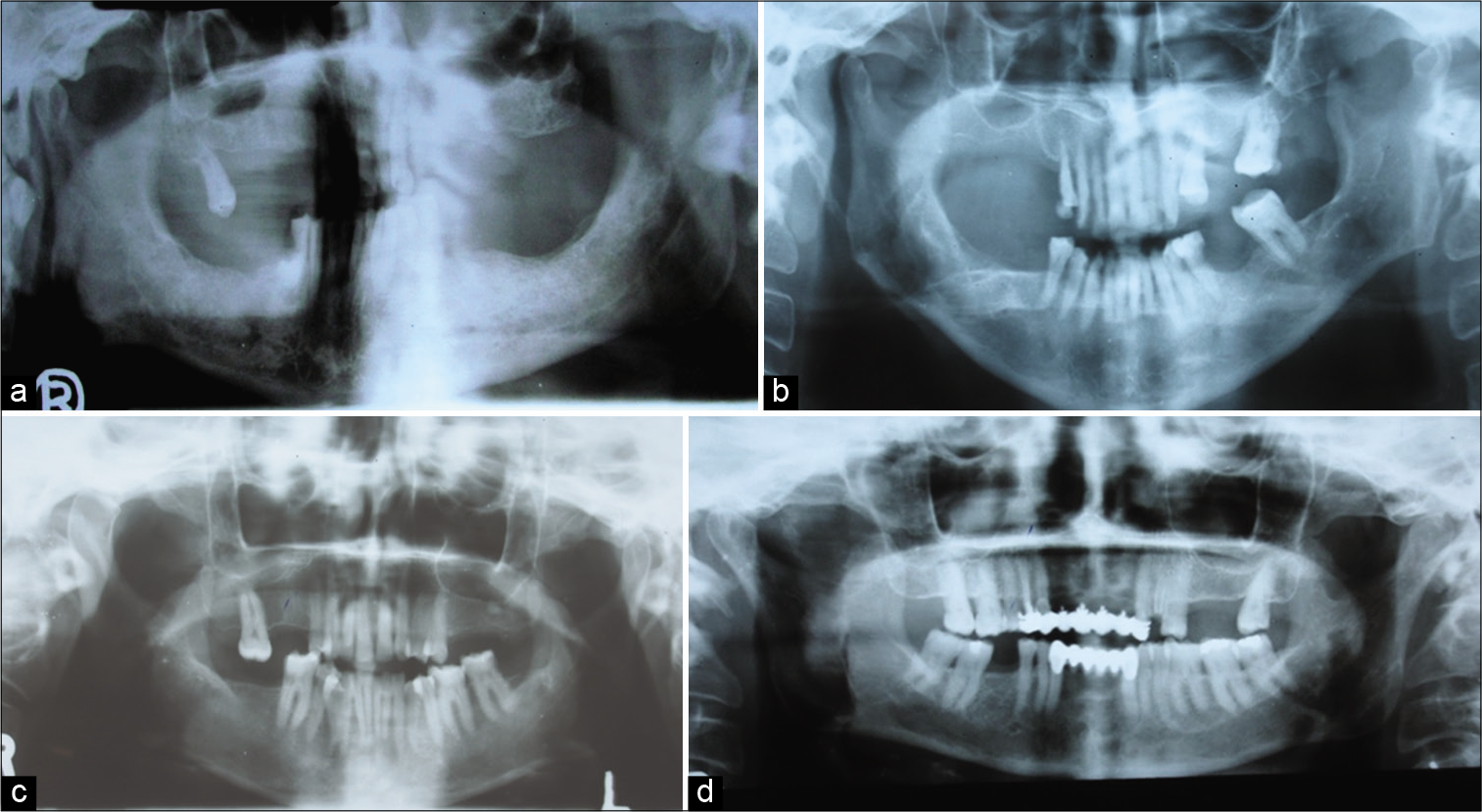
- (a) Panoramic view shows round-shaped right and pointed shaped left side condyle Eichner Class B (e.g., Figure 1b and 2d and b). (b) Panoramic view shows pointed shaped right and angled shaped left side condyle Eichner Class B (e.g., Figure 1b and 2b and c). (c) Panoramic view shows flat-shaped right and pointed shaped left side condyle Eichner Class B (e.g., Figure 1b and 2a and c). (d) Panoramic view shows angled shaped right and round-shaped left side condyle Eichner Class B (e.g., Figure 1b and 2c and d).
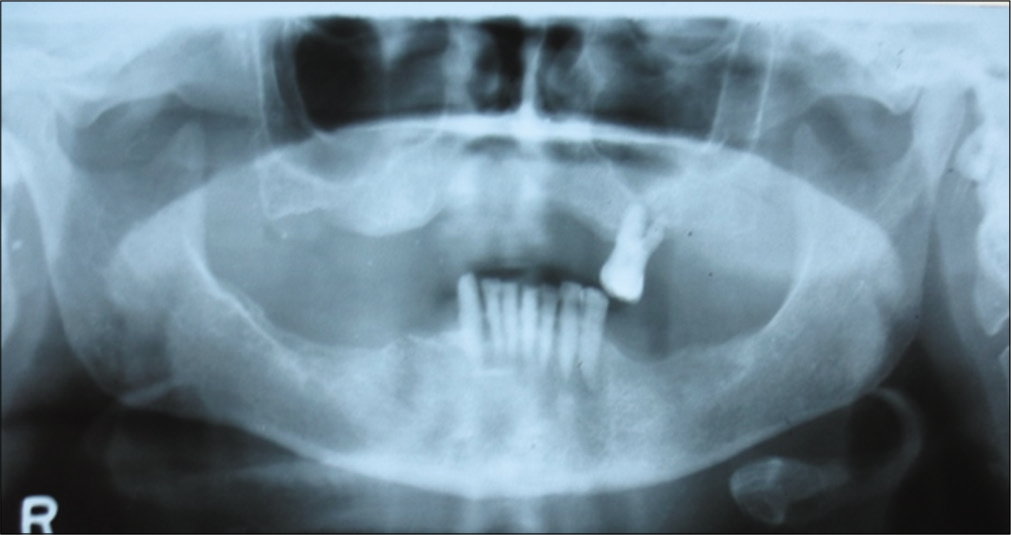
- Panoramic view shows round-shaped right and pointed shaped left side condyles with Eichner Class C (e.g., Figure 1c and 2d and b).
Dentition status with dissimilar shaped condyle frequency according to side
Combinations of round-shaped right side with pointed shaped left side were found maximum in the Eichner Class A, that is, 13 persons (20%). Angled shaped right side with round-shaped left and round-shaped right side with flat left side was observed in 2 persons each (3%). Pointed right and angled left side was found to be least 1 (1.5%) [Graph 15 and Figures 1,8-10].
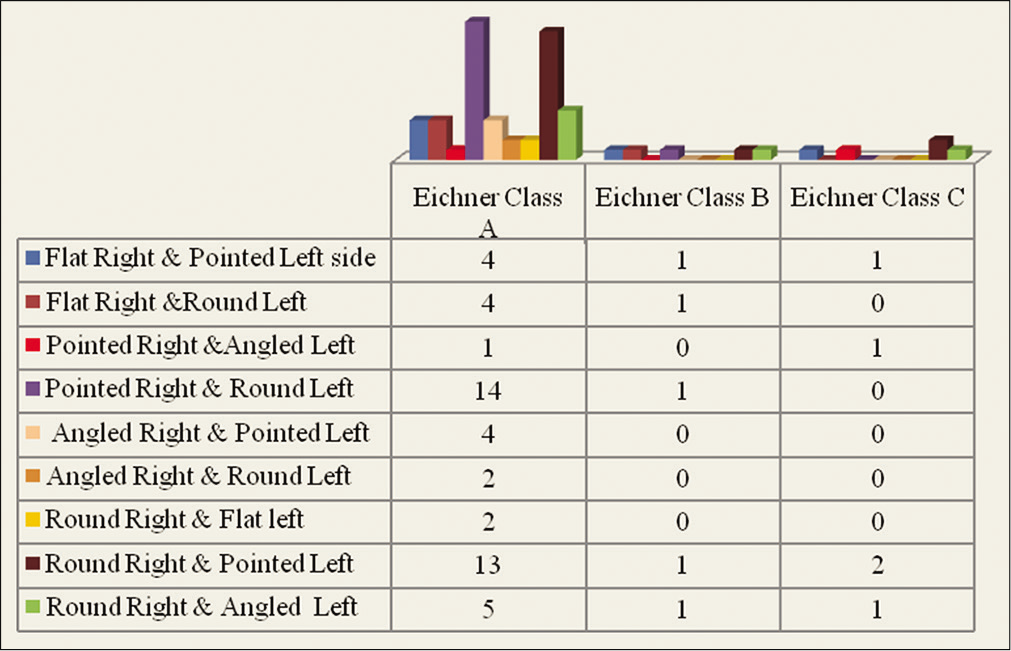
- Distribution of dissimilar condyles according to dentition status.
Frequency of condylar shapes on the right side with dentition status
A total of 282 individuals (80.5%) with the dentition status Eichner Class A were seen. Flat-shaped condyle in the Eichner Class A was 11 persons, (4%). Pointed shape was found in 84 subjects (30%), angled shape was in 21 (7%), and round shape was in 166 subjects (59%). In the Eichner Class B, 33 (9.5%) persons were observed and the frequency of the flat shape condyle on the right side was in 3 persons, pointed in 7, angled in 4, and round in 19 with percentage of 9%, 21%, 12%, and 58%, respectively. Thirty-five (10%) individuals were found under Eichner Class C, out of which 5 persons (14%) with flat shaped, 11 persons (31.4%) pointed shaped, 3 persons (8.6%) angled shaped, and 16 persons (46%) round shaped. The shape of the condyle on the right side with the dentition status was found statistically significant (P = 0.00). The round-shaped condyles on the right side were found more among the persons with dentition status Eichner Class A. This frequency was found to be decreased as the dentition status was shifted to Eichner Class B and Eichner Class C [Graph 16 and Figures 1,2,8-10].
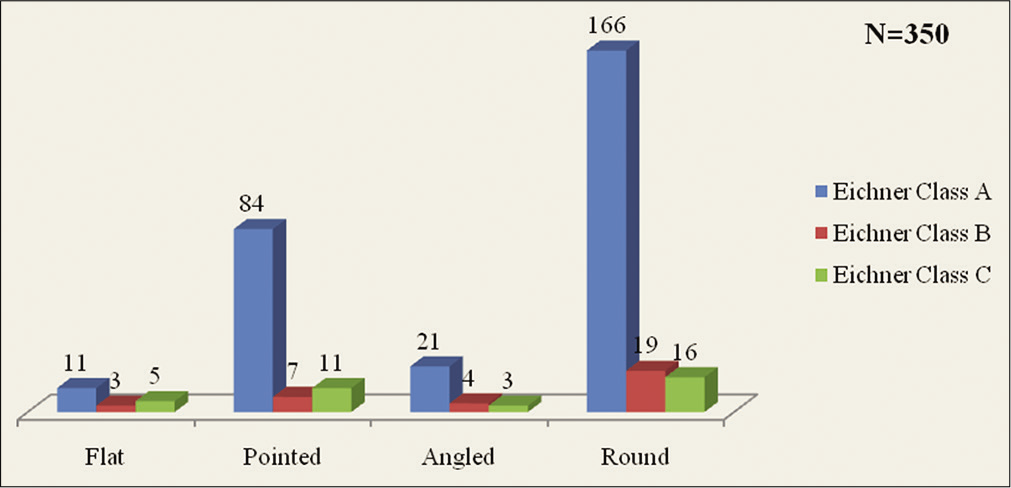
- Frequency of condylar shapes on the right side with dentition status.
Frequency of condylar shapes on the left side with dentition status
A total of 282 individuals (80.5%) with the dentition status Eichner Class A were seen, out of them flat-shaped condyle was in 6 persons (2%), pointed was in 81 (29%), angled was in 30 (11%), and round shape was in 165 (58%) belonged to dentition status Eichner Class A. Among the Eichner Class B, 33 persons were seen and the flat shape was found in 1 (3%), pointed was in 8 (24%), angled was in 5 (15%), and round shaped in 19 persons (58%). Thirty-five persons were sighted in Eichner Class C, among which 4 persons (11.4%) with flat- shaped condyle, 13 persons (37.3%) were pointed, 5 angled (14.3%), and 13 persons (37.3%) had round-shaped condyle. The shape of the condyle on the left side with the dentition status was found statistically significant (P = 0.04). Round- shaped condyle on the left side was found more in Eichner Class A. The prevalence of round shape condyle on the left side was found to be decreased as the dentition status shifted to Eichner B and Eichner C [Graph 17 and Figures 1,2,8-10].
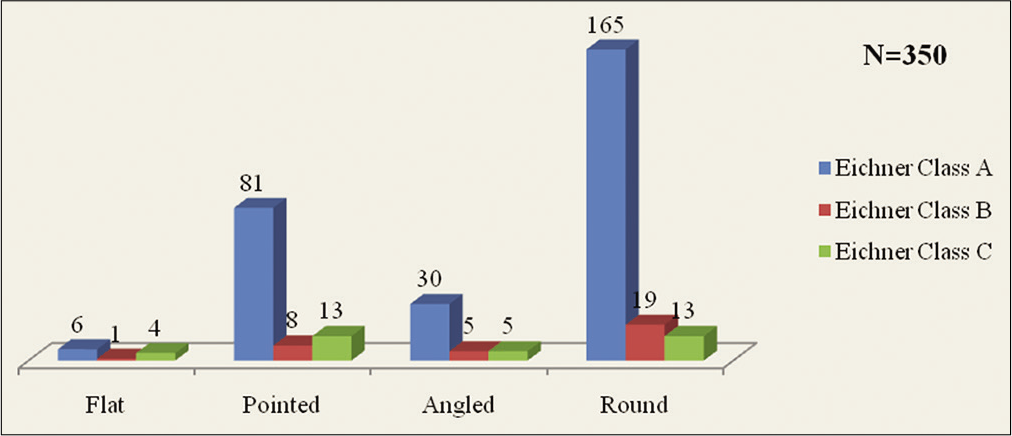
- Frequency of condylar shapes on the left side with dentition status.
Correlation between bilaterally similar shape of condyles with chewing habits
Statistically significant relationship (P = 0.003) was seen between chewing habits and bilaterally similar condyle shape. Majority of person had no specified chewing habits with bilaterally round-shaped condyles 120 (68%), followed by bilateral chewing habit 51 person (29%) and unilateral left side 2 persons (1%) and unilateral right side chewing habit in 3 persons (2%). Round shaped was observed more with the individuals whose chewing habits were not specified and those with bilateral chewing habits [Table 5 and Figure 2].
| Condylar shapes | Chewing habits | Total | |||
|---|---|---|---|---|---|
| Bilateral | Unilateral left | Unilateral right | Not specified | ||
| Flat | 2 | 1 | 0 | 6 | 9 |
| Pointed | 20 | 2 | 2 | 53 | 77 |
| Angled | 3 | 0 | 0 | 20 | 23 |
| Round | 51 | 2 | 3 | 120 | 176 |
| Total | 76 | 5 | 5 | 199 | 285 |
Correlation between condylar shapes with parafunctional habits
All persons with parafunctional habits had dissimilar condyles. The stability of condyles could be altered due to the parafunctional habits. These persons need to be followed up to see if they are likely to become symptomatic [Figures 2,8-10].
Association between condylar shapes and history of orthodontic treatment
Only 25 persons had a history of orthodontic treatment for mild malocclusion of whom 3 persons (12%) had dissimilar condyles.
Association between condylar shapes and history of usage of denture
Twenty-six persons had a history of usage of denture (removal partial denture) of whom 3 persons (11.5%) had dissimilar condyles [Figure 2]. The condylar morphology in a larger population of denture wearers needs to be studied to ascertain whether dentures can alter condylar morphology on prolonged usage.
DISCUSSION
Specific anatomic components of the TMJ include the mandibular condyle, the mandibular fossa and articular eminences of the temporal bone, and the soft-tissue components of the articular disk, its attachments, and the joint cavity.[1] The condyle presents an articular surface for articulation with the articular disk of the TMJ.[11] Mandibular condyle varies considerably both in size and shape. Oliveira-Santos et al. observed and outlined the condyles, which were classified into four groups, according to their shape: (a) Flat, (b) pointed, (c) angled, and (d) round. It was also recorded whether the same shape appeared bilaterally or different shapes were seen within each subject [Figure 2].[10]
Panoramic radiography is a simple, low-cost method to evaluate the bony structures of the TMJ and is one of the most commonly used techniques by dentists and dental specialists. Its principle is based on the tomographic concept of imaging a section of the body while blurring images outside the desired plane so that the TMJ and teeth are in focus, but adjacent structures are blurred. The use of panoramic radiographs and double TMJ views is justified by its small dose of radiation, low cost and for providing sufficient information of TMJ morphology. Although structural changes are thought to be related to TMJ dysfunctions, the changes affected by chewing habits, parafunctional habits, denture usage in older individuals, and loss of dentition have to be correlated.
In this study, the age groups of the individuals ranged from 18 years onward which were divided into five groups. This was nearly similar to Oliveira-Santos et al.[10] where they had taken subjects above 20 years with division of five age groups in their study in Bauru School of Dentistry at University of São Paulo. The current results showed that the bilateral occurrence of the same shape of the condyles represented four-fifth of the subjects, however, this frequency was found to be nearly two-thirds of the subjects in the study by Oliveira-Santos et al.[10] The highest prevalence of bilateral occurrence of the same shape was in the youngest group and the lowest prevalence in the oldest group. Similar findings were noticed by Oliveira et al.[10] and Sahithi et al.[12]
In the present study, round-shaped condyle (57%) was the most common morphology followed by pointed shaped (29%) and angled shaped (10%). Oliveira-Santos et al.[10] and Sahithi et al.[12] also observed in their study, round shaped was the most frequent shape. They found that angled shaped was second most prevalent condylar shape which was not in accordance with this study. Flat condyles were seen in 4% of the sample which was least common morphology, which was again accordance with the study of Oliveira-Santos et al.[10] and Sahithi et al.[12] However, Sahithi et al.[12] obtained these findings in their retrospective study using digital panoramic radiography for 200 subjects from the Department of Oral Medicine and Radiology, Vishnu Dental College and Hospital, Bhimavaram, Andhra Pradesh, India, and also the classification of condyles was not accordance with the ongoing study. They classified the condyle shape as round, angled, convex, and flat.
Ribeiro et al.[13] observed in their study the distribution of condyle and fossa shapes showed greater frequency of the rounded shape in the lateral (57% and 66%, respectively) and posterior (53% and 83%, respectively) views. There was no significant association between condylar morphology and age groups in the present study. On the contrary, Oliveira-Santos et al.[10] obtained a significant association between two.
When the distribution of condylar shapes among right and left sides was assessed independently in the present study we observed that the shape of condyle frequently observed was round (398), of which 201 (50.5%) were on the right and 197 (49.5%) on the left side. The next observed shape was pointed (204) that was equally seen on both the sides, followed by angled shape (68), that is, 28 (41%) on the right side and 40 (59%) on the left side. The flat shape (30) of the condyles was least observed with 19 (63.3%) and 11 (36.7%) on the right and left sides, respectively [Figure 2]. This surveillance was again in compliance with the study of Oliveira-Santos et al.[10] and Sahithi et al.[12] except for the angled shaped condyle which was their second most sequent shaped after the round-shaped condyle.
The frequency of flat condyles among symptomatic individuals should be determined to affirm any relation to pathological conditions. In a study by Takayama et al., the prevalence of bone change in the condyle (e.g., erosion, osteophyte, and deformity) was compared between patients with and without TMJ disorders.[14] Bone alterations were seen in 11.6% of dental patients (without symptomatology) and 17.7% of TMD patients. They found that the difference was statistically insignificant, it showed that even among TMD patients, those with bone changes were few, and most patients were confirmed to have the disease state even without bone loss. Condylar deformity was nearly as common among TMD and dental patients. No correlation of bone alterations with sex, age, dental, or occlusal conditions was demonstrated.[14]
Female-to-male ratio was 1.25:1 in the current study. Oliveira-Santos et al.[10] and Sahithi et al.[12] also found female preponderance in their study, whereas Ribeiro et al.[13] had found male preponderance in their study of adult human skulls belonging to Museum of Anatomy Collection of the Federal University of Sao Paulo – Paulista School of Medicine (UNIFESP-EPM).
In the current study, among the age group of 18–27 years, female-to-male ratio with bilateral same shapes of condyles was found to be 1.2:1 which was most and least were found in the age group of 58 and above with ratio of ratio of 0.7:1. The difference between males and females in relation to frequency of the morphologic groups in the current study was not statistically significant. Similar results were obtained by Ribeiro et al.[13] However, Yale et al. in 1966 noted that a convex superior aspect was more common in males than in females. They also noted a higher frequency of the convex shape in women than in men, whether seen from the lateral perspective (100.00% vs. 88.33%) or from the anterior perspective (37.50% vs. 18.33%). Researchers of this study concluded that fuller condyles in females may be suggestive of lesser mechanical stress of occlusion, due to lesser muscle mass, thereby causing retention of the initial convex shape of the condyle.[15] This conclusion was in agreement with the study done by Raustia and Salonen according to whom, the electromyogram recordings of the activity of the masseter muscle showed heavier activity in males than females. In their study, the right and left condyles were similar in shape in the majority of the mandibles. However, the frequency of a convex lateral shape displayed sexual variation.[16]
This study revealed that there was a statistically significant relationship between age groups and dentition status (P < 0.05). As the age advances the dentition status drifted toward Eichner Class C so as the association between dentition status and condylar, morphology was also significant (P < 0.05) [Figures 1 and 2].
The statistically significant relationship between the dentition status and bilaterally similar shaped condyles (P < 0.05) was observed. A total of 285 persons out of 350 individuals with bilaterally similar shape condyles were found in the study group, of which 227 (79.6%) persons were having the Eichner Class A, with bilateral round-shaped condyles in 146 persons (64.3%). In the Eichner Class B, 28 persons were found of which 17 persons (61%) were sighted with bilaterally round-shaped condyles and among the Eichner Class C, 30 persons of which 13 (43.3%) were observed with bilaterally round-shaped condyle. The frequency of bilaterally round- shaped condyles was most with the dentition status Eichner Class A, was observed to be least in the Eichner Class C. As the dentition status shifted with advancing age, a better distribution of condylar shapes can be noted, and the frequency of round, pointed, and angled condyles becomes much similar [Figures 1-10]. Search of available literature does not show any study which established the relationship between normal condylar morphology to dentition status.
Non-identical combination of round right and flat-shaped left side, angled right and round left side, pointed right side and angled left side condyles on panoramic radiograph, however, seems to be uncommon for all age groups among asymptomatic subjects [Figures 8-10].
There was a statistically significant (P < 0.05) relation between the distribution of condylar morphology on the right and left side to the dentition status [Figures 1 and 2]. The frequency of round-shaped condyles was found more among the individuals with dentition status Eichner Class A, 331 condyles which was more or less equally distributed on both sides (50%). The prevalence of round-shaped condyles was found to be decreased as the dentition status shifted to Eichner B and Eichner C, that is, 38 condyles that were equally seen on both the sides and in Eichner C, 29 condyles (55% on the right side and 45% on the left side) [Figures 1-10]. This shift was also seen in the frequency of bilaterally similar condyles. Halicioglu et al. found slight difference for condylar plus ramal asymmetry index value in patients with early unilateral mandibular first molar extractions.[17]
Mathew et al.[8] did a cross-sectional study of condylar shape and its associations with age TMD, dentition status, among 75 patients. They concluded that radiographic appearance of TMJ varied widely, remodeling changes were commonly seen, and there was no direct linear relationship between age and radiographic changes in condylar morphology.
Since their study showed no significant association between radiographic changes in condylar morphology and clinical signs and symptoms and dentition status, caution should be exercised not to overestimate the significance of radiologic abnormality. Minor changes in the radiographic image of the condyle of the patients with TMD may have no relevance and should not be used to infer a diagnosis. Small sample size and usage of only panoramic radiograph to assess the condylar changes were the limitations. Hence, they emphasized further studies with a larger sample size and other radiographic modalities for studying condylar morphology.[8]
Masanori et al. in their study observed the internal structure of the mandibular condyle in dentulous and edentulous jaws; they performed three-dimensional observation and morphological measurements using micro-CT. They clarified that, in edentulous jaws, reduced masticatory function due to tooth loss affects the internal structures of mandibular condyle.[18]
The relationship between age groups and denture wearing history was found to be statistically significant (P = 0.00). This signifies that with denture usage in the older age groups, there is more likely chance for morphological alteration of mandibular condyle. Uma et al. noted a change in condylar position. They suggested that this may be pathologic and referred it as the edentulous position of the TMJ.[19]
Only 7% of individuals had a history of orthodontic treatment for mild malocclusion in the study subjects of whom 88% of individuals were found to have bilaterally similar shaped condyles and 12% had dissimilar shaped condyles [Figure 2]. No significant association was noted between the history of orthodontic treatment and condylar shapes.
Merigue et al. did a tomographic evaluation of the TMJ in malocclusion subjects, they investigated condylar concentricity and morphology, and their association with Class I and II malocclusions (Angle). The sample consisted of 49 individuals of both genders, between 11 and 35 years old. They found that the convex condyle shape was the most prevalent in their study and Class I and II patients seem to present similar condyle morphology. Regarding the condyle position, anterior displacement was more prevalent regardless of the type of malocclusion. Above researchers also did not find significant association between the groups to the condylar characteristics.[20]
Mohlin et al.[21] did a systematic review of literature to evaluate associations between different malocclusions, orthodontic treatment, and signs and symptoms of TMD. They concluded that the associations between specific types of malocclusions and development of significant signs and symptoms of TMD could not be verified.
When the parafunctional habits with the condylar morphology was assessed we reveled that. The frequency of bilaterally similar round-shaped condyle was observed more in the patients with no parafunctional habits. All persons with parafunctional habits had dissimilar condyles [Figure 2]. This correlation is similar to the study of Tao et al. who noticed significant difference in distribution of condylar morphology type between the group grinding (GG) and GG combined with mediotrusive side grinding (MG).[22]
However, Shetty et al. stated that the self-reported bruxism is probably a poor method of identifying bruxism.[23] Wassell et al.[24] commented that there are also very many people who grind their teeth and who do not develop TMJ symptoms.[24] Bruxism and other parafunctional activities may play a role in perpetuating symptoms in some cases as found by Buescher et al.[25]
Statistically significant relationship (P < 0.05) was seen between chewing habits and bilaterally similar condyle shape. Majority of person had no specified chewing habits with bilaterally round-shaped condyles 120 (68%), followed by bilateral chewing habit 51 persons (29%) and unilateral left side 2 persons (1%) and unilateral right side chewing habit in 3 persons (2%). Round shaped was observed more with the individuals whose chewing habits were not specified and those with bilateral chewing habits [Figure 2]. Similar findings were seen in the study of Halicioglu et al.[17] and Masanori et al.[18] The extensive literature search did not reveal any studies describing the normal morphology of condyle relating chewing habits of the individuals.
Richards studied the morphology of the TMJs in two Australian populations with previously established differences in patterns of tooth wear and craniofacial morphology. They did not found any significant difference from that described in other comparable populations. They sighted that the relationships between age and linear and angular measures of joint form were generally not significant, but the shape of the mandibular condyle was age related, with flattening and cavitation of the posterior and medial aspects being more common in older age groups. Comparison of tooth wear data in groups with different mandibular condylar shapes suggested that rapid anterior tooth wear was associated with flattening or cavitation of the condyle, while relatively rapid posterior tooth wear was more commonly associated with a convex condylar shape.[26]
Further studies are needed with control groups to focus on the incidence of TMJ dysfunction and TMD symptoms, with early loss of dentition (partially or completely edentulism), loss of balance occlusion, and occlusion disharmony other factors such as parafunctional habits and functional chewing habits among the individuals.
CONCLUSION
Although condylar shape and size have been shown to vary between populations, very few studies on condylar morphology have been done. The morphology of the mandibular condyles in the population studied varied considerably on panoramic radiographs. The differences in morphology imply that condylar morphology cannot be generalized while dealing with TMJ pathologies and TMD. Manufacture of condylar prostheses has to be customized for the local population in relation to age, gender dentition status, normal chewing habits, parafunctional habits, history of orthodontic treatment, and history of usage of denture. The dentition status and chewing habits of individuals had a significant role in determining condylar morphology. Further studies are required which should also focus on the occurrence of TMD symptoms with early loss of dentition, chewing habits, and other factors such as parafunctional habits, loss of balance occlusion, and occlusion disharmony. Studies using advanced radiographic modalities will be beneficial.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Contemporary imaging of the temporomandibular joint. Dent Clin North Am. 2008;52:875-90.
- [CrossRef] [PubMed] [Google Scholar]
- Developmental anomalies and dysfunction In: Temporomandibular Joint and Masticatory Muscle Disorders. United States: Mosby; 1994. p. :224-54.
- [Google Scholar]
- Gray's Anatomy: Anatomical Basis of Clinical Practice Edinburgh, New York: Elsevier Churchill Livingstone; 2005.
- [Google Scholar]
- Age-related changes in the human mandibular condyle: A morphologic, radiologic, and histologic study. J Oral Maxillof Surg. 1995;53:1016-23.
- [CrossRef] [Google Scholar]
- Accuracy of cone-beam computed tomography imaging of the temporomandibular joint: Comparisons with panoramic radiology and linear tomography. Am J Orthod Dentofacial Orthop. 2007;132:429-38.
- [CrossRef] [PubMed] [Google Scholar]
- Essentials of Dental Radiography and Radiology Amsterdam: Elsevier Health Sciences; 2013.
- [Google Scholar]
- A 5-year follow-up of occlusal status and radiographic findings in mandibular condyles of the elderly. Int J Prosthod. 2001;15:539-43.
- [Google Scholar]
- Condylar changes and its association with age, TMD, and dentition status: A cross-sectional study. Int J Dent. 2011;2011:413639.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular condyle morphology on panoramic radiographs of asymptomatic temporomandibular joints. Int J Dent. 2009;8:114-8.
- [Google Scholar]
- Reveal the concealed-Morphological variations of coronoid process, condyle and sigmoid notch in personal identification. Egyp J Forensic Sci. 2015;6:108-13.
- [CrossRef] [Google Scholar]
- Shape and symmetry of human condyle and mandibular fossa. Int J Odontostomatol. 2015;9:65-72.
- [CrossRef] [Google Scholar]
- Comparison of occlusal condition and prevalence of bone change in the condyle of patients with and without temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2008;105:104-12.
- [CrossRef] [PubMed] [Google Scholar]
- An epidemiological assessment of mandibular condyle morphology. Oral Surg Oral Med Oral Pathol. 1966;21:169-77.
- [CrossRef] [Google Scholar]
- Gonial angles and condylar and ramus height of the mandible in complete denture wearers--a panoramic radiograph study. J Oral Rehabil. 1997;24:512-6.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of early unilateral mandibular first molar extraction on condylar and ramal vertical asymmetry. Eur J Dent. 2014;8:178.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional analysis of the internal structure of the mandibular condyle in dentulous and edentulous jaws using micro-CT. Cranio. 2014;27:78-87.
- [CrossRef] [PubMed] [Google Scholar]
- Cephalometric evaluation of condyle-fossa position in dentulous and edentulous subjects. Indian J Dent Res. 2015;26:256.
- [CrossRef] [PubMed] [Google Scholar]
- Tomographic evaluation of the temporomandibular joint in malocclusion subjects: Condylar morphology and position. Braz Oral Res. 2016;30:1-3.
- [CrossRef] [PubMed] [Google Scholar]
- TMD in relation to malocclusion and orthodontic treatment. Angle Orthod. 2007;77:542-8.
- [CrossRef] [Google Scholar]
- Mandibular condylar morphology for bruxers with different grinding patterns. Cranio. 2016;34:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Bruxism: A literature review. J Indian Prosthod Soc. 2010;10:141-8.
- [CrossRef] [PubMed] [Google Scholar]
- Temporomandibular joint morphology in two Australian aboriginal populations. J Dent Res. 1987;66:1602-7.
- [CrossRef] [PubMed] [Google Scholar]




