
Translate this page into:
Earlier appearance of Risser sign on ultrasound versus radiograph in adolescent idiopathic scoliosis


*Corresponding author: Michio Hongo, Department of Orthopedic Surgery, Akita University Graduate School of Medicine, Hondo, Akita, Japan. mhongo@doc.med.akita-u.ac.jp
-
Received: ,
Accepted: ,
How to cite this article: Hongo M, Kasukawa Y, Misawa A, Kudo D, Kimura R, Miyakoshi N. Earlier appearance of Risser sign on ultrasound versus radiograph in adolescent idiopathic scoliosis. J Clin Imaging Sci 2022;12:40.
Abstract
Objective
The usefulness of ultrasound in the detailed assessment of the Risser sign is still unclear. The purpose of this study was to analyze the usefulness of ultrasound for determining the Risser sign compared with that determined by conventional radiography by each Risser grade.
Materials and Methods
Eighty-eight iliac crests from 44 adolescent patients who visited the scoliosis clinic with Risser grades 0-4 were evaluated. The ultrasound probe was placed vertically on the iliac crest and the point where iliac apophysis ossification ended was marked. The length of ossification relative to the length of the iliac crest was calculated.
Results
Agreement between radiographic and ultrasound images were found in 58/86 iliac crests (67%). Kappa value was 0.565. Agreement between the two methods with regard to Risser grade was 53% for grade 0, 43% for grade 1, 47% for grade 2, 88% for grade 3, and 90% for grade 4. With additional analysis by integrating grades into two groups, the agreement rate was 47.7% and the Kappa value was 0.288 in the grade 0-2 group, and 88% and 0.703 in grades 3-4 group, respectively. In cases of disagreements, 93% of the iliac crests were judged as having higher Risser grades by ultrasound than by radiograph.
Conclusion
Risser sign evaluation by ultrasound demonstrated a higher agreement rate in grades 3 and 4, whereas less agreement was found in grades 0-2. In the majority of cases with disagreement, ultrasound showed a higher grade than radiography, suggesting that ossification can be detected earlier with ultrasound than with radiography.
Keywords
Risser sign
Ultrasound
Scoliosis
Adolescents
Radiograph

INTRODUCTION
Evaluation of skeletal maturity is important for the estimation of scoliosis progression. The Risser sign was first described in 1936[1] and has been widely used as one of the common radiographic markers to predict growth potential in the same radiograph of a whole spine image.[2] This measurement was reported to correlate poorly with the curve acceleration phase;[3] however, another study stated that a Risser grade of 0 with closed triradiate cartilage and a Risser grade of 1 were identified as predictors of the beginning of the curve acceleration phase.[2]
However, several reports have pointed out the relatively inaccurate reliability of the evaluation of the Risser sign using radiographs.[4-6] In addition, since exposure to multiple diagnostic radiographic examinations may increase the risk of breast cancer among women with scoliosis,[7] radiation exposure should be minimized during childhood and adolescence.
Ultrasound has been proposed as an alternative method to a radiographic evaluation in the determination of Risser grade.[8,9] Although ultrasound requires familiarity with the operation and has an interobserver variety among examiners, the advantages are that it can be easily performed in an outpatient setting and radiation exposure is avoided. However, Torlak et al. reported less consistent agreement with the radiological evaluation of the Risser sign, although interexaminer and intraexaminer reliability of ultrasound was higher compared to radiography.[6] Thus, the usefulness of ultrasound in the detailed assessment of the Risser sign is still unclear. The purpose of this study was to analyze the usefulness of ultrasound for the determination of Risser grade compared with that of conventional radiography and to further evaluate the apophysis appearance by each Risser grade.
MATERIALS AND METHODS
Patients between the ages of 10 and 18 years who visited the scoliosis clinic at our institution were questioned about their medical history and were excluded if they had a metabolic bone disease, growth disturbance, chromosomal abnormality, or previous spine surgery. They underwent anteroposterior radiographs of the whole spine, including the pelvis, in the standing position. Then, followed by a comprehensive explanation of the procedures, risks, and benefits of the study, prospective participants provided their written forms of informed consent approved by the institutional review board.
The Risser grade was determined with plain radiographs from grades 0-5 by the extent of ossification of the apophysis from the anterolateral to posteromedial aspect of the iliac crest.[2] Since Risser 5 was considered to represent mature bone age, 44 patients with Risser grades 0-4 were included in this study, followed by the exclusion of those with grade 5. There were 40 girls with an average age of 12.8 (range, 11-15) years and four boys with an average age of 15.0 (range, 13-17) years. The diagnosis was idiopathic scoliosis in 40 patients and congenital scoliosis in four patients. Average Cobb angle of the main curve was 25 ± 9 degrees.
Ultrasound of the iliac apophysis was performed using an ultrasound apparatus (XARIO, SSA-660A, Toshiba Medical Systems Corporation, Otawara-Shi, Tochigi, Japan) with either a linear or a convex probe. The patients were asked to lie in a lateral decubitus position for both sides, with their iliac crest fully exposed from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS). The length of the iliac crest between the ASIS and PSIS was measured using a measuring tape along the iliac bone. The ultrasound probe was placed vertically on the iliac crest [Figure 1], and the presence or absence of ossification of the apophysis was identified.[9] The probe was moved from the anterolateral to the posteromedial aspect of the iliac crest. The ultrasound images of the iliac crest which were determined as Risser grade 3 by radiograph [Figure 2a] are demonstrated as ossification covering the iliac crest [Figure 2b], ossification nucleus [Figure 2c], and cartilage with low echoic area [Figure 2d]. Then, the point where the ossification nucleus ended was marked. The length of ossification relative to the length of the iliac crest was calculated as the ossification ratio (OR).
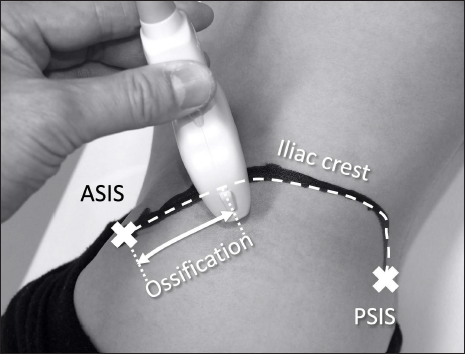
- The length of the iliac crest between the anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS) was measured. The ultrasound probe was placed vertically on the iliac crest. The presence or absence of an ossification of the apophysis was identified. The point where ossification nucleus ended was marked. Then, the length of ossification was measured.

- Plain radiograph of the iliac crest determined as Risser 3. Arrow (1) clearly shows wider ossification, and the ultrasound image at this site corresponds to Figure 2b. Arrow (2) shows thinner ossification, and ultrasound image at this site correspond to Figure 2c. Arrow (3) shows no isolated ossification, and ultrasound image at this site correspond to Figure 2d. Figure 2b: Ultrasound image of ossification covering the iliac crest (1). Figure 2c: Ultrasound image of ossification nucleus (2). Figure 2d: Ultrasound image of cartilage with low echoic area (3).
Risser grade by ultrasound was determined in the same manner as that determined by radiography according to the United States method.[10] No ossification of the apophysis was defined as a Risser grade 0. Risser grades 1 through 4 were determined when the OR of the apophysis involved (≥25%) of the iliac crest as grade 1, (25-50%) as grade 2, (50-75%) as grade 3, and (75-100%) as grade 4.
Ultrasound examination was performed by one of the authors (MH) who has had experience in clinical practice with ultrasound for musculoskeletal disorders for 5 years. One of the authors (AM) who have had more than 10 years of clinical experience in the management of scoliosis determined the Risser grade without any knowledge of the results by ultrasound.
Statistical analysis
The Risser grades evaluated by ultrasound were compared with radiographic evaluation. The agreement of Risser grades between ultrasound and radiography was determined by Kappa statistics. The Kappa values were categorized as follows: 0.81-1.00, excellent; 0.61-0.80, good; 0.41-0.60, moderate; 0.21-0.40, fair; and 0.00-0.20, slight. Statistical analyses were performed using SPSS software, version 26 (SPSS Inc., Chicago, IL).
RESULTS
A total of 88 iliac crests from 44 patients on both sides were available for evaluation in this study. However, radiographs of two iliac crests could not be evaluated due to images that were too poor to determine the Risser grade. Then, 86 iliac crests were analyzed by both radiography and ultrasound.
Agreement between radiograph and ultrasound was found in 58/86 iliac crests (67%). Kappa value was 0.565.
Agreement between the two methods was as follows: 8/15 (53%) for grade 0; 6/14 (43%) for grade 1; 7/15 (47%) for grade 2; 28/32 (88%) for grade 3; and 9/10 (90%) for grade 4 [Table 1]. In the cases of 28 disagreements, 26 (93%) iliac crests were judged as having higher grades than those by radiograph [Table 1].
| Ultrasound | ||||||
|---|---|---|---|---|---|---|
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | ||
| Radiograph | Grade 0 | 8 | 3 | 4 | ||
| Grade 1 | 6 | 6 | 2 | |||
| Grade 2 | 1 | 7 | 7 | |||
| Grade 3 | 28 | 4 | ||||
| Grade 4 | 1 | 9 | ||||
Since the difference in the agreement were notable among the grades, the grades were further integrated into two separated groups: grade 0-2 group and grade 3-4 group, and the agreement rate and Kappa value for each group were calculated. In the grade 0-2 group, an agreement was 47.7% and the Kappa value was 0.288, while the agreement was 88% and the Kappa value was 0.703 in grade 3-4 group.
Case presentation
Two illustrative cases of disagreement in the Risser grade evaluation between radiography and ultrasound are presented. The radiograph of a 12-year-old boy showed no ossification of the iliac crest, and was determined as Risser 0 [Figure 3a]; whereas apophyseal ossification was observed in the area of Risser 1 [Figure 3b], while the ossification was not visible in the area of Risser 2 [Figure 3c], then the patient was determined to be a Risser Grade 1 with ultrasound. Similarly, an 11-year-old girl was determined as Risser 0 radiographically [Figure 4a], however, longitudinal [Figure 4b] and transverse views [Figure 4c] of the ultrasound showed an ossification nucleus in the area of Risser 1.

- A case of disagreement between radiography and ultrasound in a 12-year-old boy. Radiograph of the iliac crest was determined as Risser grade 0. Arrow (4) and (5) shows no ossification. Ultrasound image at the site (4) and (5) correspond to Figure 3b and 3c, respectively. Figure 3b: Ultrasound image showing apophyseal ossification at the site of Risser grade 1 (4). Figure 3c: Ultrasound image shows that apophysis ossification was not appeared at the site of Risser grade 2 (5).

- A case of disagreement between radiography and ultrasound in an 11-year-old girl. Radiograph of the iliac crest with no evident ossification. Figure 4b: Longitudinal view of the iliac crest showing small ossification (arrow C). Figure 4c: Transverse view of the iliac crest where the ossification was observed in longitudinal view at the site C in Figure 4b.
DISCUSSION
Assessment of skeletal maturity of the iliac crest with ultrasound for the evaluation of Risser grade was first described by Wagner et al. in 1995.[9] They evaluated the iliac bone apophysis in children and adolescents with idiopathic scoliosis using ultrasound and radiography and found that the accuracy for the correct determination of the Risser grade by ultrasound in comparison with radiographic evaluation was 89.2%. The authors stated that ultrasound is useful and is an acceptable tool for bone age determination in routine clinical practice and in screening studies for scoliosis. Thaler et al. also reported higher agreement in the early Risser stages and relatively lower agreement in late stages between the two diagnostic methods and described the usefulness of ultrasound as an alternative method to radiography.[8] Contrary to these previous studies, the current study demonstrates that agreement between radiography and ultrasound was lower, especially in the earlier Risser grades. Besides, another study by Torlak et al. similarly reported a lower agreement rate of 77.7% by one examiner and 64.3% by another examiner.[6] One of the causes of the discrepancies in the agreement between X-rays and ultrasound in the literature was considered to be the inconsistencies of the evaluation for the plain X-rays as described below.
There have been several studies describing the inaccuracy of radiographs for the assessment of the Risser signs.[4,5,11,12] Izumi found a discrepancy in the appearance of the iliac apophysis between the posteroanterior and anteroposterior views.[4] The medial and lateral aspects of the apophysis were superimposed over the ilium when the image was produced with the posteroanterior view. Kotwicki described that one-third of the apophysis was not observed on the frontal radiograph.[5] Then the iliac apophysis and fusion could be accurately estimated when the lateral radiograph was analyzed. In addition, Risser grade measurements demonstrated good intraobserver but only fair interobserver reliability.[12] The results in the literature suggest that the ossification of the apophysis might not be observed on radiographs, dependent on the conditions and the direction of X-rays, and the examiners.
Meanwhile, ultrasound evaluation for the assessment of Risser grade was found to be accurate and reproducible. Torlak et al. investigated the accuracy of ultrasound for the evaluation of Risser signs in adolescents.[6] They reported that the kappa value of intraexaminer agreement of the ultrasound was 0.971 and interobserver agreement was 0.924. Whereas, they described lower agreement for the accuracy of the X-ray and ultrasound with the kappa value of 0.698 by one examiner and 0.542 by another examiner, which was compatible with our results. Eventually, they concluded that ultrasound evaluation was a reliable method; however, results could be variable and unstable when radiological evaluation is considered the gold standard.
Although Torlak et al. described the advantages and the accuracy of ultrasound, they did not assess and mention the agreement rate in each Risser grade. In the current study, Risser grade evaluated by ultrasound showed a higher agreement rate and Kappa value in grades 3-4, whereas lesser agreement and Kappa value were found in grades 0-2. In cases of disagreement, the majority of earlier Risser grades by ultrasound were higher than those on radiographs. For example, as shown in Figures 3 and 4, the ossification nucleus was clearly identified with ultrasound in seven cases determined as Risser 0 by radiographs. This disagreement indicates that invisible apophyseal ossification on the radiographs was identified by ultrasound evaluation, suggesting that the ossification can appear earlier on ultrasound than on radiographs.
Multiple indicators for curve progression have been identified, including chronological age, peak height velocity timing,[13,14] secondary sexual characteristics, metabolic markers,[15,16] and skeletal maturities, such as the Tanner-Whitehouse-III method,[17] the Greulich and Pyle method,[18] the Oxford method,[19] and the Risser sign. The Tanner-Whitehouse-III RUS score on a radiograph of the hand and wrist was strongly correlated with the curve acceleration phase, although the method for evaluation is relatively complex and time-consuming. Skeletal age assessment from the olecranon of the lateral radiograph of the elbow has also been shown to be a precise and reliable method allowing for evaluation during the period of peak height velocity.[20] Meanwhile, the Risser sign was poorly correlated with the curve acceleration phase. The iliac apophyses showed ossification at an average of 18 months after the curve acceleration phase.[3] Another study reported that 85% of the patients were at or past their growth peak by the time that the iliac apophysis became visible.[13] The Risser sign does not seem to be useful as a primary method of maturity determination. However, Nault proposed a modified grading system, and a Risser score of 0 with closed triradiate cartilage and a Risser score of 1 were the best predictors of the beginning of the curve acceleration phase.[2] The Risser sign is the finding that is readily available on the spinal radiographs, and therefore it is still important for the assessment of skeletal maturity and correlation with the curve acceleration phase, especially in the earlier grading of the Risser sign. Thus, the ultrasound measurement may be potentially beneficial for calculating skeletal maturity earlier.
There are several limitations to this study. First, this study is a cross-sectional study with small sample size. Secondly, this study focused only on the relationship between ultrasound and radiography. A longitudinal study to evaluate the beginning of apophyseal ossification is needed. Besides, since Risser grade by ultrasound evaluation may show different associations with clinical growth acceleration based on the current results, a further study analyzing the correlation of the timing of the appearance of ossification or other factors related to skeletal maturity with Risser grade by ultrasound may provide valuable information for estimating the curve acceleration phase.
In conclusion, the Risser sign evaluated by ultrasound showed less agreement in grades 0-2 compared with grades 3 and 4. In cases of disagreement, the majority of Risser grades by ultrasound showed a higher grade than by radiography. The results suggested that ossification could be detected earlier with ultrasound than with radiography.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of interest.
References
- A modified Risser grading system predicts the curve acceleration phase of female adolescent idiopathic scoliosis. J Bone Joint Surg Am. 2010;92:1073-81.
- [CrossRef] [PubMed] [Google Scholar]
- Maturity assessment and curve progression in girls with idiopathic scoliosis. J Bone Joint Surg Am. 2007;89:64-73.
- [CrossRef] [PubMed] [Google Scholar]
- The accuracy of Risser staging. Spine (Phila Pa 1976). 1995;20:1868-71.
- [CrossRef] [PubMed] [Google Scholar]
- Improved accuracy in Risser sign grading with lateral spinal radiography. Eur Spine J. 2008;17:1676-85.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrasonographic evaluation of the Risser sign. Is it a reliable and reproducible method? Spine (Phila Pa 1976). 2012;37:316-20.
- [CrossRef] [PubMed] [Google Scholar]
- Breast cancer mortality after diagnostic radiography: Findings from the U.S. Scoliosis Cohort Study. Spine (Phila Pa 1976). 2000;25:2052-63.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic versus ultrasound evaluation of the Risser Grade in adolescent idiopathic scoliosis: A prospective study of 46 patients. Eur Spine J. 2008;17:1251-5.
- [CrossRef] [PubMed] [Google Scholar]
- Determination of skeletal maturity by ultrasound: A preliminary report. Skeletal Radiol. 1995;24:417-20.
- [CrossRef] [PubMed] [Google Scholar]
- Differences in the Risser grading systems in the United States and France. Clin Orthop Relat Res 2005:190-5.
- [CrossRef] [PubMed] [Google Scholar]
- Reevaluation of the use of the Risser sign in idiopathic scoliosis. Spine (Phila Pa 1976). 1992;17:359-61.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability analysis for manual adolescent idiopathic scoliosis measurements. Spine (Phila Pa 1976). 2005;30:444-54.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am. 2000;82:685-93.
- [CrossRef] [PubMed] [Google Scholar]
- Observations on the growth of the female adolescent spine and its relation to scoliosis. Clin Orthop. 1957;10:40-7.
- [PubMed] [Google Scholar]
- Biochemical markers of bone turnover in girls during puberty. Clin Endocrinol (Oxf). 1994;40:663-70.
- [CrossRef] [PubMed] [Google Scholar]
- Insulin-like growth factor I correlations to changes of the hormonal status in puberty and age. Exp Clin Endocrinol. 1994;102:289-98.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of skeletal maturity and prediction of adult height (TW3 method) (3rd ed). London: WB Saunders; 2001.
- [Google Scholar]
- Radiographic atlas of skeletal development of the hand and wrist (2nd ed). Stanford, CA: Stanford University Press; 1959.
- [Google Scholar]
- The Oxford method of assessing skeletal maturity. Clin Orthop. 1957;10:19-39.
- [PubMed] [Google Scholar]
- Skeletal age assessment from the olecranon for idiopathic scoliosis at Risser grade 0. J Bone Joint Surg Am. 2007;89:2737-44.
- [CrossRef] [PubMed] [Google Scholar]




