
Translate this page into:
Cancerogenesis Risks between 64 and 320 Row Detector CT for Coronary CTA Screening
Address for correspondence: Dr. Mohammad K. Khan, Department of Radiation Oncology, Winship Cancer Institute, Atlanta, GA 30322, USA. E-mail: m.k.khan@emory.edu
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives:
This study compares cancerogenesis risks posed by the 64 row detector and the 320 row detector computed tomography scanners used during coronary computed tomography angiography (CCTA) following decennial screening guidelines.
Material and Methods:
Data of the radiation absorbed after CCTA by lung, thyroid, and female breast in patients between 50 and 70 years of age obtained from prior published literature for the 64 row CT scanner were compared with data from our study using 320 row detector CT scanner. Data from the 64 row and the 320 row detector CT scanners was used to determine lifetime attributable risks (LAR) of cancer based on the biological effects of ionizing radiation (BEIR) VII report.
Results:
The relative reduction of LAR (%) for 50-, 60-, and 70-year-old patients undergoing scanning with the 320 row detector CT scanner was 30% lower for lung, and more than 50% lower for female breast when compared with results from 64 row detector CT scanner. The use of 320 row detector CT would result in a combined cumulative cancer incidence of less than 1/500 for breast in women and less than 1/1000 for lung in men; By comparison, this is much lower than other more common risk factors: 16-fold for lung cancer in persistent smokers, 2-fold for breast cancer with a first degree family member history of breast cancer, and 10-fold for thyroid cancer with a family member with thyroid cancer. Decennial screening would benefit at least 355,000 patients from sudden cardiac death each year, 94% of whom have significant coronary artery disease, with at least one stenosis >75%. LAR for thyroid cancer was negligible for both scanners.
Conclusion:
Lung and female breast LAR reductions with 320 row detector compared with 64 row detector CT are substantial, and the benefits would outweigh increased cancer risks with decennial screening in the age group of 50-70 years.
Keywords
Cancerogenesis
coronary computed tomography angiography
coronary artery disease
risk assessment
screening

INTRODUCTION

The assessment of a new medical procedure requires comprehensive evaluation of all conceivable benefits and risks. In the context of coronary computed tomography angiography (CCTA), measurements of the absorbed radiation dose using 64 row detector CT have been assessed and results previously published.[1234] Despite publication of these earlier studies, radiation risk assessment including secondary cancer risks for CCTA screening guidelines is lacking.[5] Deterministic radiation risk assessment is accomplished by comparing radiation dose measurements associated with CCTA with known threshold numbers, whereas stochastic risk assessment requires more sophisticated calculations that are generally derived from past epidemiological low dose radiation exposures published in the biological effects of ionizing radiation (BEIR) VII report.[6] Stochastic risk assessments are therefore scarcer and are usually based on data of individual studies, which do not properly account for all available variables in equipment and techniques used in performing CCTA examinations.
We measured and recorded absorbed radiation dose in radiosensitive organs using standard CCTA protocols for 320 row detector CT. We employed MOSFET detectors to measure the radiation dose by placing these on and within an anthropomorphic phantom. The measured absorbed dose was then used to estimate cancerogenesis risks for several radiosensitive organs using stochastic risk assessment models published in the BEIR VII report. Those cancer risks were then compared with the natural cancerogenesis risk associated with more common risk factors. Finally, a scenario of US wide decennial coronary artery screening was assumed for the age group 50-70 years and cancerogenesis risk to radiosensitive organs was estimated based on the cumulative absorbed radiation dose associated with such screening. The estimated cumulative risk was then compared with the potential benefits of detecting clinically occult coronary artery disease within this hypothetically screened population to determine if risks of decennial screening would outweigh the benefits.
MATERIALS AND METHODS
Absorbed radiation doses associated with CCTA
We have already published a manuscript on radiation dose estimates and this data was used to estimate cancerogenesis risk assessments W1].[2] Previous measurements had been performed with semiconductor field effect transistor detectors calibrated to match the primary beam quality of the CT scanner. Since the CT scanner had beam qualities in the range of 6.5-7.5 mmAl half value layer (HVL) at 120 kVp, the detectors were calibrated against a conventional radiographic unit at 118 kVp with beam quality of 7.15 mmAl HVL. This was done by adding 5.5 mm of aluminum to the faceplate of the collimator. The MOSFET detectors were then subjected to radiation doses of 1, 3, 10, and 30 mGy. Individual calibration factors were obtained for all detectors by fitting these four data points with the least-squares fit using XLGENLINE Software (Version 1.0), “Software for Generalized Least-Squares Fitting”. The conversion factors were then stored in the MOSFET software (mobile MOSFET® software version 2.0, Revision 7.0, Thomson-Nielsen) for immediate readout after each protocol had been performed. Direct calibration data entry using MOSFET's built-in calibration capability was employed to accommodate multiple tube potential calibrations, the least-square fit method was selected to verify that a given set of calibration factors obtained at 118 kVp with beam quality of 7.15 mmAl HVL may be used for different tube potentials with reasonable accuracy (within 5%).
Calibrated MOSFET detectors were then used to measure absorbed radiation dose for thyroid, mid-breast, breast, and mid-lung in an anthropomorphic phantom at 100, 120, and 135 kVp at two different heart rate (HR) settings of 60 and 75 beats per minute (bpm) with a scan field of view (S-FOV) of 320 mm, using 400 mA, 320 × 0.5 mm detectors/160 mm collimator width (160 mm range).(2)
Cancerogenesis risk estimation
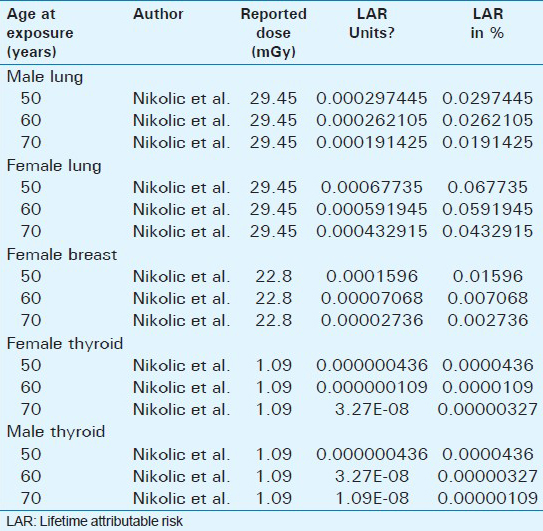
The lifetime attributable risk (LAR) based on absorbed radiation dose measurements of radiosensitive organs (lung, breast, and thyroid exposed to radiation) was adopted from BEIR VII report tabulation (Table 1 2D-1, page 311). To provide the most conservative cancerogenesis risk assessment as possible, absorbed radiation doses for calcium scoring and contrast enhanced CCTA were added for each study and included in our analysis. Data acquired with 120 kVp tube voltage were selected as being both the average and most frequently used maximum tube voltage used in clinical practice.

Lifetime attributable risk estimation
The LAR has been described in the BEIR VII report and is expressed by the formula: LAR (D, e) = ∑ M (D, e, a) S (a)/S (e) with D being the absorbed dose (in the BEIR VII report set as 0.1 Gy), ‘e’ is the exposed age of the patient, ‘a’ being the attained age, which is from e + L to 100 (L being the risk-free latent period that equals 5) accounting for remaining lifetime, S (a) being the probability of survival until age ‘a’, and S (e) being the probability of survival until age ‘e’.
The lifetime attributable cancer risk (LAR) based on absorbed radiation dose for a given organ for each age group of presumed decennial screening was calculated based on linear interpolation of a single time 0.1 Gy radiation exposure data as presented in the BEIR VII report. For instance, the average dose for coronary CTA to the lungs performed with a 320 detector row scanner was 29.45 mGy at 120 kVp and a HR of 60 bpm. From the BEIR VII report, the lung cancer incidence for 50-year-old women is 230 cases per 100,000. Thus, the LAR from a 29.45 mGy dose is (29.45/100) × (230/100,000), or 0.07%. This risk estimation methodology has been described and reported as acceptable in prior literature.[4]
Additive lifetime attributable risk estimation for decennial generalized screening from age 50 to 70 years
For a hypothetical US nationwide generalized CCTA screening for coronary artery disease, the following assumptions were made: Screening would be performed decennially for each individual for the ages 50, 60, and 70 years. Consequently, LARs for female and male lung, female and male thyroid, and female breast were added for CCTAs for the age 50 (LAR50), 60 (LAR60), and 70 (LAR70) to obtain the cumulative LAR for female and male lung, female and male thyroid, and female breast cancer, respectively, for such screening guidelines. For ages between 50-60 years and 60-70 years, linear interpolation of the BEIR VII data was used. Our approach is similar to the one used by Einstein et al., and can be utilized to determine different cumulative LARs.(4) The population size that would be subjected to such screening was assumed to be 18.8 million people and the annual incidence of occurrence of sudden cardiac death was assumed to be 355.000, 94% of whom have at least one stenosis >75%.[7]
RESULTS
We used the data from our previously published manuscript to calculate cancer risks from radiation.[2]
LAR calculations for radiosensitive organs for ages 50, 60, and 70 years in males and females are tabulated in [Table 2] and Figure 1a and b. Thyroid LAR is negligible for all ages and both genders regardless of which scanner is used. Among radiosensitive organs, all evaluated ages and both genders, LAR is otherwise lowest for female breast at age 70 (0.002%) and highest for female lung at age 50 (0.068%).
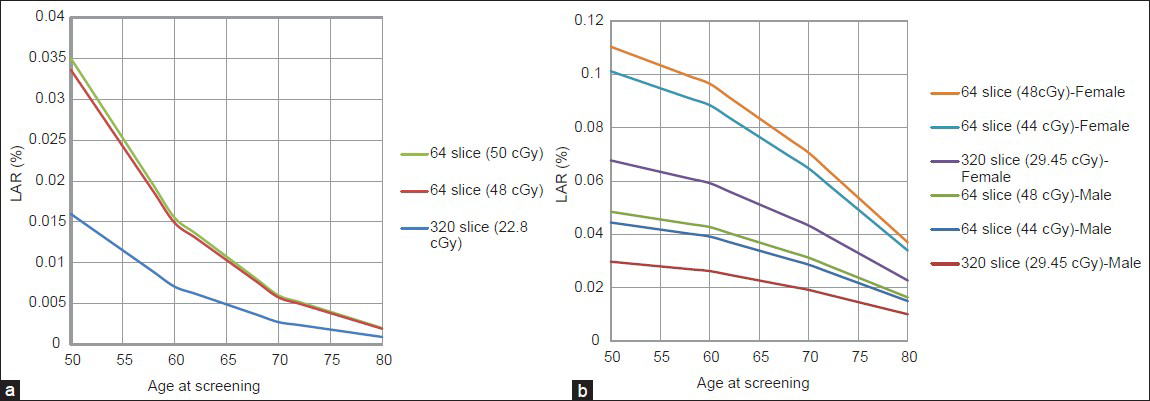
- (a) Reduction in lifetime attributable risk (LAR) for breast cancer with 320 row CT vs. 64 row CT. (b) Reduction in lifetime attributable risk (LAR) for lung cancer with 320 row CT vs. 64 Slice CT.
Cumulative cancerogenesis risk calculation and cancer-specific mortality based on the BEIR VII report for men and women assuming decennial screening between ages 50 and 70 are shown in [Table 3]. These risks are likewise negligible for the thyroid gland for both genders. Cumulative cancerogenesis risk for the recommended CCTA screening assumption using the 320 row detector CT is 0.17% for the female lung and 0.026% for the female breast. Similarly, the cumulative cancerogenesis risk for CCTA screening assumption is 0.079% for male lung using the 320 row detector CT. By comparison, common risk factors, which increase cancer risks, are as follows: 16-fold for lung cancer in persistent smokers,[8] 2-fold for breast cancer with a first degree family member with history of breast cancer,(9) and 10-fold for thyroid cancer with family member with history of thyroid cancer.[10] By way of comparison, CCTA screening in a population assumed to be 18.8 million in size would prevent occurrence of sudden cardiac death in at least some of estimated 355,000 patients, 94% of which have at least one stenosis >75%.

DISCUSSION
In our study, we estimated cancerogenesis risks for a specific organ when using 320 row detector CT by measuring the amount of radiation absorbed by the organ using known methodologies. This is an improvement to earlier organ cancerogenesis estimates that solely relied on respective “in house” absorbed radiation dose measurements in association with CCTA and are therefore more anecdotal in nature. In several previously published studies, radiation absorbed dose was calculated based on the volume CT dose index (CTDIvol) and dose length product (DLP) as proposed by the European Working Group for Guidelines on Quality Criteria for Computed Tomography.[111213141516171819] It should be noted that the CTDI is not meant to be used for dose calculations of individual patients, but rather as a quality assurance and an improvement tool that allows for dose comparisons for different types of CT scanners when the same protocol is applied, or for the same scanner if different protocols are evaluated. As such, it has no role in the calculation of absolute absorbed dose related to deterministic and stochastic risk assessment models.
In this study, we focused on absorbed radiation measurements of radiosensitive organs that are either directly within the CT radiation beam (lung, breast, and skin tissue) or exposed to nearby scattered radiation (thyroid gland). Only one study that had been previously performed with a 320 row detector CT could be included in this analysis. Yet, the stark differences of cancerogenesis risk reduction of >30% for the lung and >50% for the female breast for the 320 row detector CT compared with 64 row detector CT suggest that an epidemiologically meaningful impact is likely due to the padding effects and internal filtration improvements associated with the 320 row detector CT. These improvements can reduce the stochastic risk with future coronary artery screening, and may cause a paradigm shift when weighing risks and benefits of such a screening program. Specifically, the cancerogenesis estimates data that were calculated based on the 320 row detector CCTA would result in a combined cumulative cancer incidence of less than 1 in 500 for breast and lung cancer in women and a cumulative cancer incidence of less than 1 in 1000 for lung in men. As such, these cancerogenesis risk estimates are in magnitudes lower than common risk factors such as persistent smoking for the development of lung cancer (16-fold) or history of breast cancer in a first degree relative for the development of breast cancer (2-fold).[89] It should be noted, that cancerogenesis incidence estimates do not equate to cancer-induced mortality data. Our data may underestimate the role of other causes of death and also do not account for the capability of CCTA to detect other clinically relevant findings such as clinically occult pulmonary embolism, malignant pulmonary nodules, or other undetected cardiopulmonary abnormalities, which may also translate into improved patient outcome. In terms of expected benefits of a screening program as the one suggested, the population size that would be submitted to such screening was previously assumed to be 18.8 million people and the annual incidence of occurrences of sudden cardiac death as 355,000, 94% of which have at least one stenosis >75%.(7) As such, we believe that CCTA screening along the lines suggested with use of 320 row detector scanning and associated improvements in padding and filtration techniques can be justifiably advocated. This is contradictory to prior statements that have identified absorbed radiation associated with CCTA as a primary concern to reject CCTA as a screening tool for coronary artery disease.[5] Recent availability of the iterative reconstruction technique could reduce the radiation dose while maintaining the image quality of CCTA.[2223]
Unlike for lung and female breast, higher absorbed thyroid doses and resulting stochastic risks were found to the same for the 320 row detector CT when compared with a 64 row detector CT. This discordance can be explained by differences in measurement technique. Specifically, measurements with the 320 row detector CT were performed with the MOSFET detectors on top of the phantom surface, whereas Hurwitz et al., obtained measurements within the phantom and more closely simulated the anatomic position of the thyroid gland, thus resulting in less scatter and more dose absorption of interposed tissue and hence lower absorbed dose readings of the detectors.[20] However, thyroid dose absorptions are negligibly low in both studies, and the dose that is absorbed by the thyroid gland in association with CCTA can be safely considered as clinically inconsequential as the likelihood of cancer induction is close to zero based on BEIR VII data for patients between the ages of 50-70 years.
Limitations
The studies that were selected for comparative purposes used either an anthropomorphic phantom or an anthropomorphic mathematical phantom to measure the absorbed dose. Thus, this provided a certain degree of methodological measurement consistency for a greater transparency in inter-study comparisons of the combined equipment and CCTA protocol effects. Yet, the body mass index of the average patient as well as a potential screening subject may be greater than that of the phantom, which may result in underestimation of the scatter radiation dose associated with CCTA. At the same time it should be noted that there are natural limitations to performing direct organ measurements in vivo and that internal organ point measurements in cadavers (the main conceivable alternative to a phantom) also has inherent inaccuracies due to tissue density differences between an actual patient and a bloodless cadaver fixated in formalin.
In addition, the use of LAR to estimate cancerogenesis risk was based on the BEIR VII data, which has its own inherent limitations. A “subjective 95% confidence interval” is assigned to the LAR in the BEIR VII report in acknowledgment of the uncertainties associated with data extrapolated from the Japanese survivors to the U.S. population.
CONCLUSION
During CCTA, among radiosensitive organs at risk, LAR is highest for the lung but this risk remains relatively small compared with other more common cancerogenic risk factors such as smoking. Compared with the 64 row detector CT, technical improvements associated with the 320 row detector CT reduce radiation dose absorbed by the organs in the field of view (lung and female breast).
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2014/4/1/18/131640
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Pediatric cardiac-gated CT angiography: Assessment of radiation dose. AJR Am J Roentgenol. 2007;189:12-8.
- [Google Scholar]
- Absorbed radiation dose in radiosensitive organs during coronary CT angiography using 320-MDCT: Effect of maximum tube voltage and heart rate variations. AJR Am J Roentgenol. 2010;195:1347-54.
- [Google Scholar]
- Radiation dose from contemporary cardiothoracic multidetector CT protocols with an anthropomorphic female phantom: Implications for cancer induction. Radiology. 2007;245:742-50.
- [Google Scholar]
- Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007;298:317-23.
- [Google Scholar]
- Ionizing Radiation in Cardiac Imaging. A Science Advisory From the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009;119:1056-65.
- [Google Scholar]
- BEIR VII (Committee to Assess the Health Risks from Exposure to Low Levels of Ionizing Radiation) Health Risks from Exposure to Low Levels of Ionizing Radiation. Washington, DC: National Academy Press; 2006.
- [Google Scholar]
- Radiation exposure of computed tomography and direct intracoronary angiography: Risk has its reward. J Am Coll Cardiol. 2006;47:1846-9.
- [Google Scholar]
- Smoking, smoking cessation, and lung cancer in the UK since 1950: Combination of national statistics with two case-control studies. BMJ. 2000;321:323-9.
- [Google Scholar]
- Rapid CT diagnosis of acute appendicitis with IV contrast material. Emerg Radiol. 2006;12:99-102.
- [Google Scholar]
- Increased risk for nonmedullary thyroid cancer in the first degree relatives of prevalent cases of nonmedullary thyroid cancer: A hospital-based study. J Clin Endocrinol Metab. 2001;86:5307-12.
- [Google Scholar]
- Radiation exposure and image quality in staged low-dose protocols for coronary dual-source CT angiography: A randomized comparison. Eur Radiol. 2010;20:1197-206.
- [Google Scholar]
- Radiation dose exposure of computed tomography coronary angiography: Comparison of dual-source, 16-slice and 64-slice CT. Heart. 2009;95:1337-42.
- [Google Scholar]
- Radiation dose in a “triple rule-out” coronary CT angiography protocol of emergency department patients using 64-MDCT: The impact of ECG-based tube current modulation on age, sex, and body mass index. AJR Am J Roentgenol. 2009;192:866-72.
- [Google Scholar]
- Evaluation of a body mass index-adapted protocol for low-dose 64-MDCT coronary angiography with prospective ECG triggering. AJR Am J Roentgenol. 2009;192:635-8.
- [Google Scholar]
- Image quality and radiation dose in 256-slice cardiac computed tomography: Comparison of prospective versus retrospective image acquisition protocols. Eur J Radiol. 2011;80:127-35.
- [Google Scholar]
- Comparison of sequential and helical scanning for radiation dose and image quality: Results of the Prospective Multicenter Study on Radiation Dose Estimates of Cardiac CT Angiography (PROTECTION) I Study. AJR Am J Roentgenol. 2010;194:1495-9.
- [Google Scholar]
- Adequate image quality with reduced radiation dose in prospectively triggered coronary CTA compared with retrospective techniques. Eur Radiol. 2009;19:2147-55.
- [Google Scholar]
- Radiation dose estimates from cardiac multislice computed tomography in daily practice: Impact of different scanning protocols on effective dose estimates. Circulation. 2006;113:1305-10.
- [Google Scholar]
- Radiation dose, image quality, stenosis measurement, and CT densitometry using ECG-triggered coronary 64-MDCT angiography: A phantom study. AJR Am J Roentgenol. 2008;190:315-20.
- [Google Scholar]
- AdaptiveIterative Dose Reduction in coronary CT angiography using 320-row CT: Assessment of radiation dose reduction and image quality. J Cardiovasc Comput Tomogr. 2012;6:318-24.
- [Google Scholar]
- Comparison of radiation dose and image quality: 320-MDCT versus 64-MDCT coronary angiography. AJR Am J Roentgenol. 2011;197:163-8.
- [Google Scholar]
- Radiation exposure for coronary artery calcium score at prospective 320 row multi-detector computed tomography. Int J Cancer Ther Oncol. 2013;1:01023.
- [Google Scholar]
- Effect of Tube Voltage (100 vs. 120 kVp) on Radiation Dose and Image Quality using Prospective Gating 320 Row Multi-detector Computed Tomography Angiography. J Clin Imaging Sci. 2013;3:62.
- [Google Scholar]




