
Translate this page into:
Bisystolic Vertebral Artery: Critical Finding or can be Ignored?
Address for correspondence: Dr. Pranav Sharma, Yale New Haven Health at Bridgeport Hospital, Bridgeport, Connecticut, USA. E-mail: drpranavsharma29@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The carotid Doppler imaging findings in three adults presenting with vertigo, transient speech difficulty and for cardiac prebypass graft surgery revealing two systolic peaks in one of the vertebral arteries. In presteal situations, vertebral artery waveform shows two systolic peaks with sharp first and rounded second systolic peak or two systolic peaks with a deep cleft between the two peaks with antegrade flow. With increase in stenosis to more than 80% there is bidirectional flow and later flow reversal. We discuss the types of presteal vertebral artery waveforms, its clinical implications and brief review of literature.
Keywords
Carotid Doppler
presteal vertebral artery waveform
vertebral bunny waveform


INTRODUCTION
Carotid Doppler is one of the most common examinations performed in radiology. The main purpose of the study is to look for atherosclerotic disease, but sometimes, the study is performed to exclude subclavian steal and to follow patients with presteal and steal. Primarily, Doppler is used to characterize and quantify the stenosis in the vessels, but spectral waveforms can suggest subtle clues of the disease. Presteal waveform depicts two systolic peaks in the vertebral artery. Provocative maneuvers can transform a presteal waveform with two systolic peaks into complete steal waveform with reversal of flow. Due to the real-time and dynamic nature of the Doppler sonography, it gives very reliable and reproducible results.[1] The vertebral artery is visualized by moving the ultrasound probe posteriorly and laterally from the region of carotid artery.[2]
CASE REPORTS
Case 1
A 78-year-old female presented to the emergency department with vertigo, no facial asymmetry or any viral illness and stroke scale was zero. Computed tomography (CT) head and carotid Doppler was ordered as a part of the workup. CT head was unremarkable. Carotid Doppler revealed two systolic peaks in the left vertebral artery suggesting presteal waveform.
Case 2
A 62-year-old female for precardiac bypass graft workup. Carotid Doppler revealed two systolic peaks in the left vertebral artery Doppler suggesting presteal waveform.
Case 3
An 87-year-old female presented to the emergency department with word finding difficulty and transient altered speech. There was no cranial nerve deficits, and stroke scale was zero. Her symptoms resolved spontaneously. Carotid Doppler and CT angiography (CTA) of head and neck and were ordered as a part of the workup. Carotid Doppler revealed flow reversal in the left vertebral artery suggesting subclavian steal. The CTA showed patent carotid and vertebral arteries. Magnetic resonance angiography (MRA) with time-of-flight imaging was performed which revealed the absence of signal in the left vertebral artery suggesting flow reversal likely secondary to subclavian steal.
The findings were discussed with the treating physicians. The patients were further evaluated for the causes of subclavian steal. Informed consent was obtained for the procedures and academics in accordance with the ethical standards of the Institutional and/or National Research Committee.
DISCUSSION
The vertebral artery shows normal antegrade flow pattern with waveform similar to the internal carotid artery. Vertebral artery is low resistance system supplying about 20%–30% blood flow to the brain.[3] There are characteristic flow pattern changes in the vertebral artery secondary to ipsilateral subclavian stenosis proximal to vertebral artery origin. The severity of stenosis can be graded according to the abnormal waveform.[4]
The earliest abnormality in the vertebral spectral waveform is transient sharp deceleration of blood flow after the first systolic peak producing a notch and giving rise to two systolic peaks with first being sharp and the second being rounded. With increasing stenosis the notch deepens, which means the first systolic peak becomes sharp and the second peak broadens. This represents in a shape of a crouching bunny [Figure 1].[5] Eventually, the nadir of the notch reaches the baseline and eventually crosses the baseline causing flow reversal. This reversal is minimal and transient at first and gradually progresses to complete flow reversal which indicated high-grade stenosis.[6]
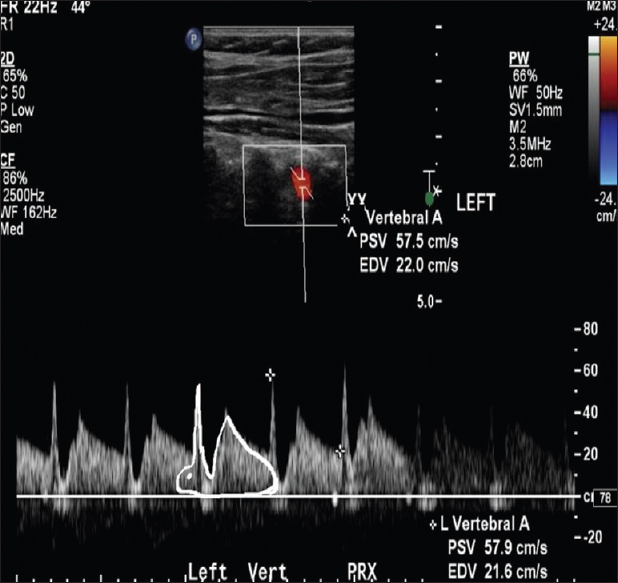
- A 78-year-old female with vertigo. The left vertebral artery Doppler tracing showing two systolic peaks and the flow velocity at the nadir of the notch less than the flow velocity at the end diastole suggesting Type 2 waveform appearing like crouching bunny with ear representing first systolic peak and back hump representing the second peak.
The subclavian steal is due to flow being directed away from stenosed subclavian artery to the upper limb causing flow reversal in the vertebral artery. A similar phenomenon is also described in the coronary arteries. This is explained by Bernoulli's equation which relates the velocity and pressures in a system inversely, i.e., when the velocity increases in an artery, for example, secondary to stenosis the pressure decreases. This decrease in pressure is transmitted to the vertebral artery from which the blood is siphoned in the reverse direction. The pressure drop is greatest when the blood flow velocity is maximum across the stenosis which is at the peak systole. This pressure drop is reflected as the notch in the vertebral spectral waveform.[1]
The subclavian steal waveforms have been classified into four types with various patterns showing two systolic peaks to flow reversal [Table 1 and Figure 2].[7]
| Type | Flow pattern | Degree of stenosis(%) |
|---|---|---|
| Type 1 | Two systolic peaks with flow velocity at the nadir of the notch greater than the flow velocity at the end diastole | 43 |
| Type 2 | Two systolic peaks with flow velocity at the nadir of the notch equal to or less than the flow velocity at the end diastole | 53 |
| Type 3 | Two systolic peaks with flow velocity at the nadir reaches the baseline | 72 |
| Type 4 | Two systolic peaks with flow velocity at the nadir below the baseline | 80 |
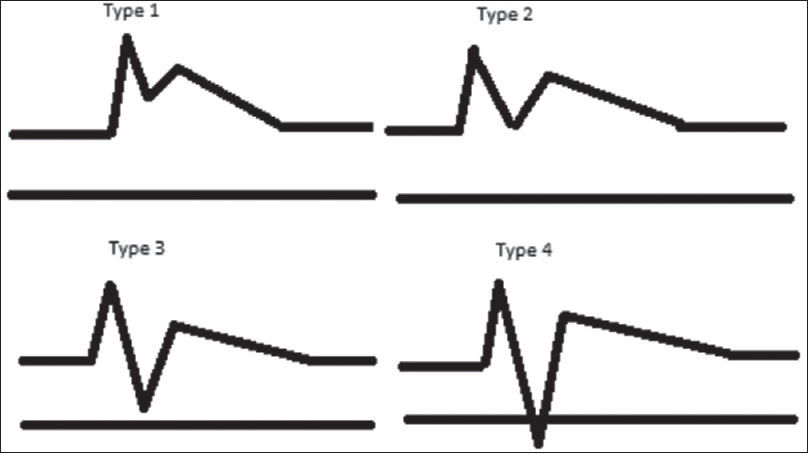
- Schematic representation of the types of presteal waveforms.
Type 1: Two systolic peaks with flow velocity at the nadir of the notch greater than the flow velocity at the end diastole.
Type 2: Two systolic peaks with flow velocity at the nadir of the notch equal to or less than the flow velocity at the end diastole [Figure 3].
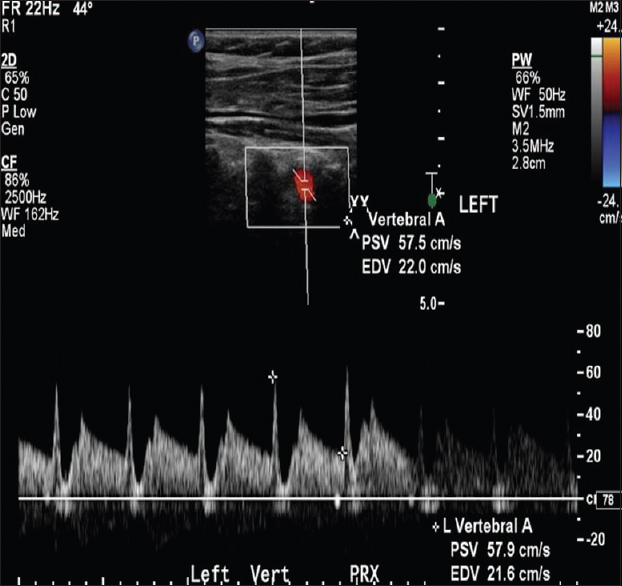
- A 62-year-old female for pre bypass graft workup. Left vertebral artery Doppler tracing showing two systolic peaks and the flow velocity at the nadir of the notch equal to or less than the flow velocity at the end diastole suggesting Type 2 waveform.
Type 3: Two systolic peaks with flow velocity at the nadir reach the baseline.
Type 4: Two systolic peaks with flow velocity at the nadir below the baseline.
Beyond this, there is flow reversal [Figure 4]. Our patients presented with vertigo, transient altered speech and reading and other with prebypass graft surgery. This is a common workup for such patients. The carotid Doppler revealed two systolic peaks in one of the vertebral arteries. CTA revealed patent bilateral vertebral arteries [Figure 5]. One disadvantage with CTA is that it does not show the flow direction. For flow direction, the Doppler examination is helpful. The MRA reveals signal loss on three-dimensional time-of-flight images which picks up signal in vessels with flow in the direction magnetic pulse and loss of signal from vessels with flow in reverse direction [Figure 6].

- An 87-year-old female with transient speech difficulty. Vertebral artery Doppler tracing showing flow reversal in the left vertebral artery.
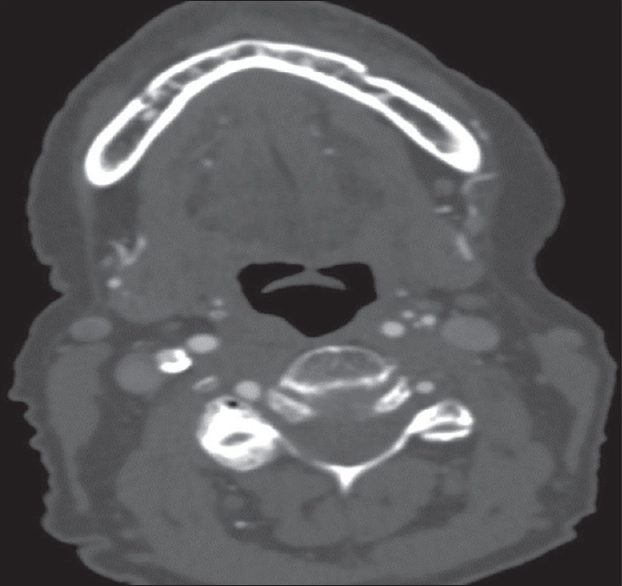
- An 87-year-old female with transient speech difficulty. Computed tomography angiography of neck of the same patient as Figure 3, showing patent bilateral vertebral arteries.

The identification of these presteal waveforms helps in informing the clinicians for further evaluation of posterior circulation flow abnormalities secondary to subclavian artery disease or other causes, before the development of frank retrograde flow. These changes can also be followed up with ultrasound or magnetic resonance imaging for response to the treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2019/9/1/2/251289
REFERENCES
- A spectrum of Doppler waveforms in the carotid and vertebral arteries. AJR Am J Roentgenol. 2003;181:1695-704.
- [Google Scholar]
- Sonography of the vertebral arteries: A window to disease of the proximal great vessels. AJR Am J Roentgenol. 2001;177:53-9.
- [Google Scholar]
- The vertebral bunny waveform: An early manifestation of the subclavian steal syndrome. JBR-BTR. 2012;95:340.
- [Google Scholar]
- Carotid and vertebral artery Doppler ultrasound waveforms: A pictorial review. Ultrasound Q. 2011;27:81-5.
- [Google Scholar]
- Vertebral artery Doppler waveform changes indicating subclavian steal physiology. AJR Am J Roentgenol. 2000;174:815-9.
- [Google Scholar]




