
Translate this page into:
A Rare Case of Laryngopyocele with Airway Obstruction
Address for correspondence: Dr. Sun Yu Lam, Department of Radiology, Ground Floor, Main Block, Tuen Mun Hospital, New Territories, Tuen Mun, Hong Kong. E-mail: pikapat@yahoo.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Laryngocele is a rare entity and can be defined as an abnormal cystic dilatation of saccule of the laryngeal ventricle with communication to the lumen of larynx. Laryngopyocele is a rare complication of laryngocele when it is infected. Patients may present with fever, neck swelling, shortness of breath, and hoarseness. Acute presentation can develop rapidly with alarming symptom, such as stridor, which signifies airway obstruction and warrants immediate treatment and airway protection. Computed tomography and endoscopy are useful in making the diagnosis and delineate the severity of disease. Laryngopyocele should be treated with antibiotics, drainage of purulent content, and followed by definitive surgical excision.
Keywords
Airway obstruction
laryngocele
laryngopyocele


INTRODUCTION
Laryngocele is an abnormal cystic dilatation of saccule of the laryngeal ventricle in connection with the lumen of larynx.[1] It is a rare entity with estimated incidence of 1 in 2,500,000 people per year.[234] Laryngopyocele is a very rare occurrence when the laryngocele is infected, with about 40 cases reported in literature.[1235] It becomes a life-threatening condition when there is mass effect causing airway obstruction, which requires prompt recognition and treatment. There are about four cases previously reported for laryngopyocele with airway compromise.[2] A case of laryngopyocele in a 75-year-old patient with airway obstruction is described.
CASE REPORT
A 75-year-old patient with a history of hypertension and chronic obstructive pulmonary disease presented to accident and emergency department with right neck swelling, sore throat, and low-grade fever for few days. Physical examination revealed tender right submandibular swelling with normal overlying skin. He had a low-grade fever and was in shortness of breath. White cell count was elevated to 18.9.
Imaging findings
A 75-year-old patient with mixed-type laryngopyocele presented with fever, right neck swelling, and shortness of breath. Plain lateral neck radiograph demonstrated air-fluid level (arrow) and swelling (asterisk) over upper cervical parapharyngeal soft tissues [Figure 1a].
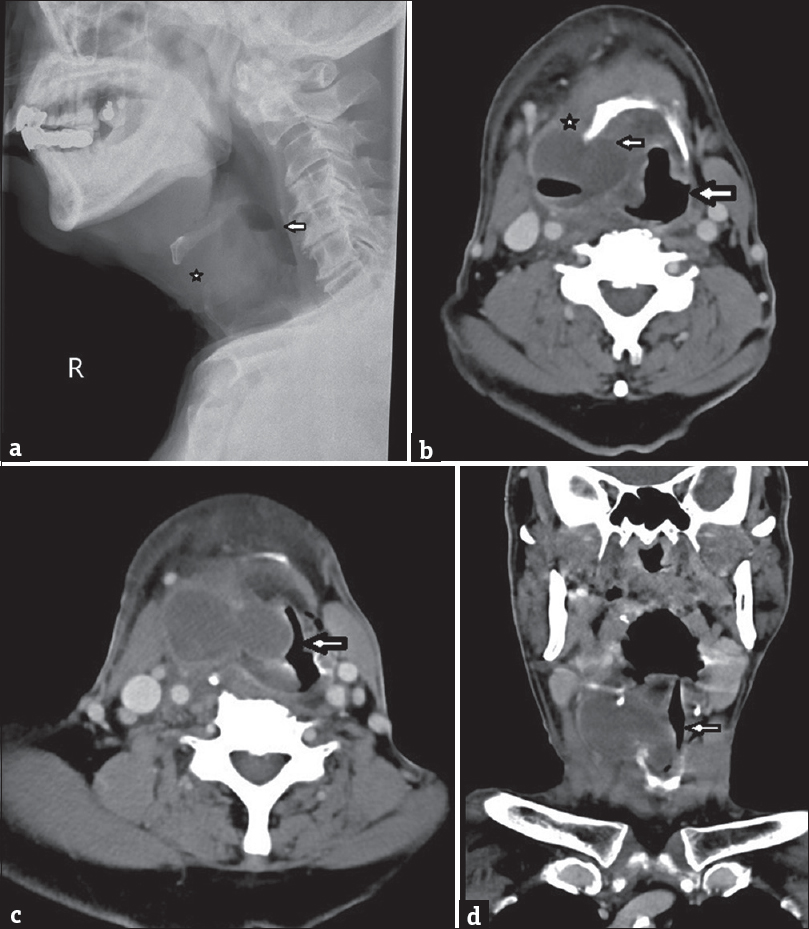
- (a) A 75-year old patient with mixed-type laryngopyocele presented with fever, right neck swelling, and shortness of breath. Plain lateral neck radiograph demonstrated air-fluid level (arrow) and swelling (asterisk) over the upper cervical paralaryngeal soft tissues, (b) Axial contrast-enhanced computed tomography image revealed cystic lesion with internal gas pockets and enhancing wall in the supraglottic region with epicenter at the right thyrohyoid membrane. It spanned medially (small arrow) and laterally (asterisk) to the hyoid bone crossing thyrohyoid membrane. Mass effect was noted with narrowing of the larynx (large arrow). The overall features were suggestive of a mixed-type laryngopyocele complicating airway obstruction (c and d) Axial and coronal contrast-enhanced computed tomography images showed marked narrowing of airway (arrow) by compressive effect of laryngopyocele. With signs of stridor and airway obstruction, subsequent intubation was performed for this patient.
Axial contrast-enhanced computed tomography (CT) image revealed cystic lesion with internal gas pockets and enhancing wall in the supraglottic region with epicenter at the right thyrohyoid membrane. It spanned medially (small arrow) and laterally (asterisk) to the hyoid bone crossing thyrohyoid membrane. Mass effect was noted with narrowing of the larynx (large arrow). Overall features were suggestive of a mixed-type laryngopyocele complicating airway obstruction [Figure 1b].
Axial and coronal contrast-enhanced CT images showed marked narrowing of airway (arrow) by the compressive effect of laryngopyocele. With signs of stridor and airway obstruction, subsequent intubation was performed for this patient [Figure 1c and d].
The patient had increased shortness of breath, and nasal intubation with fiber optics was performed by anesthetist for airway protection. Subsequent laryngoscopy by ear, nose, and throat doctor showed large cystic lesion over the right ventricular region with redundant mucosa and adjacent edematous lingual epiglottis and arytenoids. Biopsy was taken showing acute suppurative inflammation with no evidence of malignancy.
Ultrasound-guided needle aspiration was performed which yielded turbid fluid. Culture grew Haemophilus influenzae. He was treated with antibiotics for clinical improvement. Subsequently, he was extubated and stable for discharge. At follow-up outpatient clinic, the patient was asymptomatic with good general condition. Flexible laryngoscopy showed mild right ventricular bulging. Surgery for excision of laryngocele was offered; however, the patient and relatives opted for conservative management due to old age and high anesthetic risk.
DISCUSSION
Laryngocele is a rare entity with an estimated incidence of 1 in 2,500,000 people per year.[234] It occurs five times more frequently in male, with unilateral involvement more common than bilateral disease.[23] Laryngocele is an abnormal cystic dilatation of saccule of the laryngeal ventricle, it is filled with air, and in connection with the lumen of larynx.[1] The underlying etiology for laryngocele is unclear, with postulation of having both congenital (long saccule) and acquired (increase intraglottic pressure from singing, straining, and glass blowing) components.[36] Since the patient in our case has a history of chronic obstructive pulmonary disease, having chronic cough will increase intraglottic pressure and may play a role in the development of laryngocele. There are three types of laryngocele classified based on its location to the thyrohyoid membrane as follows: internal, external, or mixed type.[5] Internal type is confined within the paraglottic space and medial to the thyrohyoid membrane. External type is seen at the level of hyoid bone, lateral to the opening of thyrohyoid membrane. Majority of the cases are of mixed type, which consists of both internal and external components. Patients usually present with cough, dysphagia, hoarseness, and even dyspnea or stridor depending on the severity of disease. Laryngocele may be complicated with retention of mucus when its neck has been obstructed, being termed laryngomucocele. Laryngoceles are associated with laryngeal carcinoma, with the presence of ~18% of laryngocele in patients with laryngeal carcinoma.[7891011] Laryngopyocele occurs when the laryngocele is infected, usually found in the mixed type, with pathogens most commonly being Escherichia coli, Haemolytic Streptococcus B, Staphylococcus aureus, and Pseudomonas Aeruginosa.
Laryngopyocele is a very rare occurrence with about 40 cases reported in literature and only 4 cases causing acute airway obstruction.[1235] During acute presentations, the initial treatment includes drainage which reduces the mass effect and prevents inhalation of purulent material in case of cystic rupture. Broad-spectrum antibiotics are used to target the culprit bacterial organisms. Subsequent definitive management includes endoscopic resection to prevent recurrence. For the patients with laryngeal carcinoma complicated with laryngocele or laryngopyocele, the management includes excision, laryngectomy, and radiotherapy depending on the tumor staging.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2018/8/1/42/245529
REFERENCES
- Internal laryngopyocele as a cause of acute airway obstruction: An extremely rare case and review of the literature. Acta Otorhinolaryngol Ital. 2012;32:58-62.
- [Google Scholar]
- Laryngopyocele: Three new clinical cases and review of the literature. Eur Arch Otorhinolaryngol. 2000;257:507-11.
- [Google Scholar]
- Laryngocele associated with laryngeal carcinoma. Rom J Morphol Embryol. 2011;52:183-5.
- [Google Scholar]
- Asymptomatic bilateral mixed-type laryngocele and laryngeal carcinoma. Eur Arch Otorhinolaryngol. 2004;261:307-9.
- [Google Scholar]
- Acutely obstructed airway resulting from complications of a laryngopyocoele. Case Rep Surg 2017 2017:8123573.
- [Google Scholar]
- Radiology in focus: Laryngocele and squamous cell carcinoma of the larynx. J Otol Laryngol. 2001;115:590-2.
- [Google Scholar]
- Relationship between laryngoceles and laryngeal carcinomas. Laryngoscope. 1978;88:680-8.
- [Google Scholar]
- Observations on the size of the saccule in laryngectomy specimens. Laryngoscope. 1987;97:190-200.
- [Google Scholar]




