
Translate this page into:
Nasal Lobular Capillary Hemangioma
Address for correspondence: Dr. Saurabh Singla, B 101, M.S Palazzo, 491, Jakkur Main Road, Yelahanka, Hobli, Bengaluru - 560 064, Karnataka, India. E-mail: saurabh_6681@yahoo.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Nasal lobular capillary hemangioma is a rare benign tumor of the paranasal sinuses. This lesion is believed to grow rapidly in size over time. The exact etiopathogenesis is still a dilemma. We discuss a case of nasal lobular capillary hemangioma presenting with a history of epistaxis. Contrast enhanced computed tomography of paranasal sinuses revealed an intensely enhancing soft-tissue mass in the left nasal cavity and left middle and inferior meati with no obvious bony remodeling or destruction. We present imaging and pathologic features of nasal lobular capillary hemangioma and differentiate it from other entities like nasal angiofibroma.
Keywords
Nasal lobular capillary hemangioma
paranasal sinuses
pyogenic granuloma
Kiesselbach plexus

INTRODUCTION

Nasal lobular capillary hemangioma are rare[1] and benign tumors of paranasal sinuses. The exact etiopathogenesis is unknown, but are commonly seen during pregnancy, in patients on oral contraceptive pills or patients with a history of trauma. Most common location is the head and neck region. Nearly 76.9%[2] of cases seen in children occur in this region with the gingiva, lips, and tongue being the most common sites and nasal cavity a rare site of origin. Nasal lobular capillary hemangioma occurs in children 10 months of age to adults in their 7th decade with a mean age of occurrence being around the 4th decade and has no sex predilection.
These lesions show benign capillary proliferation with distinct lobular architecture and the stoma may be fibro-myxoid/oedematous with acute or chronic inflammation. Nasal lobular capillary hemangioma are rapidly growing hypervascular lesions.
A 46-year-old female patient presented with a 2-week history of intermittent episodes of nasal bleeding. Each episode lasted for 15-20 min as the bleeding stopped spontaneously after applying pressure on the nose. On local nasal examination, it was found that a pale smooth surfaced mass with anterior bleeding point was seen filling the left nasal cavity. The mass was mobile and appeared pedunculated with its base attached to the nasal septum. Mass was non-tender on palpation. Mucosa was normal on the right side with hypertrophy of turbinates. No post-nasal bleed was found on examination of the throat.
RADIOLOGIC FEATURES
Plain and contrast enhanced computed tomography (CT) of the paranasal sinuses revealed a lobulated, well-circumscribed, intensely enhancing soft-tissue mass filling the left nasal cavity [Figures 1 and 2]. Epicenter of the lesion was seen to be in the nasal cavity and it was closely attached to the nasal septum with no erosion or remodeling of underlying bones [Figure 3]. A diagnosis of hemangioma or angiofibroma was made. Embolization was performed prior to surgery to prevent bleeding.

- 46-year-old female with intermittent episodes of nasal bleeding diagnosed with lobular capillary hemangioma. Computed tomography of paranasal sinuses, coronal section, shows a lobulated well-circumscribed soft-tissue mass (white arrow) filling the left nasal cavity.
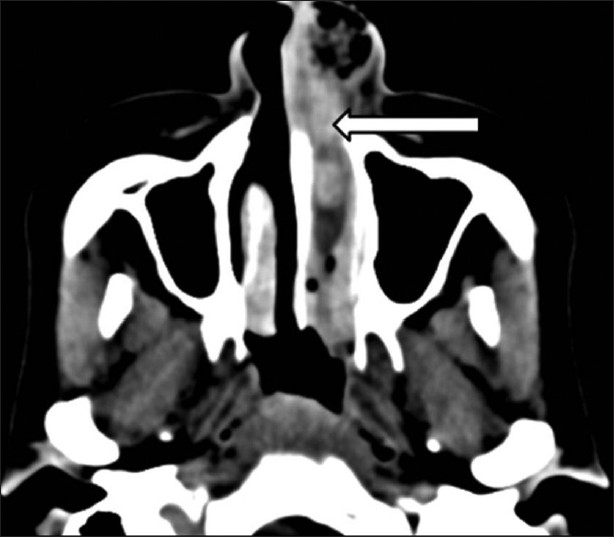
- 46-year-old female with intermittent episodes of nasal bleeding diagnosed with lobular capillary hemangioma. Contrast enhanced computed tomography of paranasal sinuses, axial section shows a lobulated well-circumscribed intensely enhancing soft-tissue mass (white arrow) filling the left nasal cavity.
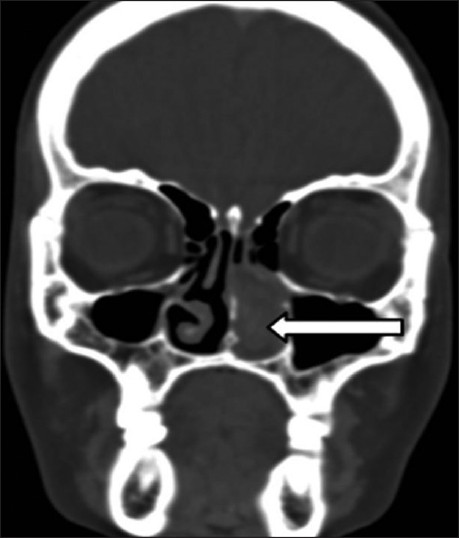
- 46-year-old female with intermittent episodes of nasal bleeding diagnosed with lobular capillary hemangioma. Computed tomography of paranasal sinuses (coronal section) bone window reveals the lesion (white arrow) is closely attached to the nasal septum with no underlying destruction or remodeling of the underlying bones.
PATHOLOGIC FEATURES
An excision biopsy was performed to remove the nasal mass from the septum. The excised specimen consisted of two irregular polypoidal bits of tissue measuring 3 cm × 2 cm × 1 cm mixed with a blood clot, and another bit measuring 2.5 cm × 2 cm × 1 cm [Figure 4]. On the cut surface, gelatinous mucinous-like material was found. Microscopic examination revealed polypoidal bits covered partly by stratified squamous epithelium and partly by pseudo-stratified epithelium with focal ulceration. The underlying stroma shows dense fibrosis and lobules of small capillaries lined by flattened epithelium and filled with blood [Figure 5]. The surrounding inflammatory infiltrate comprised of lymphocytes, eosinophils, plasma cells, and neutrophils these findings led to a diagnosis of lobular capillary hemangioma.
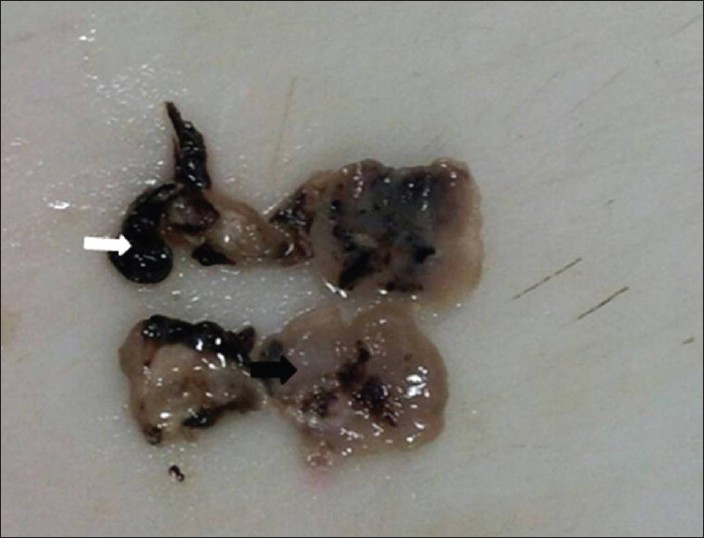
- 46-year-old female with intermittent episodes of nasal bleeding diagnosed with lobular capillary hemangioma. Gross specimen obtained after excisional biopsy of nasal mass from nasal septum shows polypoidal gelatinous tissue bits (black arrow) along with areas of hemorrhage (white arrow).
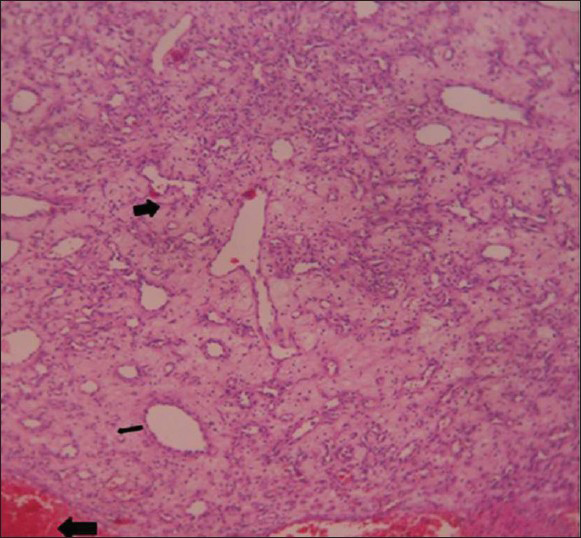
- 46-year-old female with intermittent episodes of nasal bleeding diagnosed with lobular capillary hemangioma. Hematoxylin and eosin stained tissue (×10) reveals lobules of small capillaries lined by flattened endothelium (thin black arrow) filled with blood, the surrounding stroma shows hemorrhage (thick black arrow) at places
DISCUSSION
Lobular capillary hemangiomas was first describe by Poncet and Dor in the year of 1897 where they referred to these tumors as small vascular tumors in the fingers of 4 patients.[3] They called these lesions botryomycosis hominis and thought it to arise secondary to fungal infection. Nasal lobular capillary hemangioma is also called as pyogenic granuloma. Here, the term is a misnomer as it is neither infectious nor granulomatous. First case of pyogenic granuloma of the nasal cavity was described in 1940 by Frank I, and Blahd M. In 1980, Mills et al., termed pyogenic granuloma as lobular capillary hemangioma due to its characteristic microscopic features.[4]
Grossly, these appear as raised or polypoidal mass with surface ulceration, which may or may not be present. On microscopic examination, numerous capillary lobules are seen. This tumor is often misdiagnosed as angiofibroma, which contains marked cellularity when compared with the nasal lobular capillary hemangioma. On immunohistiochemistry, presence of CD 31 positive endothelial cells and actin smooth muscle cells are predominant.
Nasal lobular capillary hemangiomas generally rise from the nasal septum (predominantly from the Little area) and/ or from turbinates on the roof of the nasal cavity or in the maxillary sinus.[5] The Little area, otherwise known as Kiesselbach plexus, is located in anteroinferior part of the nasal septum where four arteries anastomose to form a vascular plexus. The arteries are: (1) anterior ethmiodal artery (2) sphenopalatine artery (3) greater palatine artery and (4) septal branch of superior labial artery.
Lobular capillary hemangiomas are commonly seen in females and usually in the 3rd decade.[16] The exact etiology is still unknown. Recurrent nose picking or nasal packing may play a role in development of lobular capillary hemangioma[67] resulting in overgrowth of granulation tissue.[257] Lobular capillary hemangioma is commonly found in pregnant women and female on oral contraceptive pills and shows a strong association with trauma and hormonal influences on its development.[8]
Imaging of lobular nasal capillary hemangioma is usually by contrast enhanced CT of paranasal sinuses where the scan generally reveals a soft-tissue enhancing mass with or without associated bony destruction. On plain CT nasal lobular capillary hemaingioma appear as well-defined soft-tissue mass, which shows intense enhancement on post contrast study.[9] Lobular nasal capillary hemangioma were not thought to be generally associated with bony erosion though a few studies have found bony erosion to be more common. CT plays an important role in ruling out any destruction of the bony structures,[7] invasion to adjacent paranasal sinuses or intracranial extension. Most common differential diagnosis on CT is nasal angiofibroma. However, nasopharyngeal angiofibroma or juvenile nasopharyngeal angiofibroma should be included in the differential diagnosis only when the patient is an adolescent. The other differential diagnosis to this condition is angiomatous polyp and some uncommon malignant lesions such as nasopharyngeal carcinoma or nasopharyngeal teratoma.
On magnetic resonance imaging, these lesions have intermediate signal on T1-weighted and heterogeneous signal with areas of flow void on T2-weighted sequences showing intense enhancement post gadolinium.
Angiography is useful for preoperative embolization as it reduces the incidence of bleeding during the operation.
Epistaxis and nasal obstruction are the most common presenting symptoms also these lesions are influenced by the depth, location, and patient's age.
Treatment consists of preoperative embolization of these tumors as they are quite hypervascular followed by complete surgical resection of the same as was carried out in our case. Nasal lobular capillary hemangioma associated with pregnancy may regress following childbirth though postpartum lesions that do not regress completely may require surgery patients are generally advised follow-up.
CONCLUSION
With the advent of faster CT scanners and better histopathology techniques nasal lobular capillary hemangioma should be considered as differential diagnosis to nasal angiofibroma as it is mimics this lesion both radiologically as well as pathologically.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/40/119134
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Pediatric lobular capillary hemangioma of the nasal cavity. Eur Arch Otorhinolaryngol. 2004;261:449-51.
- [Google Scholar]
- Lobular capillary hemangioma: The underlying lesion of pyogenic granuloma. A study of 73 cases from the oral and nasal mucous membranes. Am J Surg Pathol. 1980;4:470-9.
- [Google Scholar]
- Lobular capillary hemangioma of the nasal cavity. Otolaryngol Head Neck Surg. 1999;120:783-4.
- [Google Scholar]
- Lobular capillary hemangioma of the nasal cavity: A retrospective study on 40 patients. Am J Rhinol. 2006;20:480-4.
- [Google Scholar]
- A giant pyogenic granuloma in the nasal cavity caused by nasal packing. Eur Arch Otorhinolaryngol. 2002;259:231-3.
- [Google Scholar]
- Lobular capillary haemangioma of the nasal cavity during pregnancy. J Laryngol Otol. 2011;125:973-7.
- [Google Scholar]
- CT findings in two cases of lobular capillary haemangioma of the nasal cavity: Focusing on the enhancement pattern. Dentomaxillofac Radiol. 2012;41:165-8.
- [Google Scholar]




