
Translate this page into:
SYNTAX Score in Patients with High Computed Tomography Coronary Calcium Score
Address for correspondence: Dr. Ravindran Rajendran, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Jayanagar 9th Block, Bannerghatta Road, Bengaluru - 560 069, Karnataka, India. E-mail: ravindran.raje@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives:
To study the conventional coronary angiogram ( CA) findings in patients with high coronary calcium on multidetector computed tomogram.
Materials and Methods:
Fifty patients with coronary calcium high enough in its extent and location to interfere with the interpretation of a contrast-filled coronary artery for a significant lesion were studied with conventional CA. Framingham risk score (FRS), computed tomography (CT) coronary calcium score (CCS), and SYNTAX score (SS) from the CA were calculated by separate investigators who were blinded to other scores. Effectively, 250 coronary arteries (left main, left anterior descending, left circumflex, and right coronary artery and posterior descending artery in each subject) with calcium scores were studied for lesions on CA.
Results:
Thirty-five subjects had high FRS, 10 had intermediate FRS, and 5 had low FRS. Eight subjects of 25 (32%) with CCS between 350 and 1000 had no significant coronary artery disease (CAD). Overall, the CCS and the SS had a strong agreement with each other (r = 0.68, P < 0.01) that persisted in those with very high scores >1000 (r = 0.55, P < 0.01, n = 30), but only a nonsignificant weak correlation with scores between 350 and 1000 (r = 0.1, P = 0.62, n = 20). Individual vessel calcium scores correlated strongly for the presence of any lesion (r = 0.52, P < 0.01) in the same artery but only weakly for a significant lesion (r = 0.29, P = 0.05).
Conclusion:
High CT CCS in this cohort of intermediate to high (Framingham score) risk patients correlated strongly with the subject's global burden of the CAD as derived by the SS, more so for subjects with very high scores. Similarly, CCS correlated strongly with the presence of any lesion but only weakly for a significant stenosis; also, about one-third of patients with CCS between 350 and 1000 may not have significant disease on conventional CA.
Keywords
Calcium score
coronary computed tomography angiogram
Framingham risk score
risk stratification
SYNTAX score


INTRODUCTION
Coronary calcium is a surrogate marker of systemic atherosclerosis. Their identification is an important method of risk stratification in asymptomatic patients with low to intermediate risk for coronary artery disease (CAD). The absence of coronary calcium is associated with a very high event-free probability.[1] Conversely, the detection of coronary calcium indicates an increased risk of incident coronary heart disease above that predicted by standard risk factors, from 2-fold for scores of up to 100–11-fold for scores above 1000.[2] In reality, only 20% of coronary plaques are calcified, and not all calcified plaques contribute to flow-limiting lesions.[3] Hence, contrast computed tomography coronary angiogram (CTCA) is more accurate than coronary calcium score (CCS) in diagnosing or excluding a significant coronary lesion, and it is considered appropriate to perform a CTCA in low and intermediate pretest probability (PTP) patients based on their age, gender, and symptoms. However, a high calcium score precludes CTCA as calcium in the coronaries overestimates lesions due to blooming effect and interferes with a valid interpretation.[4] The purpose of this study was to evaluate the conventional angiogram findings in those patients in whom a CTCA is considered appropriate but could not be performed in view of coronary calcium high enough in its extent and location to preclude a valid interpretation.
MATERIALS AND METHODS
Fifty-two patients who were considered ineligible for undergoing a CTCA (64 row multidetector CT) or had compromised interpretation of CTCA because of high coronary calcium were included in the study. Noncontrast-enhanced prospectively electrocardiogram-gated CT calcium score was performed using a 250 mm field of view and 2.5 mm slice thickness. The calcium scores for individual vessels were computed using the inbuilt software supplemented by manual identification of the calcified locations defined by areas with attenuation >130 HU along the course of the coronary arteries. Noncoronary calcification (sinuses of Valsalva, mitral annulus) was cautiously excluded while measuring calcification. These values were the sum of the area and density of the coronary calcium giving the unitless Agatston score. Radiation dose range was 56.0–65.5 mGy*cm and average was 59.84 mGy*cm. For analysis purpose, a CCS cut off 1000 is used to define those with very calcium score >1000 (very high CCS group) from those with high CCS between 350 and 1000 (high CCS group). Based on individual vessel calcium score, they are divided into the following four groups, namely, none or noncalcified (CCS - 0), low or mildly calcified (CCS - 1–100), moderately calcified (CCS - 101–300), and heavily calcified (CCS ->300). Fifty of the 52 patients underwent conventional CA. The SYNTAX score (SS) known to represent the global atherosclerotic burden was calculated for all patients using the online calculator version 2.11 (http://www.syntaxscore.com) by two separate cardiologists blinded for the calcium score. Concordant scores were accepted, whereas a discordant score was evaluated by a third cardiologist for validation. The lesions in individual coronary arteries are coded on an ordinal scale from normal to total occlusion with insignificant lesions defined as those ranging from any luminal irregularity to <70%, significant lesions with >70% luminal narrowing, and total as those with 100% occlusion. The 2008 Framingham risk score (FRS) was calculated for individual patients from their history, physical examination findings, and blood investigations, and they are divided into a low, intermediate, and high risk based on the cut off 10%, 10%–20%, and >20% 10-year predicted risk for a cardiovascular event, respectively.
Statistical analysis
Demographic characteristics are expressed by descriptive statistics. The coronary stenosis, FRS, and fluoroscopic calcium were studied as ordinal data, whereas the calcium score and the SS are studied as a continuous data. The association between continuous variables is studied using the Pearson's correlation coefficient, whereas the association between ordinal data is studied using nonparametric tests (Spearman's co-efficient). A two-sided P < 0.01 is considered statistically significant. Standard error of mean was calculated for continuous variables between the groups with and without significant stenosis using the independent sample t-test if they are normally distributed; else a nonparametric test like Kruskal–Wallis test was used. A receiver operator curve (ROC) was plotted for the total CCS and individual arterial calcium scores against the presence of a flow limiting stenosis for the corresponding patient or vessel to derive the sensitivity and specificity cut off for CCS in predicting a significant stenosis.
RESULTS
Demography
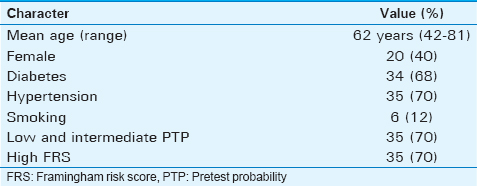
The demographic profile of the patients studied is shown in Table 1. The mean age of the study group was 62 years with 40% represented by females. Hypertensives contributed 70% and 68% of them were diabetics. Seventy percent of the study population had a low to intermediate PTP for CAD based on their age, gender, and symptoms, whereas the rest of the 30% had high PTP but were either self-referred or had denied an invasive angiogram as the initial modality of evaluation. Based on the FRS, 70% had a high risk, 20% had an intermediate risk, and only 10% had a low risk.
Coronary calcium score
All patients except for three had a calcium score >400. In these three patients, the score was between 300 and 400, but were still feared to interfere with contrast CTCA. The mean and standard deviation of the calcium score was 1191 ± 851. Right coronary artery (RCA) had the highest amount of calcium (467 ± 524), followed by left anterior descending (LAD; 458 ± 397), left circumflex (LCX; 181 ± 274), left main (LM; 70 ± 170), and posterior descending artery (PDA) had the lowest calcium.
Coronary calcium score and lesion severity at patient level
Nine patients (18%) of this cohort with high CCS had an angiogram without significant disease in any of the vessels [Table 2 and Figure 1]. Of these, four patients had a CA that was considered to be normal and all four had a CCS <1000. Four of the other five patients with insignificant disease had scores <1000, whereas one had a score >1000. The average calcium for a normal or an abnormal CA with insignificant disease was 611 ± 256, and for an abnormal angiogram with significant disease, it was 1318 ± 885, and this distribution of CCS among patients with and without significant stenosis is statistically significant (P = 0.014) [Figure 2]. The correlation between CCS and significant stenosis is moderate (r = 0.3, P = 0.005) for the whole cohort, but become insignificant when analyzed separately for the high and very high CCS groups. In the ROC analysis, an individual's calcium score of 777 has a sensitivity and specificity of 77% to predict a flow-limiting lesion [Figure 3].
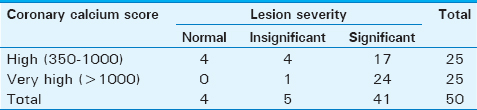
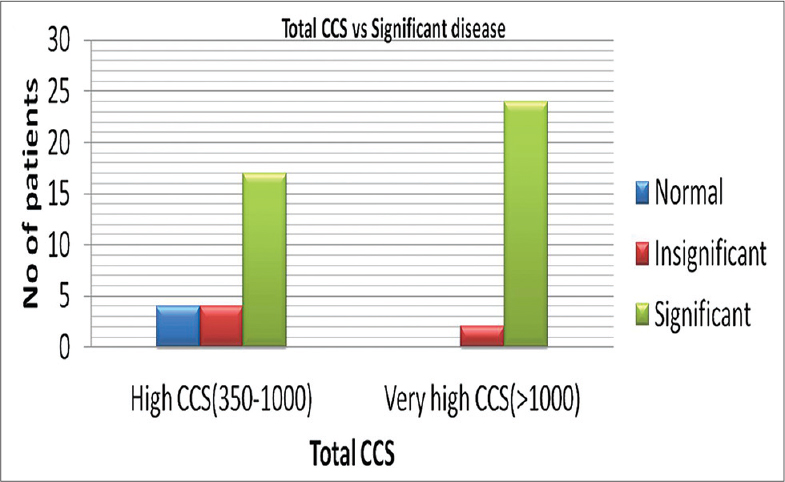
- Coronary calcium score versus significant lesion at patient level. Both high and very high coronary calcium score group have patients with significant disease. A subset of patients in the high coronary calcium score group has normal to insignificant disease.
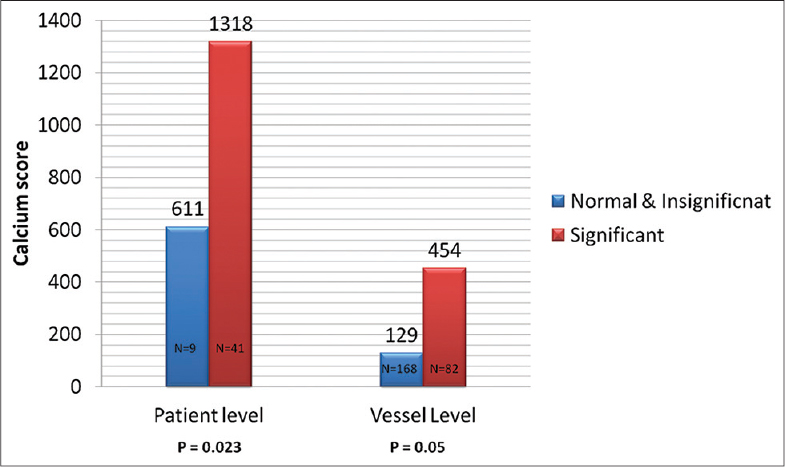
- Mean and standard error of calcium scores at patient and vessel levels with and without significant flow-limiting lesions. Patients and vessels with flow-limiting lesions have significantly higher coronary calcium score than those with normal or insignificant disease.
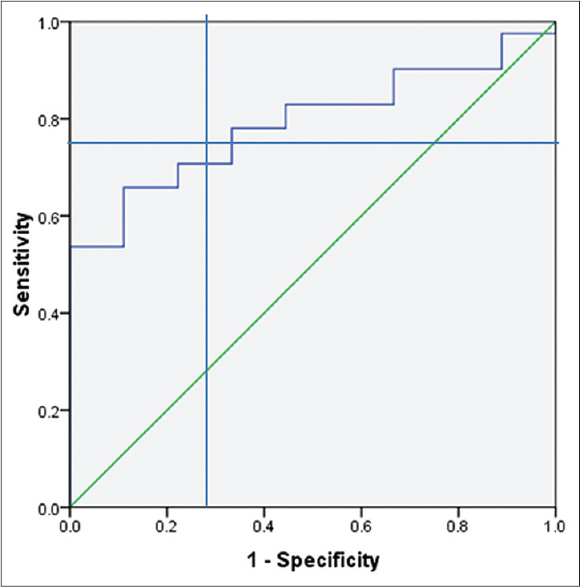
- Receiver operator curve of coronary calcium score and lesion severity at patient level. A total coronary calcium score of 777 and above has a sensitivity and specificity to predict significantly.
Coronary calcium score and lesion severity at vessel level
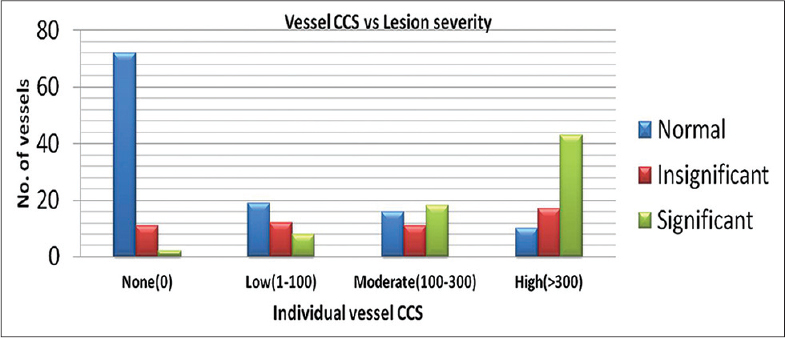
Of the 250 vessels analyzed, there were 168 vessels without significant stenosis and 82 vessels with significant stenosis. Of the 168 normal or vessels with insignificant lesions, only 52 had moderate to high calcium, whereas 61 out of the 82 vessels with significant lesions had moderate to high calcium [Table 3 and Figure 4]. When the individual vessel calcium scores were studied for association with any coronary lesion, there was a strong correlation with significant P value (r = 0.526, P < 0.01); however, the correlation for a significant lesion is weak (r = 0.29, P < 0.05). Conversely, the mean calcium scores for vessels without and with significant lesion were 129 ± 240 and 454 ± 497, respectively, which were significantly higher for vessels with flow-limiting lesions (P = 0.05). In the ROC analysis, an individual vessel score of 121 has a sensitivity and specificity of 70% to predict a flow-limiting lesion in the same vessel [Figure 5].
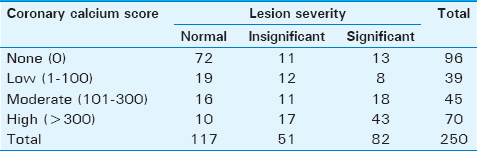
- Coronary calcium score versus lesion severity for individual vessels. At lower calcium scores per vessel, more number of vessels was normal, as the score increases more number of vessels have significant disease.
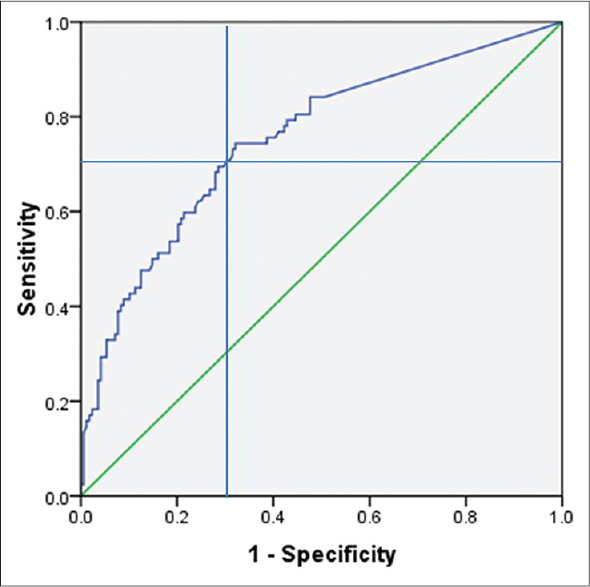
- Receiver operator curve of coronary calcium score and lesion severity at vessel level. A score above 120/vessel has a sensitivity and specificity of 70% to predict a significant stenosis in that vessel.
Coronary calcium score, SYNTAX score, and Framingham risk score
The mean SS for the whole study group was 15.9 ± 9.4; when stratified into high <1000 and very high >1000 groups, the very high group had a SS of 22.7 ± 6.9 and the high group had 9.5 ± 6.7. On comparing the CCS and the SS for association, there was strong significant correlation between the two among the whole cohort (r = 0.68, P < 0.01) [Figure 6] and the very high calcium group (r = 0.53, P < 0.01, n = 30) but not for the high calcium group (r = 0.1, P = 0.62, n = 20). The FRS correlated moderately with SS (r = 0.38, P = 0.006) and CCS (r = 0.46, P = 0.001). There is no significant gender-associated difference in the correlation between CCS and SS score (0.66 for females and 0.64 for males).
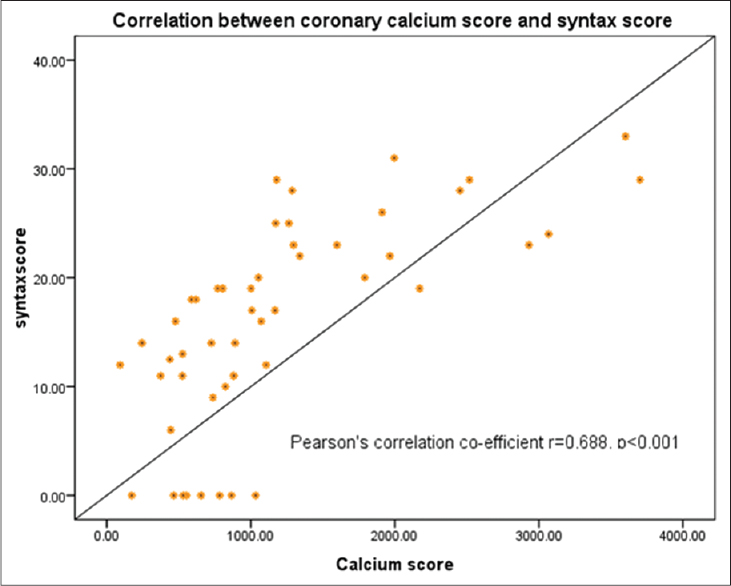
- Scatter plot of syntax score versus coronary calcium score. The syntax score increases with increasing coronary calcium score.
DISCUSSION
Calcium in the coronary arteries is believed to represent a dystrophic process, where the worn-out tissues of the aging vessels with plaques are replaced by calcium. This process is mediated by the calcium-binding glycophosphoprotein osteopontin.[5] According to the American Heart Association, staging of the coronary atherosclerotic plaques calcification is a feature of stage V, but with refined microscopic techniques micro calcification can be identified from stage III onward.[67] The location of calcification is also variable, which may be intimal, medial, or adventitial. As macroscopic coronary calcification is a late stage in the progress of atherosclerosis, in any cross-sectional autopsy series that included patients from all age groups, only 20% of plaques are found to be calcified.[3] Furthermore, the process of calcification indicates stabilization of plaques along with positive remodeling leading to compensation for the lumen loss caused by the plaque. It is for these reasons that the identification of coronary calcium though predicts the vascular age and the global atherosclerotic burden of the patient, and it is not specific for a vulnerable plaque or a significantly stenotic lesion.[8910] Supporting this fact, there are many reports of documented absent coronary calcium that was followed by acute coronary syndromes within months.[5] This has led to the discouragement of recommending calcium scoring as diagnostic rather than a screening test for risk stratification.[6] Another important indication of calcium scoring is before a proposed CTCA. Any CTCA protocol includes a plain scan at low radiation, and when that shows sufficiently high calcium known to interfere with final interpretation, the procedure might be abandoned. In such patients, conventional CA is the best modality for identifying significant lesions. Published literature on calcium scoring are mainly for risk stratification in asymptomatic subjects.[11] Based on large population-based studies, it has been shown to be of benefit in predicting cardiovascular events.[1213]
In our study, we have shown that a high coronary calcium correlates strongly and significantly with the global coronary plaque burden as derived by the SS. It was also found that the individual vessel calcium scores were correlating strongly with the presence of any lesion that may be anything above 30% narrowing, but only weakly with a significant stenosis defined by a luminal narrowing of ≥70% [Figure 7]. The sensitivity and specificity of calcium score to predict a significant lesion is higher at patient level than at vessel level which again reinforces the fact that CCS is a marker of global atherosclerotic burden rather than a marker of a focal significant lesion [Figure 8]. This was similar to other studies done on calcium scoring for identifying significant stenosis.[1415] It is also plausible with the pathogenesis of coronary calcification which occurs in older plaques rather than a significant plaque, and the majority of the coronary plaques are not significant but may be older and usually outnumber significant plaques by 3–5-fold. The SS mandates scoring for any lesion ≥50% stenosis in vessels that are ≥1.5 mm. As a result, borderline lesions also contribute to the overall score and hence correlating with CCS irrespective of the severity of lesion, not necessarily significant one. We have also found that SS correlated strongly with the FRS which is also pathogenetically plausible as FRS represents the vascular age based on the patients’ risk profile. The limitations of our study include the small number of patients included, but this could be compensated by the number of vessels studied, as both calcium scoring and lesions on CA were computed and analyzed for individual coronary arteries (LM, LAD, LCX, RCA, and PDA). The second limitation of our study could be that 70% of the studied population were high risk according to the 2008 FRS and so they are expected to have a higher vascular age. Hence, extrapolating this to the low and intermediate risk group may not hold true. It is also plausible that the high FRS would have confounded the strong correlation of the CCS with the SS, but the r value for CCS and SS is stronger than the r value for FRS and SS. This again reinforces the fact that CCS may have incremental value over and above the FRS for any given patient in predicting the atherosclerotic burden. We have a subtle evidence for the same in the form of loss of significant correlation of the CCS to SS in those with a total score <1000. The strength of our study includes the following: (1) the CCS is done by an experienced radiologist. (2) The CA was interpreted by two cardiologists with a third one validating any dispute. (3) The operators were blinded for the other scores.
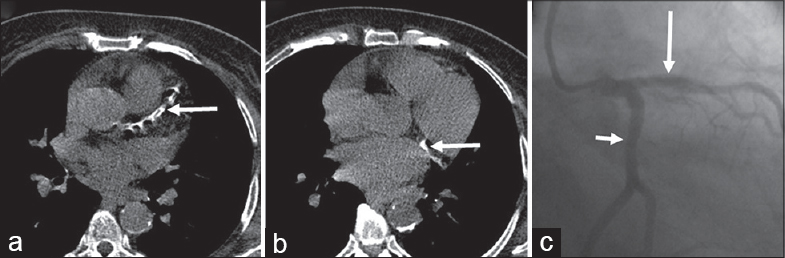
- Axial plain computed tomography images in a 45-year-old male show extensive calcification in the left anterior descending (a) and left circumflex (b) indicated by arrow; catheter angiogram (c) showing normal left anterior descending (long arrow) and left circumflex (short arrow).
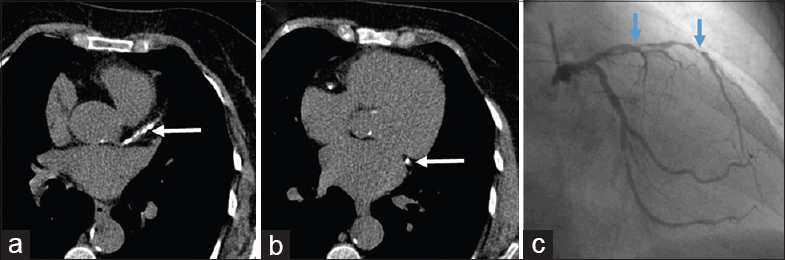
- Axial plain computed tomography images in a 53-year-male show extensively calcified left anterior descending (a) and left circumflex (b) indicated by arrow; catheter angiography image (c) showing multiple foci (arrows) of insignificant and significant stenosis in left anterior descending.
CONCLUSION
High CT calcium scores in this cohort of intermediate to high (Framingham score) risk patients correlated strongly with the subject's global burden of the CAD as derived by the SS, more so for subjects with very high scores. Similarly, high CCS predicted significant stenosis at both individual and arterial levels; also, the arterial vessel scores correlated strongly for any lesion but only weakly for the presence a significant stenosis. In spite of this association between CCS and the flow-limiting disease on conventional angiogram, a proportion of patients may still have insignificant disease when CCS is between 350 and 1000.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2016/6/1/46/193423
REFERENCES
- Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging. 2009;2:675-88.
- [Google Scholar]
- ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2007;49:378.
- [Google Scholar]
- Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: A histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol. 1998;31:126-33.
- [Google Scholar]
- Coronary angiography with multi-slice computed tomography. Lancet. 2001;357:599-603.
- [Google Scholar]
- Diffuse calcification in human coronary arteries. Association of osteopontin with atherosclerosis. J Clin Invest. 1994;94:1597-604.
- [Google Scholar]
- Coronary artery calcification: Pathophysiology, epidemiology, imaging methods, and clinical implications. A statement for health professionals from the American Heart Association. Writing Group. Circulation. 1996;94:1175-92.
- [Google Scholar]
- A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation. 1995;92:1355-74.
- [Google Scholar]
- Prognostic value of coronary calcification and angiographic stenoses in patients undergoing coronary angiography. J Am Coll Cardiol. 1996;27:285-90.
- [Google Scholar]
- Multidetector CT coronary angiography: Have we found the holy grail of non-invasive coronary imaging? Heart. 2005;91:1385-8.
- [Google Scholar]
- Coronary calcium does not accurately predict near-term future coronary events in high-risk adults. Circulation. 1999;99:2633-8.
- [Google Scholar]
- 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2010;56:e50-103.
- [Google Scholar]
- Electron beam computed tomographic coronary calcium score cutpoints and severity of associated angiographic lumen stenosis. J Am Coll Cardiol. 1997;29:1542-8.
- [Google Scholar]
- Probabilistic model for prediction of angiographically defined obstructive coronary artery disease using electron beam computed tomography calcium score strata. Circulation. 2000;102:380-5.
- [Google Scholar]
- 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol. 2007;50:1469-75.
- [Google Scholar]
- Coronary artery calcification detected with ultrafast CT as an indication of coronary artery disease. Radiology. 1992;185:435-9.
- [Google Scholar]




