
Translate this page into:
Spectrum of High Resolution Computed Tomography Findings in Occupational Lung Disease: Experience in a Tertiary Care Institute
Address for correspondence: Dr. U. C. Ojha, Director, Institute of Occupational Health, Education and Research, Employee's State Insurance Hospital and Post Graduate Institute of Medical Science and Research, Basaidarapur, New Delhi, India. E-mail: ucojha@rediffmail.com
-
Received: ,
Accepted: ,
This is an open‑access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
To study the spectrum of high resolution computed tomography (HRCT) findings in occupational lung disease in industrial workers and to assess the utility of International classification of HRCT for occupational and environmental respiratory diseases (ICHOERD).
Materials and Methods:
Retrospective analysis of radiological data (radiographs and computed tomography chest scans) gathered over a period of 3 years (January 2010- December 2012) of industrial workers in an organised sector who presented with respiratory complaints. The HRCT findings were evaluated using ICHOERD.
Results:
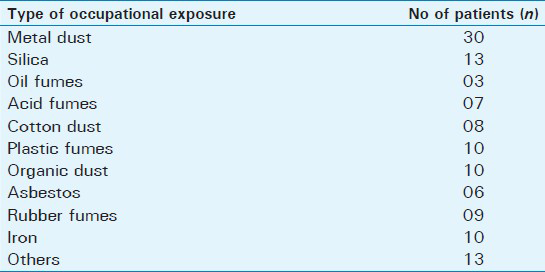
There were 5 females and 114 males in the study, with a mean age of 49 years. These workers were exposed to different harmful agents including silica, asbestos, cotton dust, metal dust, iron oxide, organic dust, rubber fumes, plastic fumes, acid fumes, and oil fumes. There were 10 smokers in the study. The radiograph of chest was normal in 53 patients. 46% of these normal patients (21.8% of total) demonstrated positive findings on HRCT. When the radiograph was abnormal, HRCT provided more accurate information and excluded the other diagnosis. The HRCT findings were appropriately described using the ICHOERD. Bronchiectasis was the most common finding (44.5%) with mild central cylindrical bronchiectasis as the most common pattern. Pleural thickening was seen in 41 patients (34.5%). Enlarged hilar or mediastinal lymphnodes were seen in 10 patients (8.4%) with egg-shell calcification in 1 patient exposed to silica. Bronchogenic carcinoma was seen in 1 patient exposed to asbestos.
Conclusions:
Occupational lung disease is a common work related condition in industrial workers even in the organized sector. Though chest radiograph is the primary diagnostic tool, HRCT is the undisputed Gold Standard for evaluation of these patients. Despite the disadvantage of radiation exposure, low dose CT may serve as an important tool for screening and surveillance. The ICHOERD is a powerful and reliable tool not only for diagnosis, but also for quantitative and analytical measurement of disease, thereby contributing to assessing the medical epidemiology of lung disease. It should always be used while evaluating HRCT of a patient with occupational lung disease.
Keywords
Classification
high resolution computed tomography
ICHOERD
industrial worker
occupational lung disease

INTRODUCTION

Despite federally mandated safety standards, the incidence of occupational or work environment related lung disease is on the rise. There is a widely used system for classification of chest radiographic abnormalities in pneumoconiosis introduced by the International Labour Office (ILO).[1] Though the introduction of high-resolution computed tomography (HRCT) has revolutionized the diagnosis of occupational lung disease, a comprehensive system for the classification and quantification of these lung abnormalities on HRCT is still not in common use. The awareness about the radiological manifestations of occupational lung disease is limited with ambiguity associated with the terminology and description of radiological manifestations.
In the present study, imaging features on HRCT chest scans of industrial workers were evaluated using the International classification of HRCT for occupational and environmental respiratory diseases (ICHOERD).[2] The HRCT findings were also compared with those seen on traditional chest radiographs.
MATERIALS AND METHODS
A retrospective analysis was done of the chest radiographs and computed tomography (CT) scans of 150 industrial workers from an organized sector, who attended an Institute of occupational and environmental health center in a tertiary care setup for medical check-up over a period of 3 years (January 2010-December 2012). Thirty-one patients were excluded based on clinical and/or radiological diagnosis that indicated lesions other than occupational lung disease. Exclusion criteria included signs/symptoms or imaging appearances on CT/X-ray suggestive of pulmonary disease secondary to infection, trauma, congenital diseases, smoking, connective tissue disorders, or any other disease known to produce similar manifestations. There were 119 patients with a diagnosis of occupational lung disease, who formed the subjects of this study. The demographic profile (age/sex), detailed occupational history, and history of smoking were recorded for these patients. The radiological records, including radiograph of chest in posteroanterior view and high resolution computed tomography scan of thorax, were evaluated. The findings on HRCT were evaluated using ICHOERD classification.
RESULTS
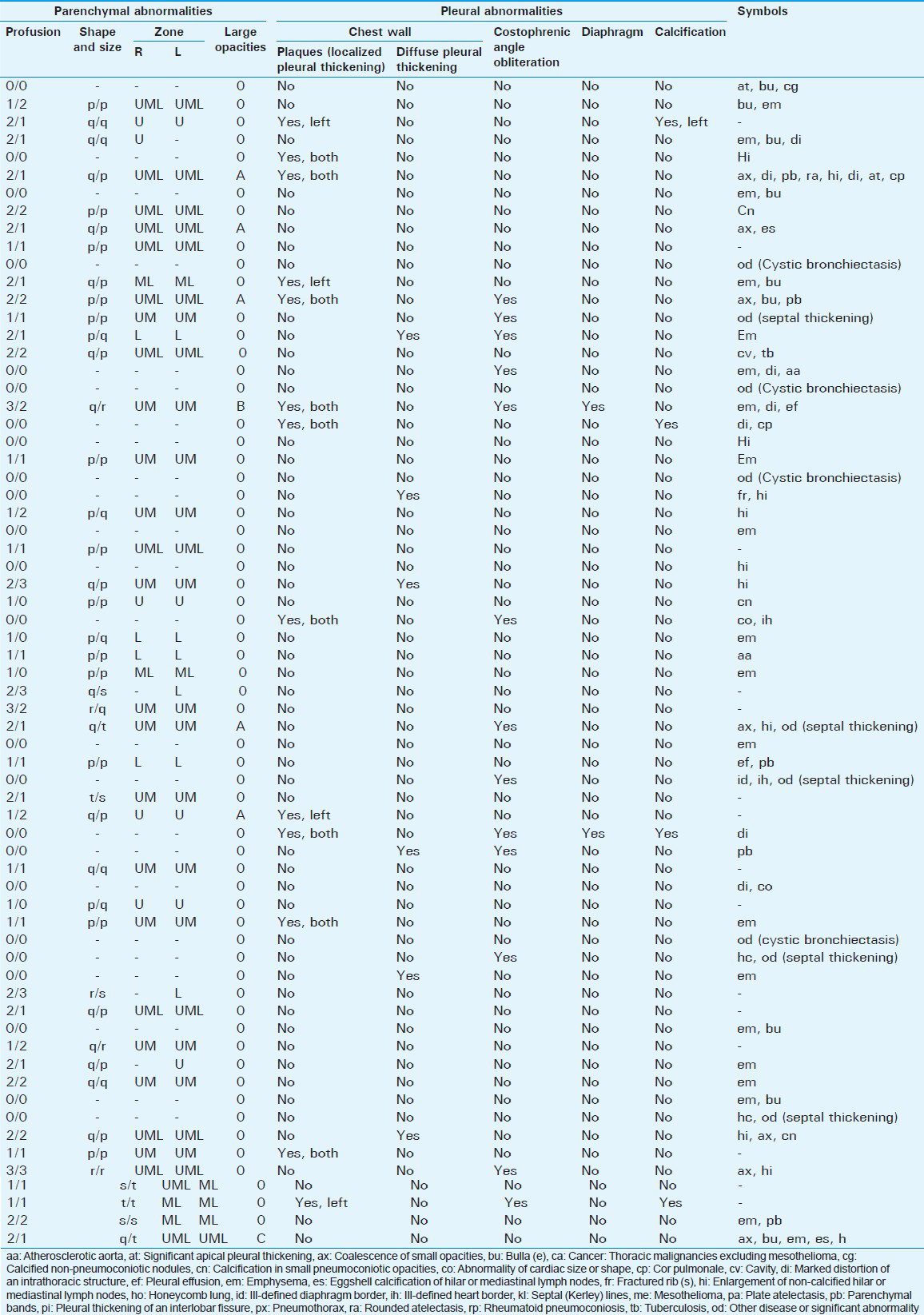
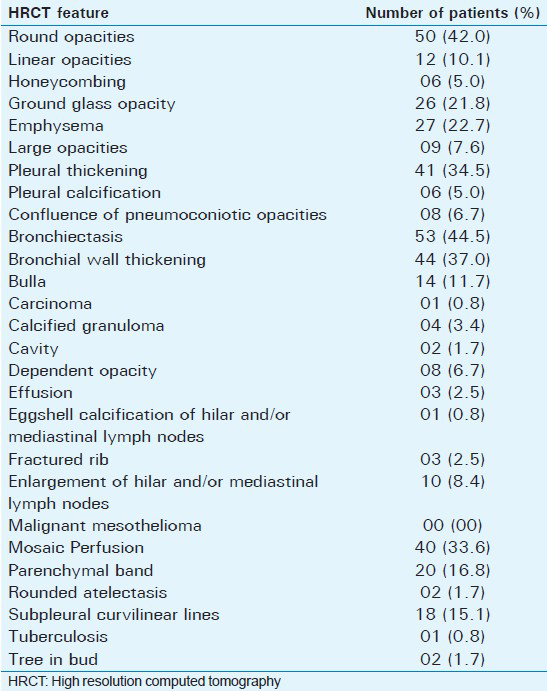
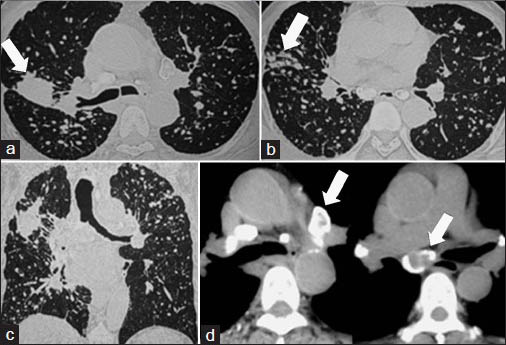
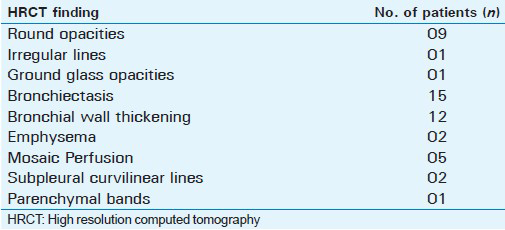
There were 5 females and 114 males in the study. Their ages ranged from 31 years to 74 years, mean age being 49 years. These workers had been exposed to different types of hazardous agents as detailed in Table 1. There were 10 smokers in the study. The radiograph of chest was normal in 53 patients. Out of these, 26 patients demonstrated positive findings on HRCT [Figures 1 and 2]. The chest radiograph findings in 66 patients with positive X-ray are tabulated in Table 2. The various HRCT findings observed are listed in Table 3. Bronchiectasis was the most common finding with mild central cylindrical bronchiectasis as the most common pattern [Figure 3]. This was associated with bronchial wall thickening and mosaic attenuation. Pleural thickening was seen in 41 patients (34.5%). Hilar or mediastinal lymphnodes were enlarged in 10 patients (8.4%) with egg- shell calcification seen in 1 patient exposed to silica. Bronchogenic carcinoma developed in one patient exposed to asbestos.
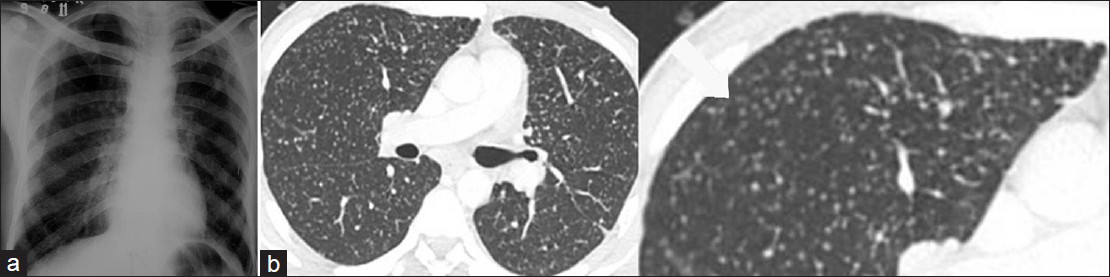
- 54-year-old man working as stone cutter for 25 years with simple silicosis on HRCT and normal chest radiograph. (a) Radiograph of chest in posteroanterior view shows no abnormality. (b) HRCT thorax in axial plane: Multiple small well defined nodules, round opacities (RO type P) (arrows) seen in bilateral upper lobes.

- 57-year-old construction worker with early asbestosis on HRCT and normal chest radiograph. (a) Chest X-ray is normal. (b) Axial HRCT prone image in lung window demonstrates subtle intralobular septal thickening and ground glass opacity in lower lobes in subpleural distribution.

- 44-year-old woman exposed to rubber fumes for 15 years. Axial HRCT image in lung window shows minimal central cylindrical bronchiectasis (BE) with bronchial wall thickening (BR) (arrows). This was the most common HRCT finding seen in present study, consistent with airway disease.
In patients with history of exposure to silica (N = 13), presence of rounded opacities (RO) [Figure 4] was the most common manifestation (9/13). The type of RO predominantly seen was Q, and showed upper lobe predominance. Progressive massive fibrosis [Figure 5] was seen in 2/13 patients and HRCT was normal in 2/13 patients. There was lymphadenopathy in 3/13 patients with egg-shell (ES) calcification seen in 1 of them [Figure 6]. Two patients demonstrated the presence of irregular lines (IR) (intralobular/interlobular septal thickening) with associated ground glass opacity (GGO). Minimal central cylindrical bronchiectasis was seen in 5/13 patients.

- 47-year-old woman working as stone grinder diagnosed with simple silicosis. (a) Axial HRCT image in lung window show small round opacities (RO type P and Q) in bilateral upper lobes.
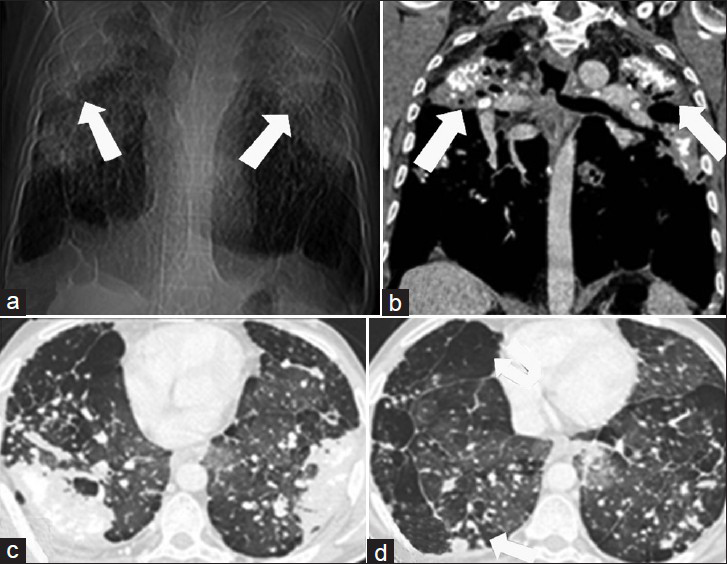
- 61-year-old man construction worker with silicosis and progressive massive fibrosis. (a) Computed tomography topogram shows large bilateral opacities in the upper zones of the lung with large emphysematous bullae in lower lobes. (b) Coronal CT scan obtained with mediastinal window settings shows bilateral conglomerate masses with calcifications (arrows). (c and d) Axial HRCT images in lung window, show presence of round opacities (RO) with paraseptal emphysema (EM) in addition.

- 52- year-old foundry worker with silicosis and progressive massive fibrosis. Axial contrast enhanced computed tomography image in mediastinal window shows egg-shell calcification of mediastinal and hilar lymph nodes (arrows).
In six patients with history of exposure to asbestos, one demonstrated normal HRCT. 3/6 patients demonstrated the presence of IR (intralobular septal thickening) with GGO, with peripheral subpleural distribution [Figure 7]. Honeycombing was observed in two patients, pleural plaques in three patients with pleural calcification in one patient. Round atelectasis was seen in one patient. One patient demonstrated the presence of right upper lobe malignant mass with malignant mediastinal lymphadenopathy and right pleural effusion [Figure 8].

- 69-year-old man working in brake shoe lining manufacturing industry with lung disease. (a) Computed tomography in axial lung window (a) shows irregular lines (IR), predominantly intralobular septal thickening with ground glass opacity seen in bilateral lungs in peripheral subpleural distribution. (b) Contrast enhanced computed tomography, axial image in mediastinal window shows pleural calcification (arrows). These findings are suggestive of asbestos related lung disease.
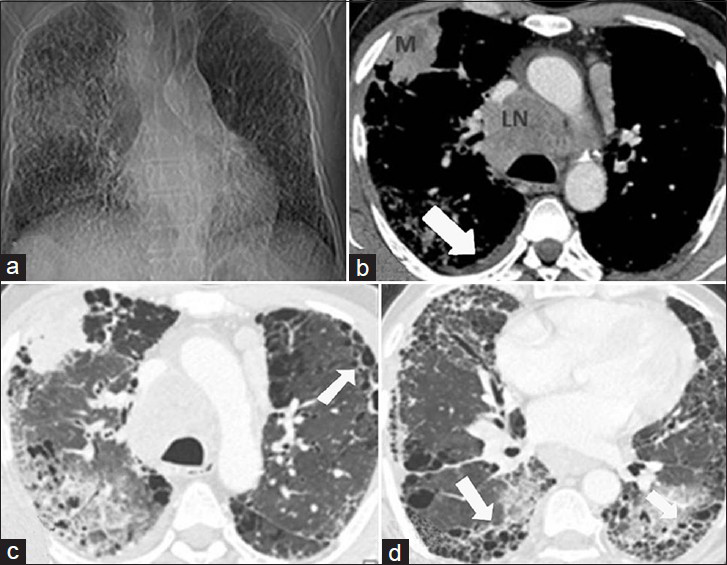
- 71-year-old man with asbestos related lung disease and bronchogenic carcinoma. (a) CT topogram shows presence of reticular opacities in bilateral lung parenchyma with an ill-defined mass in right upper zone. (b) Axial contrast enhanced CT demonstrates presence of a malignant mass (M) with mediastinal lymphadenopathy (LN) and right pleural effusion (arrow). (c and d) Axial HRCT images in lung window show evidence of intralobular septal thickening with honeycombing (arrows), findings consistent with advanced asbestosis.
In patients exposed to cotton dust (N = 8), two demonstrated normal HRCT. Minimal central cylindrical bronchiectasis (BE) with bronchial wall thickening (BR) and associated mosaic attenuation was the most frequently observed manifestation, seen in 3/8 patients. One patient demonstrated emphysema whereas parenchymal bands were the only manifestation in one of them. RO with predominant pattern P with confluent opacities at places and GGO were seen in one patient. This was associated with emphysema, bullae, and pleural thickening.
3/6 patients exposed to rubber fumes showed normal HRCT. Minimal central cylindrical BE with BR and associated MP was seen in other three patients. IR (interlobular septal thickening) with GGO was seen in 2/6 patients.
Exposure to plastic fume also resulted in 6/10 patients demonstrating a predominant pattern of minimal central cylindrical BE, BR, and MP [Figure 9]. There were associated fine centrilobular nodules (RO) in five patients. HRCT was normal in 3/10 patients and RO was the only manifestation in one patient.
- 38-year-old woman with plastic fumes exposure. Axial HRCT image in lung window shows presence of minimal central cylindrical bronchiectasis (BE) with bronchial wall thickening (BR) (arrows). Patient demonstrated obstructive pattern of abnormality on spirometry.
Three out of ten patients exposed to iron oxide fumes (siderosis) showed normal HRCT. The predominant appearance of RO in the upper lobe was seen in 4/10 patients [Figure 10]. One patient demonstrated IR (interlobular septal thickening), with GGO and HC. Emphysema was seen in two patients with BE and BR in 5/10 patients.

- 53-year-old man working as electric arc welder for 28 years diagnosed with siderosis. (a) Radiograph of chest in posteroanterior projection is unremarkable. (b) Axial HRCT image in lung window shows presence of small, round opacities (RO type P) in bilateral upper lobes. There are associated patchy areas of ground glass attenuation (GGO).
Two patients exposed to organic dust demonstrated normal HRCT. BE with BR and MP was seen in 4/10 patients. IR with GGO was seen in three patients with honeycombing in one of them. Emphysema, predominantly paraseptal, and bullae formation was seen in three patients.
Patients exposed to metal dust (n = 30) showed RO as the most common radiological manifestation (16/30). Five patients had normal HRCT. The next most common appearance was bronchiectasis with bronchial wall thickening, seen in 11 patients. Uncommon appearance included GGO (5/30), parenchymal bands (6/30), subpleural curvilinear opacities (3/30) and emphysema (3/30). IR comprising predominantly interlobular septal thickening were evident in two patients with the presence of honeycombing in one of them [Figure 11]. Lymphnodes were enlarged in three patients [Figure 12].

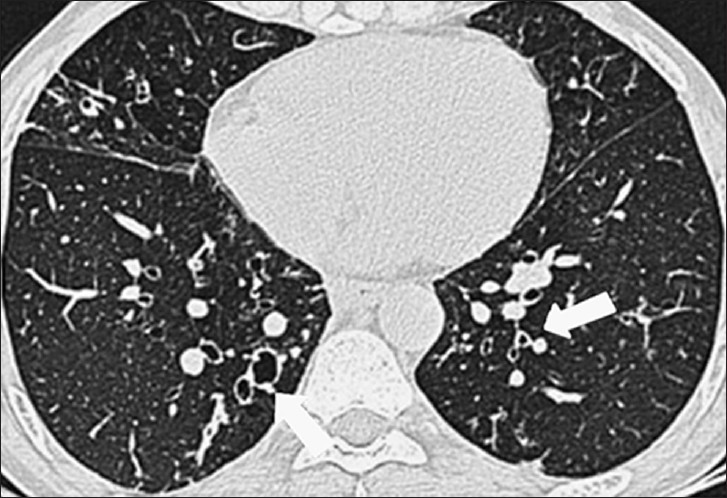
- 50-year-old man with exposure to aluminum dust for 30 years. Axial HRCT image in lung window shows interlobular and intralobular septal thickening and honeycombing in upper lobes.

- 45-year-old woman working in dental prostheses manufacturing unit with chronic berylliosis. Axial CT image in mediastinal window demonstrate mediastinal lymphadenopathy (arrow).
In patients with chronic obstructive airway disease (COAD), i.e.,with the clinical diagnosis of asthma and chronic obstructive pulmonary disease (COPD) and finding of bronchiectasis, bronchial wall thickening and mosaic pattern decreased after the patient was no longer exposed to the hazardous agents in the work environment and their overall response to bronchodilator was good. Their response to treatment was similar to those with COAD due to other causes. Overall, patients with asthma responded better to the treatment than the chronic obstructive pulmonary disease (COPD) patients. Those with interstitial lung disease (ILD), especially idiopathic pulmonary fibrosis (IPF) had progressive worsening of respiratory disease. The worsening was however slower than that seen in patients with IPF not caused by exposure to metal dust. Patients with progressive massive fibrosis, carcinoma of lung, and asbestosis had gradual worsening of symptoms even leading to death.
Limitations
This study had certain limitations. The study was a retrospective study. The number of subjects in each subgroup was very small. Also, the pulmonary manifestation may result from exposure to a combination of agents at the work place and not one particular agent. In the present study, effort was made to select patients with one predominant exposure, leading to selection bias. Also, histopathological confirmation was not available in every case.
DISCUSSION
Occupational lung diseases are a group of illnesses that are caused by either repeated, extended exposure or a single, severe exposure to irritating or toxic substances that leads to acute or chronic respiratory ailments.[3] It is the most common work-related condition after injuries and includes pneumoconiosis, asbestos-related pleural and parenchymal disease, chemical pneumonitis, infection, hypersensitivity pneumonitis, and organic dust toxic syndrome. Pneumoconiosis may be clinico-pathologically classified as fibrotic or non-fibrotic, depending upon the absence or presence of fibrosis.
Imaging plays an indispensable role in the evaluation of patients with suspected occupational lung disease. The radiograph of chest is the first and most important diagnostic tool for evaluation. It is easily available and inexpensive. It can be highly suggestive of an occupational disorder and may be sufficient to establish a diagnosis in certain cases [Figure 13]. Considering this fact, the classification system of chest radiographic abnormalities in pneumoconiosis introduced by the ILO has been widely used. However, despite the well-established role of chest radiography in accurately and inexpensively displaying a wide range of pulmonary pathology, equally well-established limitations have been documented. The findings can be non-specific and the sensitivity low, missing as many as 10 to 15 percent of cases with pathologically documented disease. In the present study also, 26 out of 53 patients (46.4%) with a normal radiograph demonstrated abnormal findings on HRCT [Table 4]. In a study by Begin et al.,[4] 41% patients interpreted as normal on chest radiograph demonstrated the evidence of silicosis on HRCT. In patients with significant asbestos exposure but no evidence of asbestosis on chest radiograph, 20-30% demonstrate abnormal HRCT findings consistent with the disease.[5]
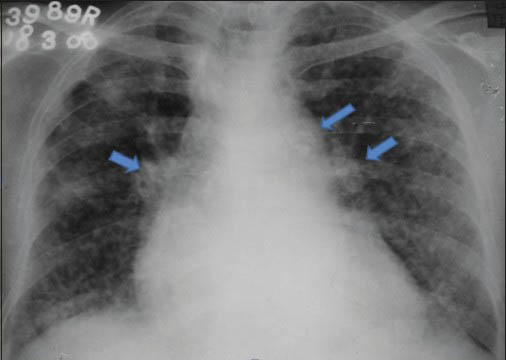
- 45-year-old man working in glass industry diagnosed with silicosis. (a) Radiograph of chest in posteroanterior projection shows multiple nodules in bilateral lung parenchyma with calcified mediastinal and hilar lymphnodes (arrows). These findings in association with appropriate history of exposure are diagnostic of silicosis.
- HRCT thorax of the same patient. (a and b) Axial and (c) coronal images in lung window: Multiple round opacities (RO type P) seen in bilateral lung parenchyma with upper zone predominance. There is evidence of confluence (AX) (arrow in b) and a large opacity (arrow in a) seen in posterior segment of right upper lobe. (d) Axial image in mediastinal window show calcified hilar and mediastinal lymphnodes with egg-shell calcification (arrows).
It has been proved undisputedly that CT, particularly high-resolution CT (HRCT), is superior to chest radiography in the detection of parenchymal abnormalities, more accurate in providing the differential diagnosis, and free from considerable inter-observer variation in its interpretation. The application of CT to the occupational lung diseases attempts to relate morphological feature of respiratory manifestation more closely to existing pathology. It is even indicated as a tool for further investigation of positive cases screened by chest radiograph.
The radiological findings on HRCT were evaluated using ICHOERD in the present study. The most common finding was bronchiectasis with bronchial wall thickening. This finding correlates with occupational asthma and chronic obstructive airway disease (COAD). Occupational asthma represents the most common form of occupational lung disease.[3]
Simple silicosis is characterized by the presence of multiple small nodules, 2–5 mm in diameter, accompanied by calcifications.[6] The distribution may be diffuse, though upper lobe with posterior zone predominance is characteristic. In the present study also, type Q round opacities was the most common finding (69.2%) in patients. Egg-shell pattern of calcification of lymph nodes though characteristic is seen in 5% cases,[7] as in the present study (1/13, 7.7%). Silicosis predisposes the affected individual to pulmonary tuberculosis and carcinoma with increased risk of chronic interstitial pneumonia and subsequent fibrosis, most commonly usual interstitial pneumonia (UIP).[8] Irregular lines were seen in two patients with exposure to silica.
Asbestos-related conditions in the chest include pleural effusion, pleural plaques, diffuse pleural thickening, rounded atelectasis, asbestosis, mesothelioma, and lung carcinoma.[9] Pleural plaques are the most common manifestation of asbestos-related pleural disease. Mesothelioma and bronchogenic carcinomas can arise in the setting of asbestos exposure. In the present study, pleural pathology comprising of pleural plaques, pleural calcification, and round atelectasis were observed in 50% of the patients exposed to asbestos. IR was also seen in half of the patients with exposure to asbestos. One patient developed bronchogenic carcinoma.
HRCT appearance in siderosis includes widespread ill-defined small centrilobular nodules and less often patchy areas of ground-glass attenuation without zonal predominance.[10] Emphysema is commonly seen. Though siderosis is not usually associated with fibrosis or functional impairment and traditionally considered a benign pneumoconiosis, symptomatic disease with interstitial fibrosis has been described in arc welders.[11] In the present study, the most common appearance secondary to iron exposure was airway abnormality (BE and BR), followed by round opacities (40%). Evidence of fibrosis was seen in one patient.
Cotton-induced airways disease is common; however, pulmonary fibrosis and pneumoconiosis due to cotton dust have also been reported in a few cases.[12] In the present study also, BE with BR and associated MP was the most common HRCT finding in patients exposed to cotton dust, indicating the presence of airway disease.
The most common radiological manifestations in plastic fumes and rubber fume exposure was also BE and BR, related to the presence of a disease of the air passages. RO was the most common manifestation of metal dust exposure. The best characterized occupational ILD secondary to metal dust and fume exposure is chronic berrylium disease (CBD). HRCT findings of chronic berylliosis are similar to sarcoidosis and include small nodules with peribronchovascular distribution, smooth or nodular interlobular septal thickening, ground-glass opacity, and bronchial wall thickening.[13] Mediastinal and hilar lymphadenopathy is seen in about 25% of patients (with CBD). HRCT findings of hard metal pneumoconiosis consist of bilateral ground-glass opacities, tiny nodules, reticular opacities, traction bronchiectasis, and consolidation. In aluminium dust pneumoconiosis, HRCT findings include subpleural or diffuse honeycombing resembling idiopathic pulmonary fibrosis (IPF), centrilobular nodules resembling silicosis, or irregular reticulation with upper lobe predominance.[14]
Since HRCT is fundamental for the quantification of disease severity and the prognosis and identification of coexisting or alternative diseases, a standardized quantification scheme should be available for occupational lung diseases using CT. There should be a comprehensive system for the classification and quantification of the lung abnormalities typically seen in patients with pneumoconiosis. A classification system, similar to the ILO system, should be implemented to accurately diagnose and effectively prevent these diseases.
Current information available for recognising imaging findings on HRCT that is suggestive of occupational lung disease lacks sensitivity. The descriptive system used is ambiguous and the inter-observer variation in reporting high. To make the use of HRCT efficient and effective the International Classification of HRCT for Occupational and Environmental Respiratory Diseases (ICHOERD) should be brought into use. This classification provides a detailed and comprehensive description of significant HRCT findings and methods for appropriately recording them. All aspects of the HRCT diagnosis of pneumoconiosis, including the technical aspects of CT, radiation exposure, use of appropriate terminology in description of abnormalities, coding systems (including a review of the ILO system), and pathologic correlations have been considered. It assists in diagnostic evaluations of dust-exposed individuals and provides a tool for quantitative and analytical measurement of disease. It makes the use of a standard scale, thus eliminating non-specific terminology such as mild, moderate, and severe. The observations are noted in a more quantitative and comparative way. Accumulation of clinical data in a standardized format using the HRCT Classification system helps to gather clinical epidemiological data. If the Classification system is introduced into many hospitals and clinics, data on dust-exposed individuals screened by HRCT can be collected and distributed to workplaces so as to establish an effective surveillance system. Standardization of the reporting system would enable global sharing of experiences and data.
CONCLUSION
Occupational lung disease is a diverse group of preventable pulmonary diseases that accounts for a significant portion of diffuse lung disease in industrial workers. Imaging plays an important role in evaluation of such patients. Though chest radiograph is the first most important diagnostic tool, HRCT has become the Gold Standard in evaluation of patients with suspected occupational lung disease. Despite the primary disadvantage of radiation exposure involved in chest CT, surveillance and screening with CT may be a preferable tool when compared with conventional radiography, especially if a standardized approach to classification is widely accepted and applied. The International Classification of High-Resolution Computed Tomography for Occupational and Environmental Respiratory Diseases serves this purpose. It not only assists in diagnostic evaluations of occupational lung disease, but also provides a tool for quantitative and analytical measurement of disease, and contributes to study of the epidemiology of the disease.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/64/124097
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Guidelines for the use of ILO international classification of radiographs of pneumoconioses, Revised Edition 1980, Occupational Safety and Health series 22 (rev. 80)
- [Google Scholar]
- International Classification of HRCT for Occupational and Environmental Respiratory Diseases. Tokyo: Springer-Verlag; 2005.
- [Google Scholar]
- Computed tomography scan in the early detection of silicosis. Am Rev Respir Dis. 1991;3:1.
- [Google Scholar]
- Pulmonary fibrosis in asbestos insulation workers with lung cancer: A radiological and histopathological evaluation. Br J Ind med. 1987;44:96-100.
- [Google Scholar]
- Chronic diffuse infilterative lung disease; determination of the diagnostic value of clinical data, chest radiography, and CT with Bayesian analysis. Radiology. 1994;194:383-90.
- [Google Scholar]
- Chronic interstitial pneumonia in silicosis and mix-dust pneumoconiosis: Its prevalence and comparison of CT findings with idiopathic pulmonary fibrosis. Chest. 2007;131:1870-6.
- [Google Scholar]
- Asbestos: When the dust settles an imaging review of asbestos-related disease. RadioGraphics. 2002;22(spec No):S167-84.
- [Google Scholar]
- Pulmonary fibrosis secondary to siderosis causing symptomatic respiratory disease: A case report. J Med Case Rep. 2008;2:257.
- [Google Scholar]




