
Translate this page into:
Role of Noninvasive Imaging of Cerebral Arterial System in Ischemic Stroke: Comparison of Transcranial Color-coded Doppler Sonography with Magnetic Resonance Angiography
Address for correspondence: Dr. Shyamkumar Nidugala Keshava, Department of Radiodiagnosis, Christian Medical College, Vellore - 632 004, Tamil Nadu, India. E-mail: aparna_shyam@cmcvellore.ac.in
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim:
To determine the accuracy of transcranial color-coded Doppler sonography (TCCS) in the evaluation of cerebral arterial system in patients with ischemic stroke attending a tertiary care hospital in South India.
Objectives:
(1) To describe the topographical distribution of atherosclerotic lesions in the cerebral circulation in patients presenting with ischemic stroke from the Indian subcontinent and (2) to determine the accuracy of TCCS for detection and quantification of intracranial stenoses in various segments of the intracerebral arterial system in comparison with magnetic resonance angiography (MRA).
Materials and Methods:
The demographic profile and risk factors of consecutive patients who presented to neurology outpatient department with cerebral ischemia and scheduled for MRA were determined. These patients had undergone neck Doppler, TCCS, and MRA. The agreement between the MRA and TCCS was assessed using kappa statistics. The sensitivity, specificity, and positive and negative predictive values of TCCS as compared to MRA were calculated.
Results:
Ninety patients were included in the final analysis. Intracranial atherosclerosis was found in 35.6% of cases. The agreement between TCCS and MRA in detecting lesions for the different arterial segments in the intracranial circulation was 0.83 for anterior cerebral artery (ACA), 0.66 for M1 segment of middle cerebral artery (MCA), 0.45 for M2 segment of MCA, 0.86 for terminal internal carotid artery (TICA), 0.46 for posterior cerebral artery (PCA), and 0.81 for vertebral artery (VA). The sensitivity for the detection of hemodynamically significant arterial lesions in different vascular segments was 100%, 70%, 33.3%, 90.9%, 33.3%, and 72.7% for ACA, M1, M2, TICA, PCA, and VA, respectively.
Conclusion:
Intracranial atherosclerosis was found to be the predominant distribution of cerebral atherosclerosis. TCCS is a safe method for evaluation of proximal basal cerebral arteries in the intracranial circulation with relatively better sensitivity in the anterior circulation.
Keywords
Cerebral arterial system
ischemic stroke
magnetic resonance angiography
transcranial color-coded Doppler sonography


INTRODUCTION
Stroke, which occurs when blood flow to the region of the brain is interrupted, is a major cause of death and disability in the population. It is the second-most common cause of death worldwide.[1] Ischemic stroke accounts for about 87% of all strokes.[2] Atherosclerosis causing thrombosis and resultant narrowing or occlusion of vessels is the most common cause of ischemic stroke.[34]
Racial differences in the distribution of cerebral atherosclerosis is well established in many studies.[567] Intracranial atherosclerotic stenosis is responsible for ischemic strokes in only 6%–10% of White patients but up to 29% of African-American and Asian patients,[3] with 3-fold increased risk of intracranial atherothrombosis reported in South Asian patients.[8]
Transient ischemic attack (TIA) is an important risk factor for recurrent stroke which is a major cause of increased mortality and morbidity.[9] Hence, the importance of recognizing this event and prompt evaluation for disease extent to start early treatment which will reduce new or severe stroke subsequently. There has been an increasing focus on this secondary prevention of stroke in the recent years.[101112]
Advances in low-frequency Doppler ultrasound as well as imaging resolution, color flow Doppler, and power Doppler have led to the use of these technologies for interrogation of intracranial circulation through the intact skull. Doppler combines the advantages of hemodynamic information, cost-effectiveness, and bedside application. It is safe, noninvasive, fast, and repeatable. Transcranial color-coded Doppler sonography (TCCS) may particularly be useful in patients who require repeated imaging.
This study was done to determine the accuracy of TCCS in evaluation of the cerebral arterial system in patients with ischemic stroke or TIA presenting to a tertiary care center in South India.
MATERIALS AND METHODS
Consecutive patients who presented to the neurology outpatient department during the study (March to October 2009) with a history of cerebral ischemia (TIA or ischemic stroke) and who were planned for magnetic resonance angiography (MRA) as part of evaluation were included in this study after obtaining informed consent.
The exclusion criteria included patients who have had a previous vascular surgery (endarterectomy) or endovascular procedures such as carotid stenting, age <35 years, hemorrhagic stroke, hyperacute stroke, and patients who lacked a suitable acoustic window for TCCS.
Using sensitivity of 94% (based on a previous review),[13] precision index of 6, and 95% confidence interval, we calculated the sample size for those positive for intracranial disease on MRA to be 40 cases.
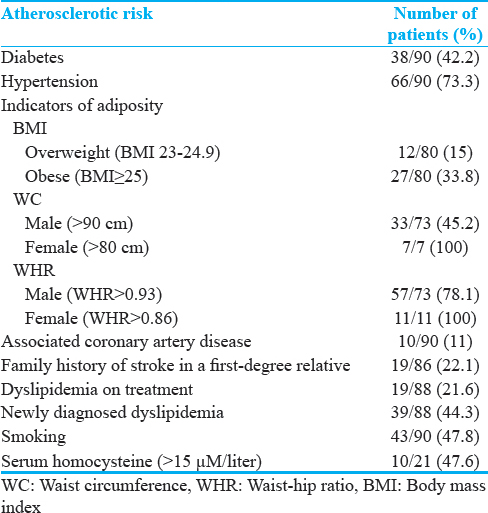
The risk factor profiles determined included age, gender, indicators of adiposity (body mass index [BMI], waist circumference [WC], and waist–hip ratio [WHR]), diabetes mellitus, hypertension, coronary artery disease, dyslipidemia, family history, smoking, and serum homocysteine levels. The National Cholesterol Education Program Adult Treatment Panel III uses a higher cutoff for WC, which may not be reflective of central obesity in our population; hence, the cutoffs we used were WC >90 and >80 in men and women, respectively.[14] Men with WHR ≥0.93 and women with WHR ≥0.86 had significantly increased risks of ischemic stroke in simple and multivariate models.[15] These were the cutoffs used in our study. The BMI was calculated with the Indian cutoffs based on the standards set by the Indian Health Ministry's consensus guidelines for the prevention and management of obesity and metabolic syndrome for the country. The cutoffs used were as follows: <18.4 – underweight, 18.5–22.9 – normal, 23–24.9 – overweight, and >25 – obese.
Hyperhomocysteinemia has been linked to various vascular events including carotid artery stenosis.[16] This association has been described mostly for extracranial carotid artery stenosis.
The patients were classified into the subtypes of ischemic stroke based on the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification, which is based on clinical symptoms as well as results of further investigations. Accordingly, stroke is classified as being due to (1) thrombosis or embolism due to atherosclerosis of a large artery, (2) embolism of cardiac origin, (3) occlusion of a small blood vessel, (4) other determined causes, and (5) undetermined cause (in case two possible causes or no cause identified, or incomplete investigation).[17] Associated presence of leukoaraiosis (white matter hyperintensities) was also documented.
A neck Doppler was performed to evaluate atherosclerotic lesions in the common carotid artery, extracranial internal carotid artery (ICA), and vertebral arteries (VAs). The percentage degree of stenosis of the extracranial ICA was stratified based on the consensus panel gray scale and Doppler US criteria for diagnosis of ICA stenosis.[18] Neck Doppler was performed on Xario SSA 660A, Toshiba Medical Systems Corporation, using an 8–12 MHz linear probe.
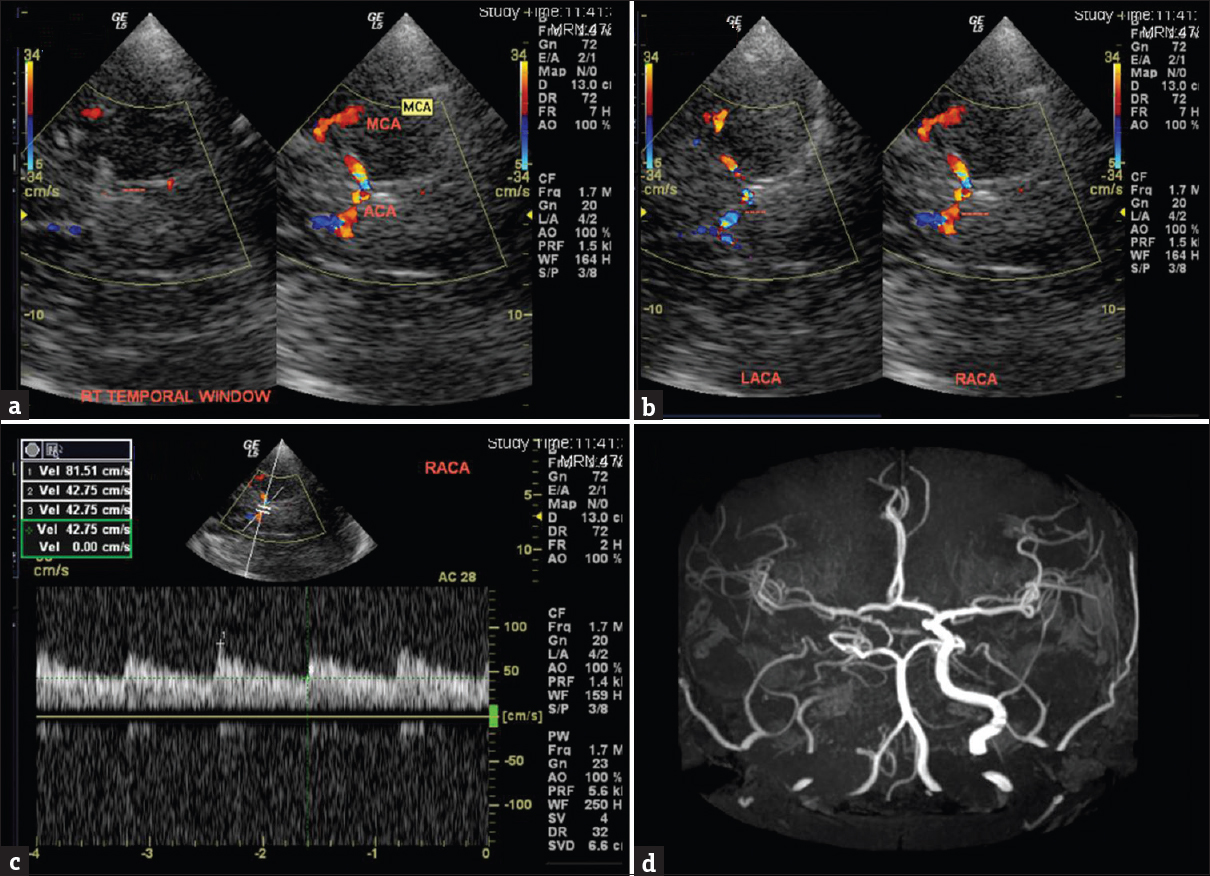
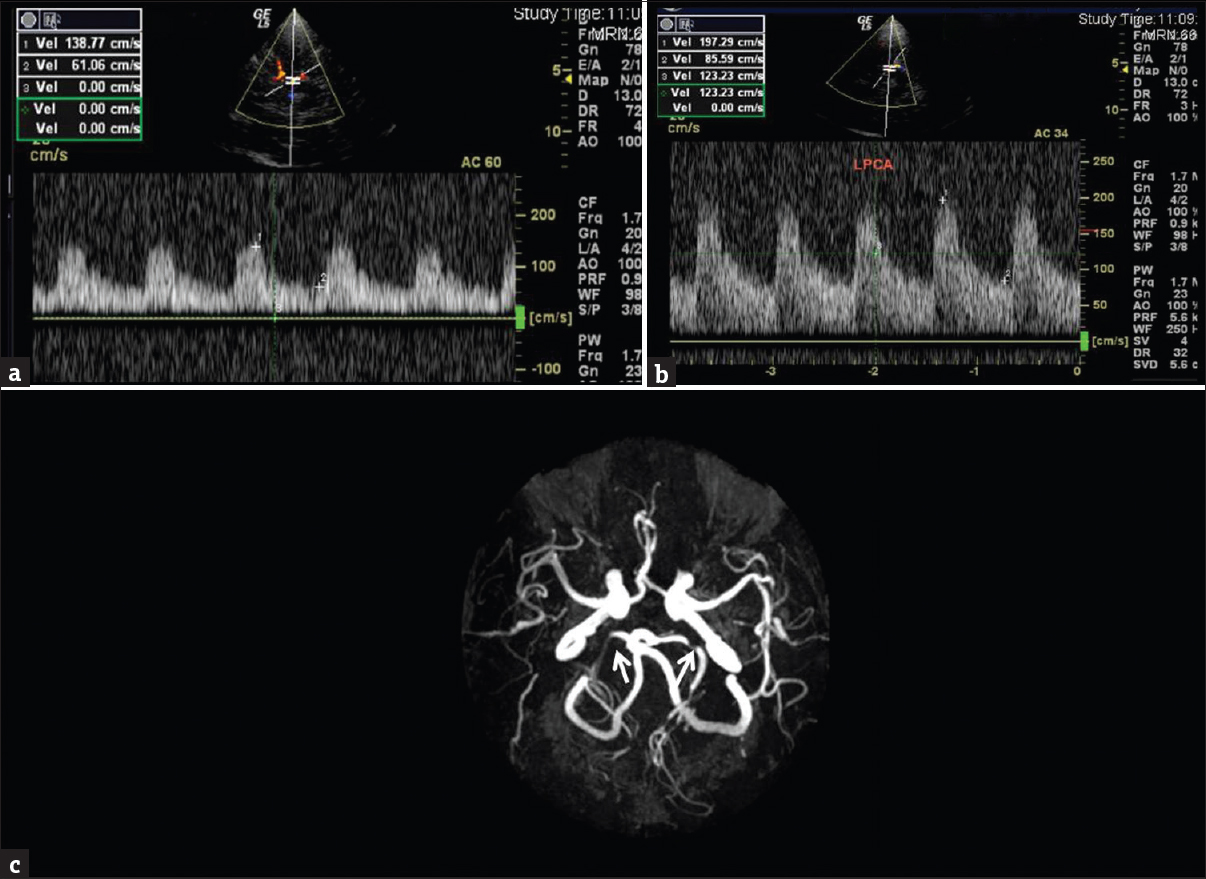
TCCS was performed on GE Logiq 500 Pro, GE Healthcare India, with 1.9–3 MHz sector array transducer. The bilateral terminal internal carotid artery (TICA) segments, middle cerebral artery (MCA-M1 and M2 branches), anterior cerebral artery (ACA), and posterior cerebral artery (PCA) were imaged through the transtemporal window with the patient in lying-down position [Figure 1], and the bilateral terminal VAs and proximal basilar artery (BA) were imaged through the transforaminal also called the transoccipital window with patients in either sitting or lying down, lateral position depending on the clinical condition of the patient [Figure 2]. The angle-corrected velocities were measured from the spectral display. Depending on the peak systolic velocity (PSV) recorded, Ralf W. Baumgartner criteria was used for stratifying ≥50%/< 50% stenosis in the various vascular segments as[19] ≥155/≥120 cm/s for ACA, ≥220/≥155 cm/s for MCA main stem (M1), ≥145/≥100 cm/s for PCA, ≥140/≥100 cm/s for BA, and ≥120/≥90 cm/s for VA, respectively.
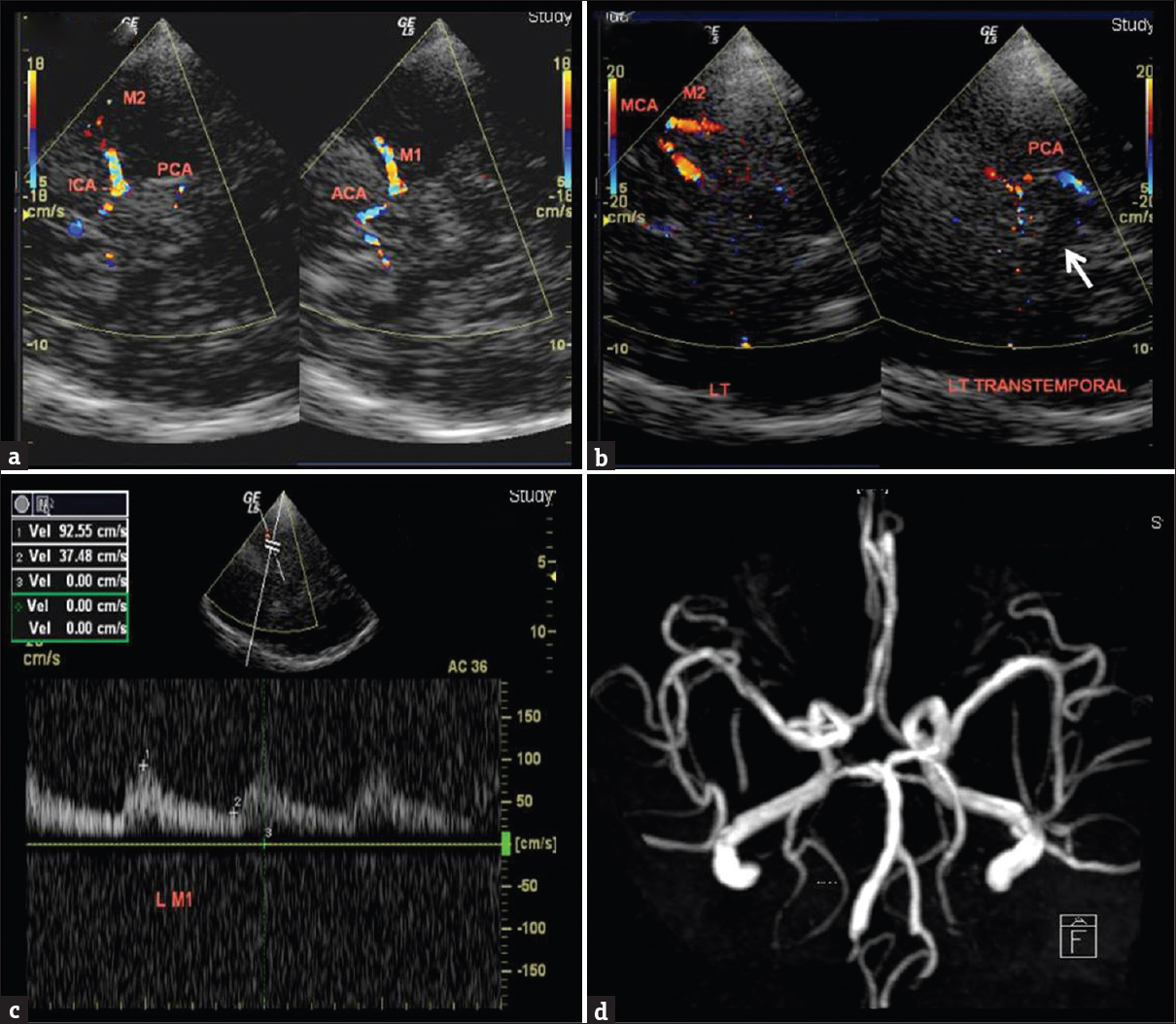
- (a) A 65-year-old male with dementia and past stroke. Transcranial color-coded Doppler sonography, right transtemporal insonation demonstrates ipsilateral (dotted lines), M1 and M2 segments of middle cerebral artery, anterior cerebral artery on color display. A 53-year-old female with a history of recurrent stroke. (b) Transcranial color-coded Doppler sonography, left transtemporal insonation shows the normal middle cerebral artery on color display. Posterior cerebral artery is curving around the hypoechoic mesencephalon (white arrow). (c) Left middle cerebral artery spectral waveform shows normal peak systolic velocity and spectrum. (d) Magnetic resonance angiogram showing a normal circle of Willis.
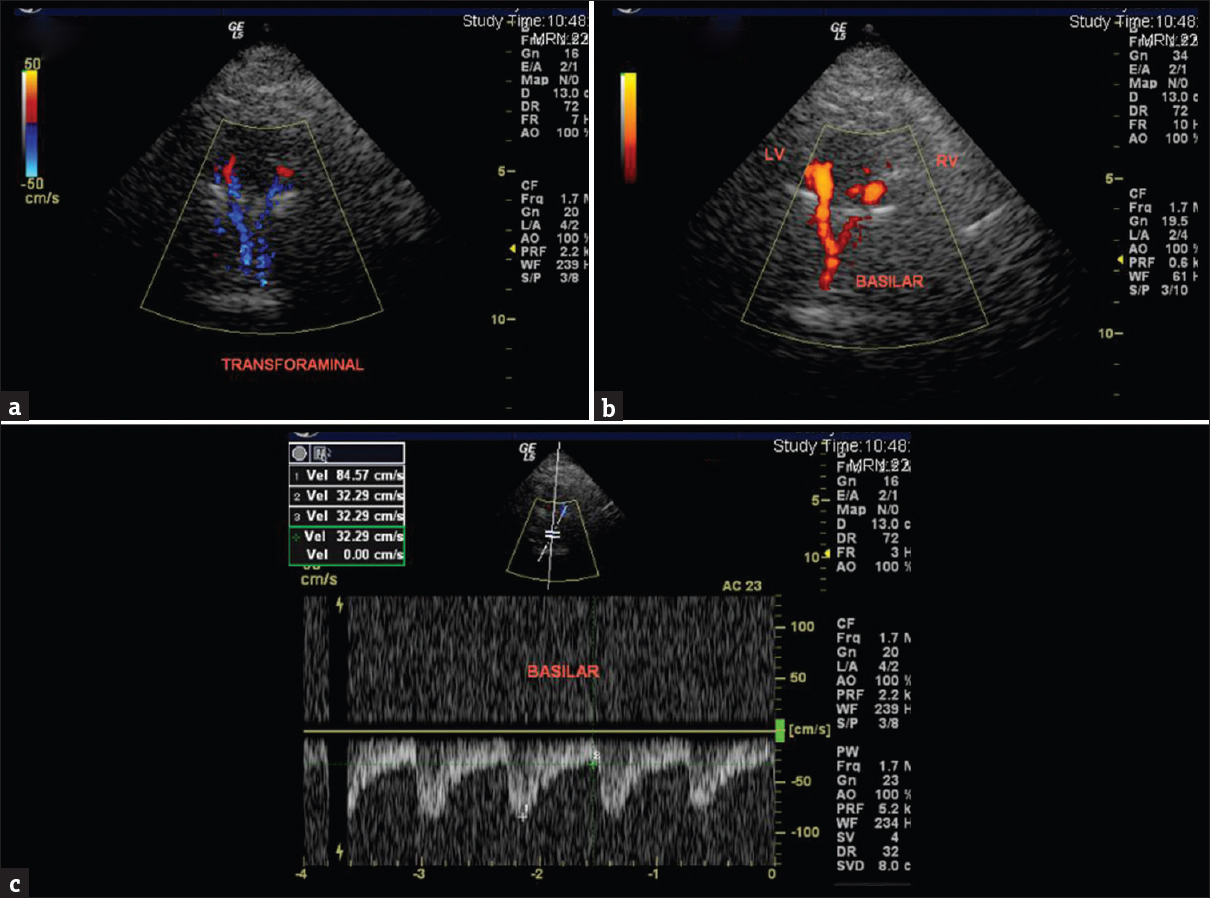
- A 47-year-old female with a history of left hemisensory syndrome. (a) Transcranial color-coded Doppler sonography, trans foraminal insonation through nape of the neck color Doppler and (b) power Doppler demonstration of the normal vertebral arteries (marked left vertebral and right vertebral) and proximal basilar artery. (c) Spectral waveform in proximal basilar artery shows normal peak systolic velocity and spectral pattern.
For intracranial TICA, elevation in PSV >120 cm/s was taken as the cutoff.[20] Ratio with contralateral TICA or MCA of at least 2:1 also was taken as additional criteria for classification into ≥50% stenosis.[21] Since there were no previous data available on velocity cutoffs for M2 stenosis, a value of ≥150/≥120 cm/s was taken in our study to classify as ≥50%/<50% stenosis in addition to the disturbed spectral flow pattern. Velocity in a single M2 branch which was well visualized was measured.
Unenhanced three-dimensional time of flight (TOF) MRA of the intracranial arteries was performed on 1.5 Tesla Magnetom Avanto, Siemens machine, and 3 Tesla Intera Achieva, Philips machines. The parameters used were repetition time (TR)/echo time (TE) (in milliseconds) of 24/8.6; 20° flip angle; 320 × 224 matrix; 0.6 mm section thickness with 0.12 mm slice gap on Siemens and TR/TE (in ms) of 25/3.4; 20° flip angle; 544 × 274 matrix; 1.4 mm section thickness with 0.7 mm slice gap for Philips machine, respectively.
The TCCS was performed by two observers in conjunction, and the observers included a radiology resident and a consultant neuroradiologist with >5 years of experience. The neck Doppler images recorded on picture archiving and communication systems (PACS) were first reviewed by the same observers followed by performance of TCCS. MRA images on the PACS were evaluated on a later day by the same observers. The stenosis grading was done by measurement of vessel caliber on the MRA source images.
Weighted kappa was computed to assess the agreement between TCCS and MRA. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of color Doppler with respect to MRA was calculated. Statistical analysis was done using Statistical Package for Social Sciences (SPSS) software (version 16, SPSS, Inc, Chicago, IL, USA).
The study was approved by the institutional review board.
RESULTS
Ninety patients satisfied the eligibility criteria for the study. The study group comprised of 78 males and 12 females. Majority (43.3%) of patients were in the age group of 50–60 years. The mean (standard deviation) age was 54.3 (9.9) years. The median time of the latest stroke episode in the patient from presentation was 3 months (range: <1–80 months).
Atherosclerotic risk factor profile
The atherosclerotic risk factors noted in the study population are shown in Table 1.
In patients who were smokers, the median pack years of smoking was 22.4 years (range: 1.8–156). Among patients who had intracranial atherosclerosis, 50% had diabetes and 68.8% had hypertension. Of the total of 1170 vascular segments studied by MRA, 1077 (92%) were successfully insonated. Suboptimal unilateral or bilateral temporal acoustic window was encountered in 13 (12.1%) patients.
The predominant subtype (TOAST) was small-artery occlusion (41.1%), followed by large-artery atherosclerosis (LAA) (33.3%), and stroke due to undetermined cause was 25.6%. Associated leukoaraiosis was found in 44.4% of patients. Leukoaraiosis was more prevalent in lacunar stroke subtype (64.9%).
Topographic distribution of cerebrovascular atherosclerosis
Intracranial atherosclerosis was found to be the predominant site of cerebral atherosclerotic disease in our study population, with 32/90 (35.6%) patients having significant intracranial arterial lesions. Isolated extracranial atherosclerosis was found in only 2/90 (2.2%), while combined intracranial and extracranial disease was found in 11/90 (12.2%). No significant proximal arterial lesion was found in 45/90 (50%) patients.
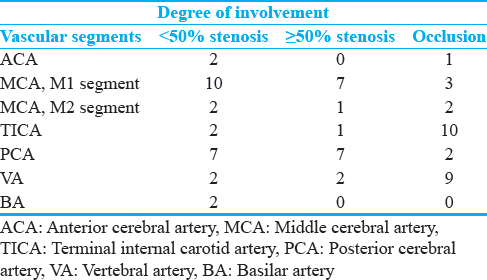
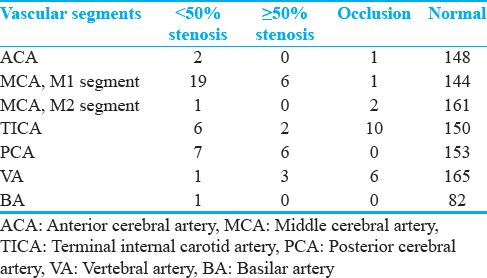
Distribution according to diseased vascular segments in intracranial circulation in our study population on MRA is shown in Table 2.
The distribution of diseased and normal vascular segments as evaluated on TCCS is shown in Table 3.
Comparison of transcranial color-coded Doppler sonography and magnetic resonance angiography
The weighted kappa values calculated to determine agreement between TCCS and MRA for assessment of various vascular segments in the intracranial circulation were 0.83 (good agreement between the two modalities) for ACA, 0.66 (fair agreement) for MCA, M1 segment, 0.45 (poor agreement) for MCA, M2 segment, 0.86 (good agreement) for TICA segment, 0.46 (poor agreement) for PCA segment, and 0.81 (good agreement) for VA segment.
The kappa value could not be computed for BA as there were not enough variables in the different disease categories to be compared.
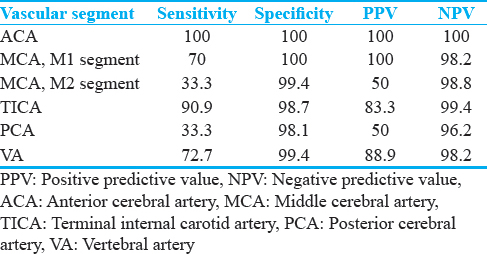
The sensitivity, specificity, PPV, and NPVs for hemodynamically significant (≥50%) and normal/hemodynamically insignificant lesions (0%–49%) in the different vascular segments on TCCS in comparison to MRA are shown in Table 4.
As there were no hemodynamically significant (>50%) arterial lesions in the BA in our sample population, the accuracy parameters could not be assessed .
DISCUSSION
Intracranial atherosclerosis was found to be the predominant site of cerebrovascular atherosclerosis in our study population. Previous studies have reported intracranial atherosclerosis to be responsible for majority of ischemic stroke in African-American and Asian patients.[6222324] Limited literature from India has also reported a predominance of intracranial disease. Kaul et al., from Hyderabad found a predominance of intracranial atherosclerosis (133/392, 33.9%) in their South Indian population studied.[25] This difference in the atherosclerotic disease spectrum in our population has crucial implications in clinical decision-making and management.
The classification of stroke into subtypes based on the etiology also has major implications in clinical practice. In our study, the most frequent subtype was the small-artery occlusion (lacunar stroke) category (41.1%), followed by LAA (33.3%). This is different from the study by Kaul et al., in which LAA was found to be the predominant subtype of stroke.[25]
Comparison of transcranial color-coded Doppler sonography with magnetic resonance angiography
The rate of suboptimal temporal window encountered in the present study was 12.14%. The reported rate of poor temporal window in TCCS is up to 20%.[26] This is higher than transcranial Doppler (TCD) because B-mode imaging in TCCS lacks the penetration of conventional TCD. The challenge of poor sonological window is partly overcome by the use of ultrasound contrast agents in some centers. A recent study done using TCD by Kamal et al., in South Asian population reported an insonation failure rate of 19.6% in males and 35.7% in females.[27]
Anterior cerebral artery
In our experience, ACA is technically difficult to be insonated because of its orientation during TCCS. The angle correction applied is often incorrect, resulting in spuriously increased velocities. We had only three patients with abnormalities in ACA on MRA, including one occlusion. Hence, the high sensitivity obtained in our study needs to be prospectively evaluated in a larger group with diseased ACA.
Middle cerebral artery, M1 segment
Out of the seven MRAs detected >50% stenoses, TCCS correctly identified six of them. One of these missed on Doppler was a stenosis located in the distal most M1 and sampling was done in the proximal M1 resulting in spurious normal velocity. This reinforces the importance of sampling the entire length of the vessel to avoid false negatives. Two out of three M1 occlusions were missed on TCCS. One of these patients had a severe stenosis in the ipsilateral TICA and multiple collaterals in the region of MCA. Probably one of the larger collaterals was imaged. Some studies have used USG microbubble contrast agents to improve the accuracy of detecting occlusions; however, we do not have experience with the same. A tandem lesion downstream a major stenosis cannot be detected on Doppler, and other modalities definitely score over Doppler in this setting.
Lien and Chen and Chen also have reported similar results for the detection of both MCA stenosis and occlusion.[2829]
Middle cerebral artery, M2 segment
TCCS had a very low sensitivity for distal MCA branches. Since TCCS lacks the penetration of conventional TCD, only the central vessels are better identified. There is also an inconsistency in the bifurcation or trifurcation of the MCA into M2. It is difficult to determine how many MCA branches are present and image each of them. We only imaged any one of the well-visualized M2 branches in our study.
Terminal internal carotid artery
There were good agreement and high sensitivity and specificity for the assessment of TICA segment on TCCS compared to MRA [Figure 3]. Navarro et al., who evaluated the accuracy of TCD in diagnosis of stenosis or occlusion of TICA, observed that the sensitivity was 90% and specificity was 83%.[21]
- A 37-year-old male with a history of progressive vision loss on the right (a) transcranial color-coded Doppler sonography, right transtemporal insonation shows absence of color flow in the right terminal internal carotid artery (dotted lines) suggestive of occlusion. (b) Transcranial color-coded Doppler sonography, left and right transtemporal insonation showing normal left anterior cerebral artery in blue (dotted lines on the left) and red-coded right anterior cerebral artery (dotted lines on the right) suggesting reversed flow toward the probe. (c) Spectral Doppler of right anterior cerebral artery shows waveform above the baseline in keeping with collateralization. (d) Magnetic resonance angiogram shows right internal carotid artery occlusion and reformed middle cerebral artery through collaterals.
Posterior cerebral artery
TCCS missed two out of seven >50% stenosis in PCA and the two PCA occlusions. The velocities were mostly measured in the P1 segment of the PCA in our study [Figure 4]. Most of the MRA-detected abnormalities were located in the distal P1 or P1–P2 junction. The anatomic orientation of PCA is such that it takes a curved course around the mesencephalon and angle correction is technically difficult in distal PCA, especially at the P1–P2 junction. Another fact to be aware of regarding false-negative finding in PCA is that SCA also courses very close to PCA and hence there could be sampling errors.
- A 61-year-old male with a history of residual left spastic hemiparesis after a previous episode of stroke. (a) Transcranial color-coded Doppler sonography, transtemporal insonation with spectral display from right posterior cerebral artery and (b) left posterior cerebral artery showing increased peak systolic velocity, left more than right. (c) Magnetic resonance angiogram showing significant stenosis of bilateral posterior cerebral artery (white arrows).
Vertebral artery
There was good agreement between MRA and TCCS in evaluation of terminal VA. One of the MRA-detected occlusions was classified as >50% stenosis on TCCS. This case illustrates the fact that TCCS provides real-time hemodynamic information unlike TOF MRA, which is known to overestimate stenosis. Furthermore, TOF technique is not sensitive to slow flow states. TCCS may aid in differentiating a complete occlusion from severe stenosis which is sometimes a dilemma on MRA.
Although the demonstration of intracranial vascular anatomy with TCCS is inferior to MRA, especially in the peripheral intracranial circulation, TCCS can provide reliable estimations of blood flow direction and velocity in the proximal basal cerebral vessels. The hemodynamic changes of an arterial lesion are demonstrated by Doppler, whereas TOF MRA provides only the anatomical details. TCCS could be advantageous in patients who require repeated imaging. A major role of TCCS may be in follow-up of patients with intracranial disease to assess the progress of disease. Furthermore, TCCS can be used at the bedside.
TCCS is highly operator dependent. Considerable experience is required for the radiologist to accurately and consistently identify the anatomic planes and vasculature. Adequate knowledge of cerebral hemodynamics is a must for interpretation of TCCS findings.
Limitations
Although digital subtraction angiography (DSA) is the gold standard, we used MRA as the reference standard as its performance is reported to be comparable to DSA[30] and considering the risks and cost factors associated with subjecting these patients to DSA. The low prevalence of vascular lesions in our study population could be explained by the fact that most of these patients were imaged in the chronic stage of stroke when recanalization of the vessel could have occurred. We did not use an ultrasound contrast agent which could have improved a poor sonological window to a certain extent.
CONCLUSION
Atherosclerotic occlusive lesions of the intracranial vessels are more common than extracranial atherosclerosis in patients from the Indian subcontinent.
Sensitivity of TCCS in detecting significant intracranial atherosclerosis varies in different vascular segments of intracranial circulation. A larger prospective study assessing the interobserver agreement may be helpful in evaluating the utility of this modality as a screening tool in developing nations like India, which has predominance of intracranial atherosclerosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank Mr. Saravanan and Mr. Solomon from the Department of Biostatistics, Christian Medical College, Vellore for their assistance with the statistical analysis.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2018/8/1/19/230767
REFERENCES
- Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095-128.
- [Google Scholar]
- Heart disease and stroke statistics – 2011 update: A report from the American Heart Association. Circulation. 2011;123:e18-209.
- [Google Scholar]
- Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction. The Northern Manhattan Stroke Study. Stroke. 1995;26:14-20.
- [Google Scholar]
- Race and sex differences in the distribution of cerebral atherosclerosis. Stroke. 1996;27:1974-80.
- [Google Scholar]
- Arteriographic study of sites, incidence, and treatment of arteriosclerotic cerebrovascular lesions. Neurology. 1962;12:698-711.
- [Google Scholar]
- Joint study of extracranial arterial occlusion VI Racial differences in hospitalized patients with ischemic stroke. JAMA. 1972;222:285-9.
- [Google Scholar]
- Cerebral atherosclerosis in Negroes and Caucasians. Atherosclerosis. 1972;16:141-54.
- [Google Scholar]
- Cerebrovascular disease among patients from the Indian subcontinent. Neurology. 2006;67:894-6.
- [Google Scholar]
- Secondary prevention of Stroke: The Evidence Based Review of Stroke Rehabilitation. Available from: http://www.ebrsr.com
- [Google Scholar]
- Progression and clinical recurrence of symptomatic middle cerebral artery stenosis: A long-term follow-up transcranial Doppler ultrasound study. Stroke. 2001;32:2898-904.
- [Google Scholar]
- The warfarin-aspirin symptomatic intracranial disease study. Neurology. 1995;45:1488-93.
- [Google Scholar]
- Transcranial color-coded sonography for the detection of middle cerebral artery stenosis. J Ultrasound Med. 2005;24:451-7.
- [Google Scholar]
- Transcranial color duplex sonography in cerebrovascular disease: A systematic review. Cerebrovasc Dis. 2003;16:4-13.
- [Google Scholar]
- Can we apply the national cholesterol education program adult treatment panel definition of the metabolic syndrome to Asians. Diabetes Care. 2004;27:1182-6.
- [Google Scholar]
- Body mass index, waist circumference, and waist-hip ratio on the risk of total and type-specific stroke. Arch Intern Med. 2007;167:1420-7.
- [Google Scholar]
- Association between plasma homocysteine concentrations and extracranial carotid-artery stenosis. N Engl J Med. 1995;332:286-91.
- [Google Scholar]
- Classification of subtype of acute ischemic stroke Definitions for use in a multicenter clinical trial TOAST Trial of org 10172 in acute stroke treatment. Stroke. 1993;24:35-41.
- [Google Scholar]
- Carotid artery stenosis: Gray-scale and Doppler US diagnosis – Society of radiologists in ultrasound consensus conference. Radiology. 2003;229:340-6.
- [Google Scholar]
- Assessment of >50% and <50% intracranial stenoses by transcranial color-coded duplex sonography. Stroke. 1999;30:87-92.
- [Google Scholar]
- Use of transcranial Doppler ultrasound to predict outcome in patients with intracranial large-artery occlusive disease. Stroke. 2000;31:2641-7.
- [Google Scholar]
- The accuracy of transcranial Doppler in the diagnosis of stenosis or occlusion of the terminal internal carotid artery. J Neuroimaging. 2004;14:314-8.
- [Google Scholar]
- Racial differences in the distribution of posterior circulation occlusive disease. Stroke. 1985;16:785-90.
- [Google Scholar]
- Duplex Doppler and spectral flow analysis of racial differences in cerebrovascular atherosclerosis. Stroke. 1990;21:740-4.
- [Google Scholar]
- Chinese-white differences in the distribution of occlusive cerebrovascular disease. Neurology. 1990;40:1541-5.
- [Google Scholar]
- Subtypes of ischemic stroke in a metropolitan city of South India one year data from a hospital based stroke registry. Neurology India. 2002;50(Suppl 1):S8-S14.
- [Google Scholar]
- The basic transcranial Doppler examination: Technique and anatomy. In: Babikian V, Wechler L, eds. Transcranial Doppler Ultrasonography (2nd ed). Boston: Butterworth Heinemann; 1999. p. :13-31.
- [Google Scholar]
- Diagnostic TCD for intracranial stenosis in acute stroke patients: Experience from a tertiary care stroke center in Karachi, Pakistan. BMC Res Notes. 2015;8:341.
- [Google Scholar]
- Comparison of transcranial colour-coded sonography and magnetic resonance angiography in acute ischemic stroke. J Neuroimaging. 2001;11:363-8.
- [Google Scholar]
- Absent middle cerebral artery signal in transcranial colour-coded sonography: A reliable indicator of occlusion. Cerebrovasc Dis 2005. 2005;251:7.
- [Google Scholar]
- Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: A systematic review. Stroke. 2003;34:1324-32.
- [Google Scholar]




