
Translate this page into:
Musculoskeletal Disorders in the Elderly
Address for correspondence: Dr. Ramon Gheno, Centre de Consultations et d’Imagerie de l’Appareil Locomoteur, 2 Avenue Oscar-Lambret, 59037 Lille Cedex, France. E-mail: rgheno@yahoo.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Musculoskeletal disorders are among the most common problems affecting the elderly. The resulting loss of mobility and physical independence can be particularly devastating in this population. The aim of this article is to present some of the most frequent musculoskeletal disorders of the elderly, such as fractures, osteoporosis, osteoarthritis, microcrystal disorders, infections, and tumors.
Keywords
Aged
arthritis
fracture
musculoskeletal diseases
neoplasm

INTRODUCTION
Musculoskeletal disorders are common problems affecting the elderly.[1] With age, musculoskeletal tissues show increased bone fragility, loss of cartilage resilience, reduced ligament elasticity, loss of muscular strength, and fat redistribution decreasing the ability of the tissues to carry out their normal functions.[2] The loss of mobility and physical independence resulting from arthropathies and fractures can be particularly devastating in this population, not just physically and psychologically, but also in terms of increased mortality rates.[3] The aim of this article is to present some of the most frequent musculoskeletal disorders of the elderly, including some misleading presentations.
Search criteria
The Medline database was used to search for the articles. We used the following terms and some of its combinations: Elderly, aged, epidemiology, fracture, osteoporosis, vertebral, hip, pelvis, arthritis, neoplasm, malignancy, myeloma, paget, gout, infection, microcrystal, and radiology. Articles without English abstracts were excluded. Besides, certain relevant rheumatological, orthopedic, and radiological books were also used. The current review is based on information obtained from 55 articles and eight books.
Fractures
Fractures are frequent in the elderly and result mainly from the effects of falls and osteoporosis.[34] Low-impact falls, even from standing height, are the most common cause of injury in geriatric patients.[3] Falling is a multi-factorial problem due to both extrinsic (e.g., environmental and housing conditions) and intrinsic risk factors (e.g., impaired mobility, loss of muscular strength, poor visual acuity, and medication, for instance corticoids).[4–6] Osteoporosis, which is characterized by qualitatively normal, but quantitatively deficient bone, leads to bone fragility and increased risk of fractures.[37] The general prevalence of osteoporosis in women is approximately 50% at the age of 85 years, while in men the prevalence is about 20% at that age.[8] Ethnic differences also exist: Mineral bone density is higher in black women and lower in Asian women, while in white women evidence shows an intermediate value.[9] Due to its precision, the most widely used quantitative technique is dual energy X-ray absorptiometry, which makes it possible to diagnose osteoporosis early, predict the risk of fracture, determine therapeutic intervention, and monitor response to treatment.[4710] This method grades bone loss according to standard deviations (SD) from the mean young adult value. A value less than 2.5 times the SD below the young adult mean, is considered to indicate osteoporosis.[411] The main radiographic features of osteoporosis are increased radiolucency and cortical thinning, mainly in the spine, giving rise to a well-demarcated outline of the vertebral body, which has been described as, ‘picture framing’.[12] Besides, in the spine, an increased biconcavity of the vertebral end plates, with a protrusion of the intervertebral disk into the vertebral body can be observed.[12] However, early radiographic changes are subtle, as a bone loss of approximately 30% must occur before it can be detected.[7]
Vertebral compression fractures are the most common osteoporotic fractures, with a greater incidence in women over 60 years of age.[1314] They can be observed in up to 25% of women over 70 years of age and 40% of those over 80 years.[3] After one episode, the risk of subsequent vertebral fracture increases at least four-fold, with substantially increased rates during the first year.[1415] These fractures are associated with higher mortality and significant morbidity, even though they are afforded little clinical attention.[1617] They often appear as multiple fractures with anterior wedging, and may be associated with significant deformity, leading to kyphosis. They are usually well demonstrated on radiographs, but can be better assessed with computed tomography (CT) or magnetic resonance (MR) imaging, when necessary. The latter imaging modality may be indicated in case of associated neurological symptoms – a rare event – or when a vertebroplasty is discussed, in order to better localize the recently fractured vertebra. Vertebral compression fractures in the elderly may involve several problems: First is differentiating between osteoporotic and malignant vertebral collapse (VC), particularly metastatic VC, as the latter is by far the most common malignant tumor affecting the skeleton in the elderly.[18] In most patients, plain films allow this differentiation. Multiple, relatively symmetrical thoracolumbar VCs, associated with diffuse increased radiolucency are suggestive of osteoporosis [Figure 1a]. The whole vertebral endplate is impacted, sometimes in association with increased or decreased radiolucency of the subjacent trabecular bone (band-like distribution of the abnormalities under the fractured vertebral end plate). Gas can also be seen under the fracture and is nearly pathognomonic of the benign nature of the collapse. There is no cortical osteolysis, although fractures can be identified with retropulsion of a bone fragment. Conversely, the following are a cause for concern: a single VC, involvement of the cervical spine, heterogeneous increased or decreased radiolucency that cannot be explained by an underlying end plate fracture, a focal collapse (on the AP or lateral view), or a bulging of the vertebral body or cortical osteolysis [Figure 1b]. If in doubt or for a better assessment of the spinal canal and soft tissue, CT, or better yet, an MRI can be performed, in order to differentiate between these two disorders. In benign fractures, an MRI may show a band distribution of abnormal signal intensities on T1 and T2 weighted images, spared normal bone marrow signal intensity, retropulsion of a posterior bone fragment, and multiple compression fractures; on the contrary, signs such as a convex posterior border of the vertebral body, abnormal signal intensity of the posterior elements, an epidural mass or a focal paraspinal mass are suggestive of spinal metastasis.[19–21] Second, vertebral fractures can be missed following moderate trauma, because the fracture may be difficult to identify in an osteoporotic radiolucent bone and / or because the pain is attributed to another painful condition, such as degenerative changes. This is observed in particular in the cervical spine, particularly at C2, and may lead to secondary neurological complications [Figure 2]. Finally, transverse fractures should enter in the differential diagnosis in an ankylosed spine. Ankylosis may be related to ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, which especially affect males and they have an estimated frequency of 5 to 15% in the elderly.[22–25] These ankylosed spines become increasingly susceptible to injury, even in the event of low-energy impacts, and are prone to unstable vertebral fractures with an increased frequency of neurological complications, either primary or secondary, after unprotected transfers and manipulation.[24] These lesions may be missed on plain films when non-displaced or mildly displaced, especially in hyperextension, whereas, they are well demonstrated on CT or MR imaging.[24] However, the MRI features can sometimes be misleading and mimic infectious spondylitis when signal abnormalities of the disco-vertebral junction are present. Caution is required when an elderly patient presents with an ankylosed spine, minor trauma or acute pain, especially if signal abnormalities of the anterior and posterior spine are observed [Figure 3].
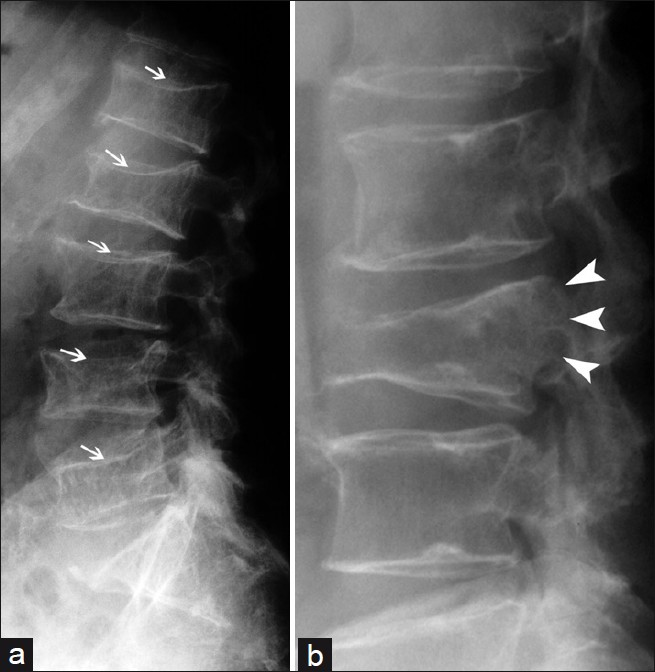
- Usual benign vertebral compression (a) multiple levels, diffuse radiolucency, and whole vertebral endplate involvement (arrows); usual malignant vertebral compression characteristics (b) single vertebral involvement, focal and bulging of the posterior wall (arrowheads).

- Missed fracture of the odontoid process and vertebral body of C2 (arrows) in a patient with a history of fall one month before. Note the associated degenerative changes of the lower cervical spine (arrowheads).
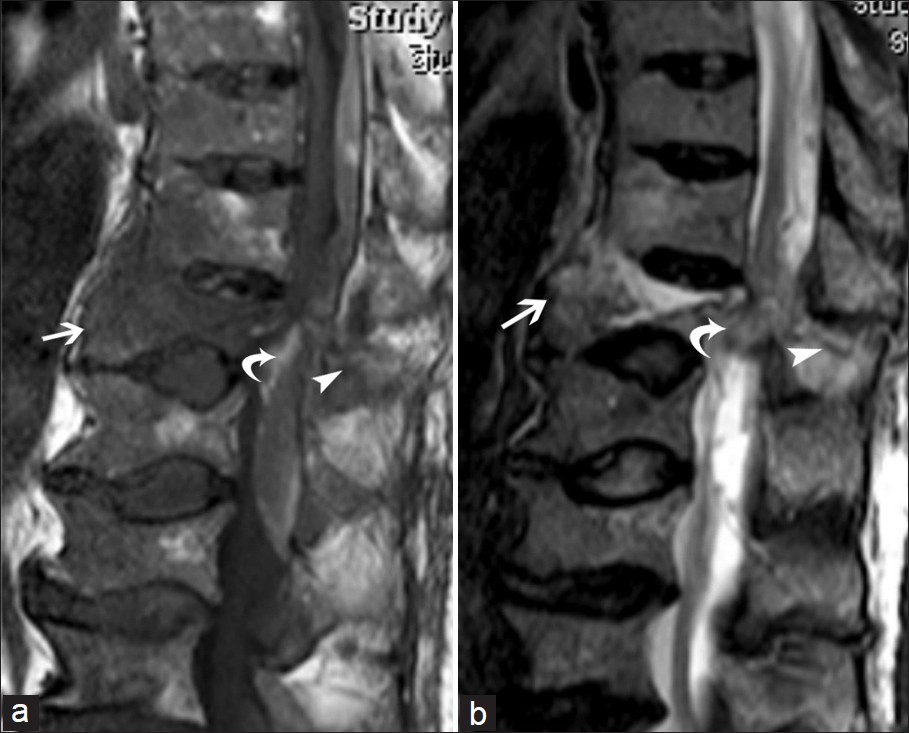
- Transverse fracture of thoracic vertebral body (arrow) and posterior arch (arrowhead) with posterior epidural hematoma (curved arrow) in an ankylosed spine depicted on (a) T1- and (b) T2-weighted sequences.
Other important sites of fractures are the hip and the pelvis, which are associated with increased mortality and specific diagnostic problems in the elderly population.[26] They are common and frequently result from lateral falls directly on the greater trochanter, in the case of hip fractures, and forward or backward falls in the case of pelvic fractures.[327] Most fractures are easily diagnosed by conventional radiography, particularly fractures of the proximal femur. However, non-displaced fractures may be negative or equivocal, particularly if the bone is osteoporotic. If a clinical suspicion of a fracture persists, CT or better still MR imaging is advocated, as this modality can show the fracture line surrounded by bone marrow edema.[28] Spontaneous osteoporotic insufficiency fractures are also common and not necessarily associated with trauma. They may occur everywhere, but are particularly common in the hip and pelvis, the majority being located in the sacrum and pubic ramus [Figure 4].[2930] Radiographic findings are often subtle or unremarkable, and in suspected cases MR imaging is indicated due to its superior accuracy as compared to other radiological methods.[2931] All the images should be carefully analyzed, as multiple insufficiency fractures are frequent [Figure 5].[29] Subchondral fractures are particularly difficult to identify on radiographs, but the thin hypointense line that represents the fracture, surrounded by a variable degree of edema, is well demonstrated on an MRI [Figure 6]. This kind of fracture can be complicated by a necrosis of the subchondral bone, which is hypointense on T2 weighted images, and is not enhanced following gadolinium administration.
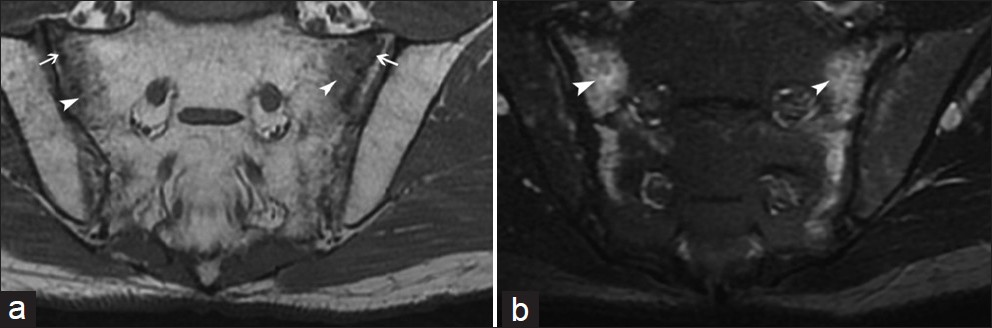
- Insufficiency fractures (arrows) located in the sacrum with adjacent edema (arrowheads), better depicted on (a) T1- and (b) T2- weighted sequences, respectively. This bone edema should not be confused with sacroiliitis.
- Multiple fractures (white arrows) in (a) the proximal femur and (b) pubic ramus on coronal T1-weighted images
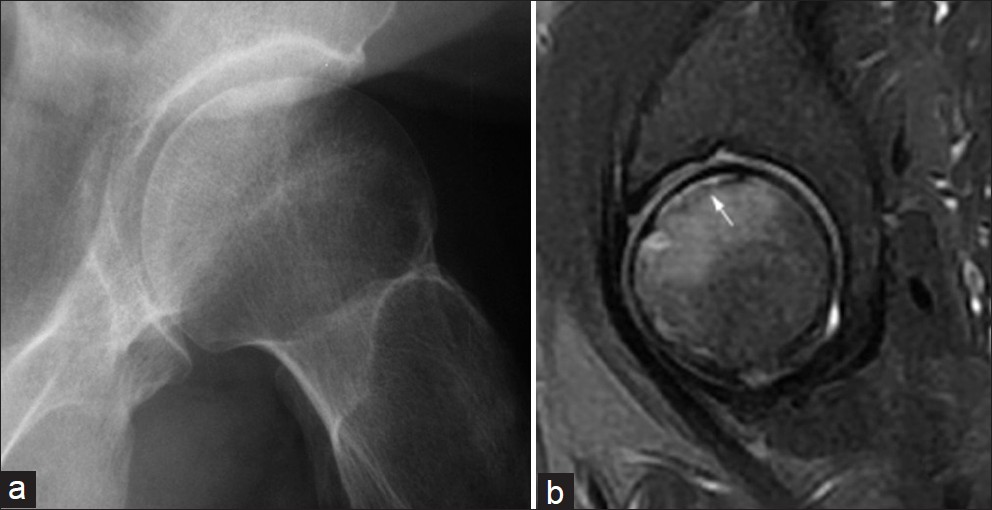
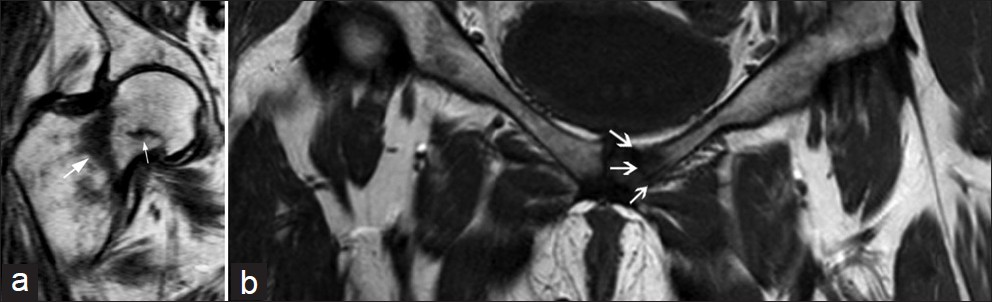
- Subchondral fracture of the femoral head: (a) conventional radiography and (b) fat saturated sagittal T2-weighted image (white arrow).
Osteoarthritis and associated conditions
Osteoarthritis (OA) can be defined as a group of distinct, but overlapping diseases, which may have different etiologies, but similar biological, morphological, and clinical outcomes – affecting the articular cartilage, subchondral bone, ligaments, joint capsule, synovial membrane, and periarticular muscles.[32] Pathological changes can include fibrillation of cartilage, disruption of collagen fibers, changes in proteoglycan staining, chondrocyte proliferation, necrosis, and neovascularization.[32] OA is the most common joint disease in persons 65 years of age and above, with a radiographic prevalence as high as approximately 90% in women and 80% in men.[33–35] Its etiology is not fully understood, although there are several related factors, such as female gender, genetics, metabolism, and excessive mechanical stress.[3234] It frequently leads to decreased function and loss of independence. Although the joints of the hand are the most commonly affected, they are less likely to be symptomatic than the knee or hip [Figure 7].[3436] The diagnosis of OA is primarily based on clinical history and physical examination. Plain radiographs can help confirm both the diagnosis and grade the severity of the condition. The cardinal radiographic features of OA are focal / non-uniform narrowing of the joint space in the areas subjected to the most pressure, subchondral cysts, subchondral sclerosis, and osteophytes.[37] However, the severity of the spondylolisthesis of the radiographic changes does not correlate with the clinical symptoms. Shoulder OA and rotator cuff disease are also fairly common in the elderly and are associated with significant shoulder pain and disability related to decreased shoulder movement. Direct signs of OA and indirect signs of large rotator cuff tears can be seen on plain films, including superior humeral head migration and remodeling of the acromion and the greater tuberosity.[38] Ultrasound is another valuable tool for easy assessment of the rotator cuff tendons due to its good sensitivity and specificity [Figure 8]. However, when surgical treatment is considered, arthro-CT, or MRI may be preferred, in order to improve its planning. The lumbar and cervical spine is also frequently affected, with degenerative changes of the disk spaces, facet joints, and spinous processes, and sometimes with progressive scoliosis. Although the intervertebral disks are not synovial joints, the pathological changes are similar to those seen in the articular cartilage.[32] CT and MRI are routinely used for the evaluation of narrowing of the central canal, lateral recesses, and neural foramina, when such an assessment is required (percutaneous or surgical treatment). Besides, MRI can be useful in evaluating marrow changes in the vertebral plate, especially inflammatory changes (Type I Modic), which present a positive correlation with low back pain.[39]
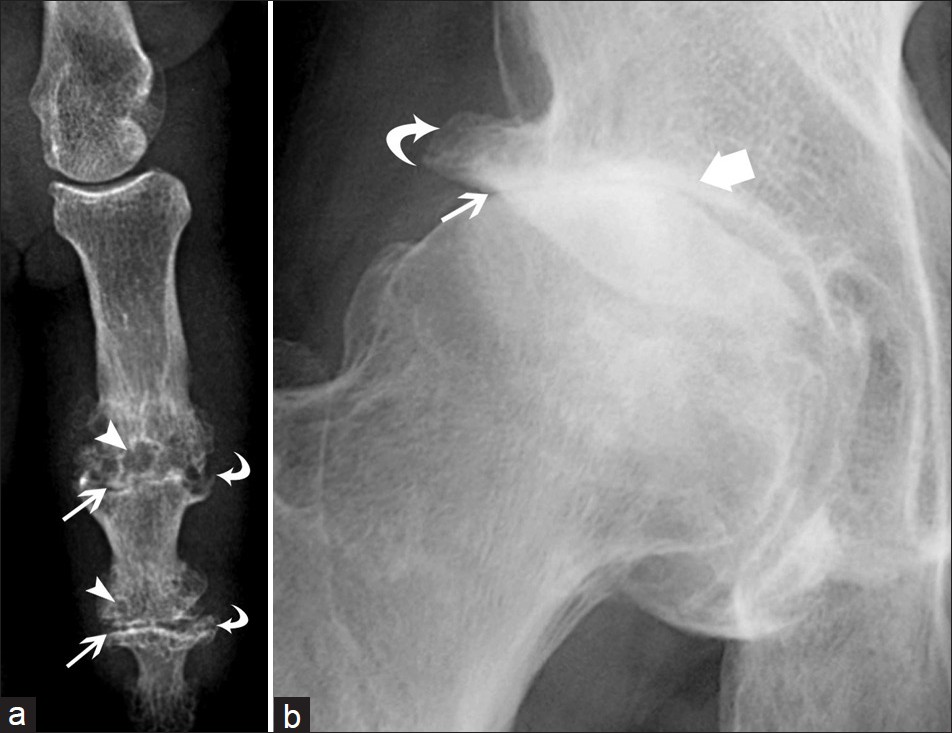
- Typical osteoarthritis of (a) the distal and proximal interphalangeal joints and (b) hip joint: joint space narrowing (arrows), subchondral cysts (arrowheads), osteophytes (curved arrows), and subchondral sclerosis (thick arrow).
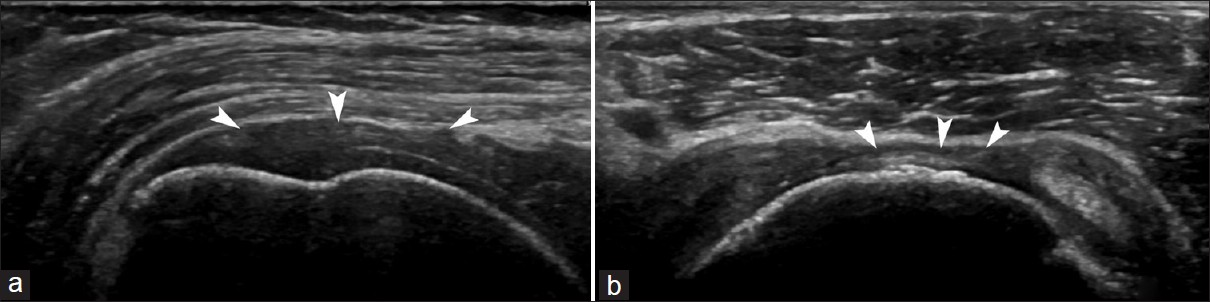
- Ultrasound images in (a) the long and (b) short axis of the supraspinatus tendon demonstrating a complete tear (arrowheads).
Microcrystal disorders
The frequency of microcrystal disorders also increases with age; this is mainly true of gout and calcium pyrophosphate dihydrate deposition (CPDD) arthropathy. Gout is the most common inflammatory arthritis in the elderly and is characterized by a disturbance of purine metabolism, with deposits in the joints, cartilage, and kidneys.[4041] The first metatarsophalangeal joint is the most common site of involvement in gouty arthritis [Figure 9], but any joint can be involved.[3] The typical radiographic features include eccentric nodular soft tissue masses (particularly suggestive of tophus when they are dense), close erosions (also suggestive when located at a distance from the joint and when associated with an elevated bony margin), preservation of the joint space, exuberant bony proliferation, and lack of periarticular osteoporosis.[42] When the clinical, biological, and radiographic findings are uncertain, an ultrasound may be particularly helpful, as this technique may demonstrate more tophi [Figure 10] and erosions than plain films, more synovitis than a clinical examination, suggestive hyperechoic aggregates in the synovium or in the joint fluid, which may be aspirated, and the double contour sign (an irregular hyperechoic band over the superficial margin of the articular cartilage, related to crystal deposition).[42–44] Calcium pyrophosphate dihydrate deposition (CPDD) disease is characterized by articular and periarticular tissue deposits (hyaline cartilage, fibrocartilage, and other soft-tissue structures), even in the spine [Figure 11].[45] Unlike gout, in which the increase in serum urates leads to supersaturation and deposits in the joints, in CPDD, the calcium deposits usually appear in the cartilage in the absence of any serum abnormality.[33] Even though such deposits may be seen in asymptomatic patients, they may be associated with the development of severe arthropathies or with acute pain related to the migration of the crystals in the synovial fluid, mimicking septic arthritis.[334647]
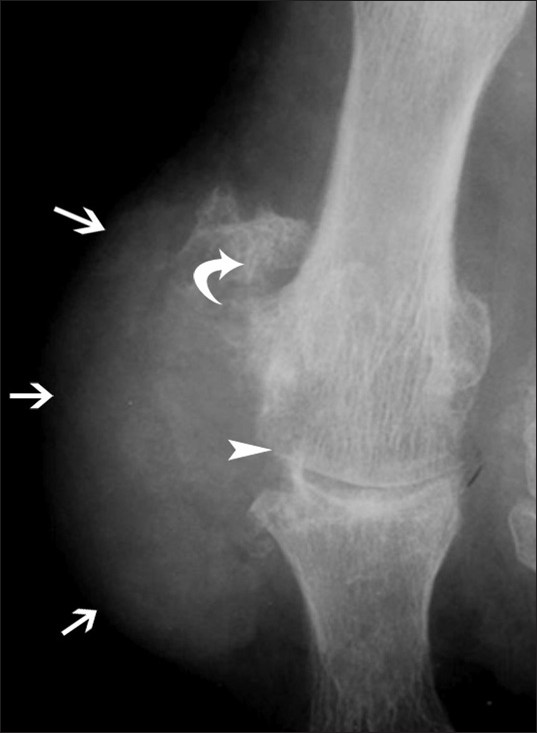
- Gout of the first MTP joint in conventional radiography: Excentric dense nodular soft tissue mass (arrows), large erosions (arrowhead), lack of periarticular osteoporosis, and exuberant bony proliferation (curved arrow).
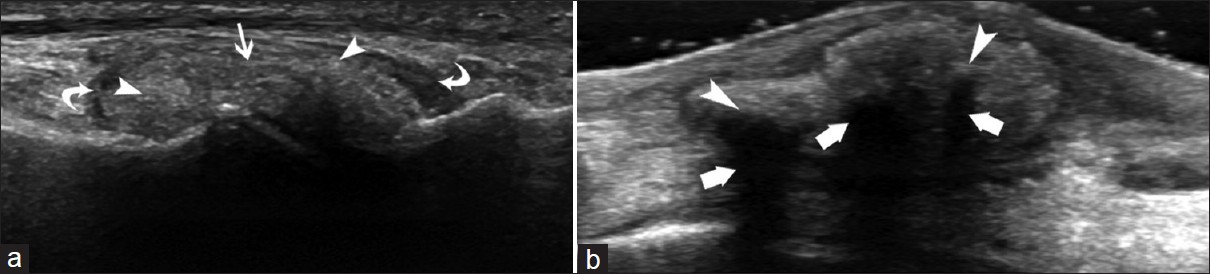
- Gout involvement of the MTP (a) shows the tophus (arrow) with hyperechogenic microcrystal deposits (arrowheads) and a thickened synovium (curved arrows). Another patient with tophus deposition in the dorsal midfoot (b) demonstrates microcrystal deposits (arrowhead) with acoustic shadows (thick arrows).
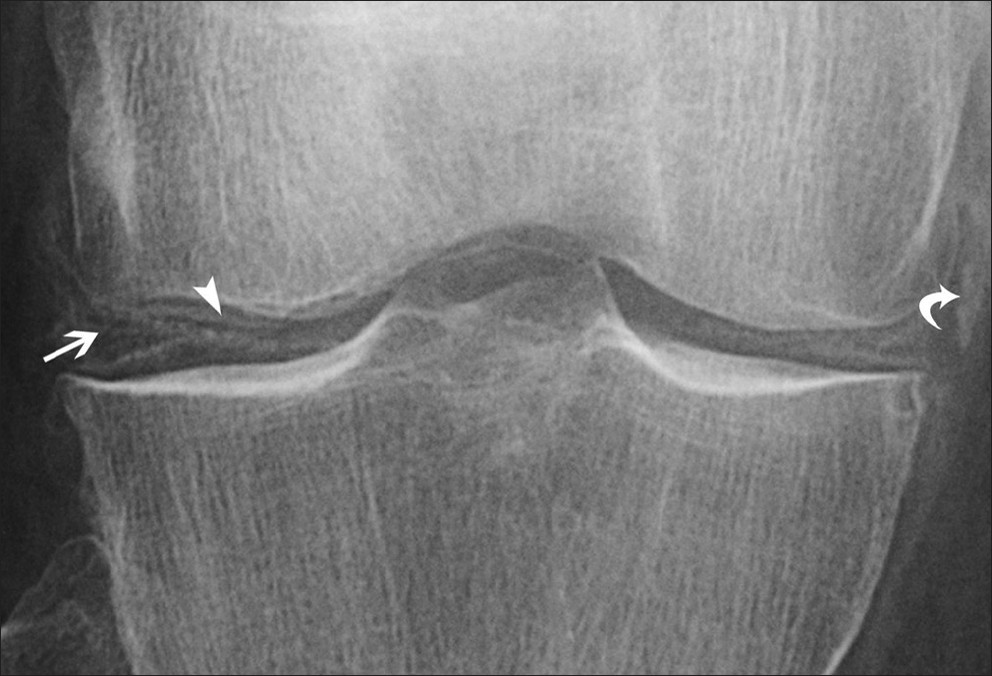
- Calcium pyrophosphate dihydrate deposition disease demonstrated by deposits of microcrystals in the menisci (arrow), articular cartilage (arrowhead), and periarticular soft tissue (curved arrow).
Infection
Elderly patients are more prone to infection because of an increased incidence of predisposing disorders (diabetes mellitus, peripheral vascular disease, poor dentition,…), immunosuppression and surgical procedures in this population (dental extractions, open heart surgery, prosthetic joint replacement,…).[348] The infectious agents affecting elderly patients are similar to those found in the younger population; although in the elderly, evidence shows an increased incidence of infection by nosocomial organisms (due to institutionalization and hospitalization). These infections can have a relatively benign course, as in the case of cellulitis, or serious consequences, as with necrotizing fasciitis.[4849] In patients over 80 years of age, the knee, shoulder, and hip are the most frequently affected joints. Another peculiarity of the elderly, uncommon in adults, is acute hematogenous osteomyelitis that mainly affects the spine.[49] Attention should, moreover, be paid to the diagnosis of tuberculosis, as early manifestations are subtle and advanced disease mimics other infections, granulomatous diseases, and malignancy.[50] Tuberculosis may affect the spine (about 50% of cases), with potential neurological consequences, or any joint, causing deformity [Figure 12]. It should be noted that elderly men may present with bone lesions, as a manifestation of reactivation of the disease.[50] As there are no pathognomonic imaging signs of musculoskeletal tuberculosis, the most conclusive means of reaching a diagnosis is by biopsy and culture, as chest radiographs and skin tests may not be positive in the elderly.[50] As regards imaging techniques, magnetic resonance imaging is the modality of choice for musculoskeletal infection, as it best delineates the extension of soft tissue infections.[48] Computed tomography, ultrasound, radiography, and nuclear medicine studies are considered to be ancillary.[48] In some circumstances ultrasound can be very useful, as it allows the aspiration of fluid collected in the joints or soft tissue, the evaluation of structures adjacent to orthopedic hardware, or the assessment of small peripheral joints.[485152] Besides, in the case of debilitated elderly patients, a mobile ultrasound device can be easily moved close to their beds.
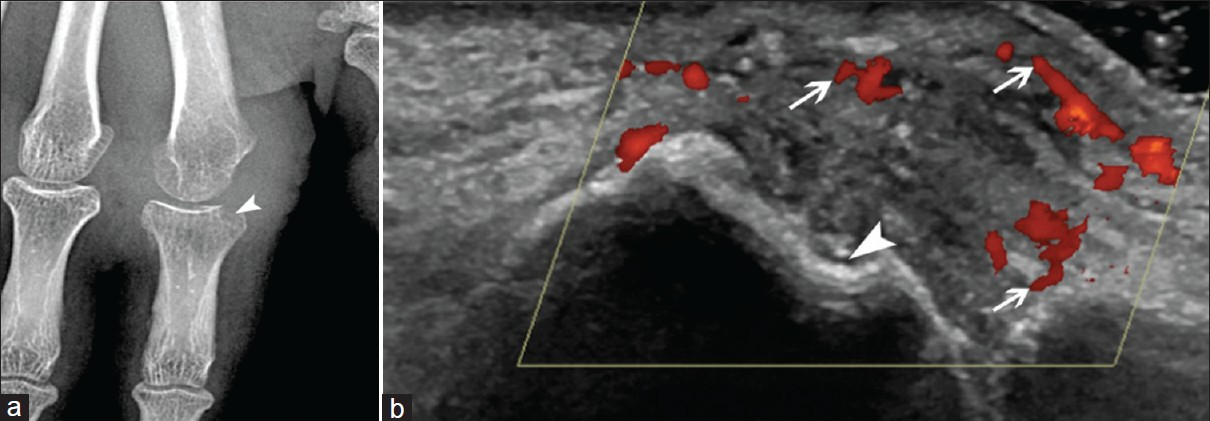
- Tuberculosis of the second metacarpophalangeal joint. (a) On conventional radiography there is mild osteoporosis, extensive soft tissue swelling, and large marginal erosion (arrowhead), (b) On Doppler ultrasound the synovitis (arrows) and bone erosion (arrowhead) are well-depicted.
Paget's disease
Paget's disease is a bone disorder characterized by an increase in osteoclast-mediated bone resorption accompanied by osteoblast-mediated formation of new bone of inferior quality.[3] The frequency of this condition is decreasing, but it still exists in 1 – 5% of persons over 50 years of age, varying according to geographic areas.[53–56] The radiographic signs include an advancing wedge of bone resorption, an accentuation and coarsening of the bone trabeculae along lines of stress, cortical thickening, and enlargement of the bone [Figure 13]. As a result, secondary osteoarthritis, insufficiency fractures, bowing of the bones, and even spinal cord or nerve root compression can be observed. In a minority of cases, sarcomatous degeneration may develop, mainly in the humerus, pelvis, and proximal femur, with a frequency believed to range from 0.9 to 2%.[5758]
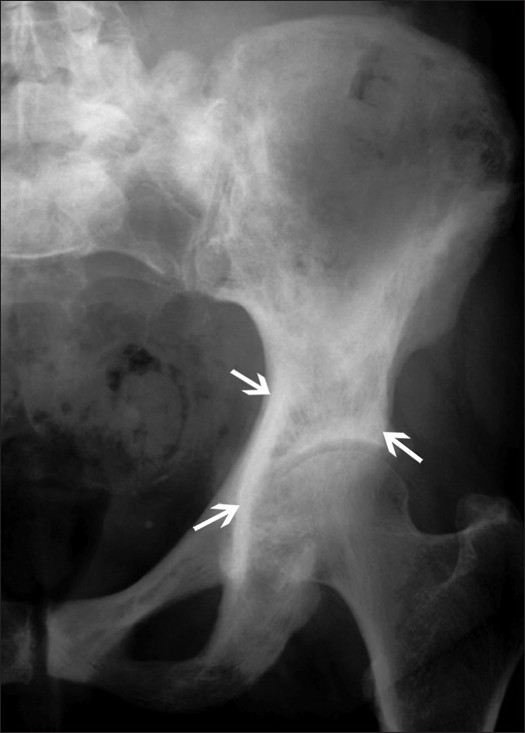
- Paget's disease affecting the iliac bone demonstrated with coarsening of the bone trabeculae and cortical thickening (arrows).
Tumors: Tumors can be revealed by bone pain, pathological fractures, or disability, or be discovered as an incidental finding. Primary bone tumors in elderly patients are not common, but, due to the risk of metastases, any newly discovered bone lesion or one developing within a known pre-existing lesion must be assumed to be malignant until proven otherwise.[3]
Metastases: Bone metastases are a common complication of malignant disease, especially of the breast, prostate, and lung.[1859] Although they are often multiple, a solitary metastasis is still more common than a primary neoplasm. Plain films are relatively insensitive for the detection of bone metastases, especially subtle lesions. MR imaging is superior to CT in the detection of malignant marrow infiltration, and it has a better contrast resolution for visualizing soft tissue and spinal cord lesions. Even with the advances in MRI, especially for bone marrow screening, bone scintigraphy continues to be used as an effective method for initial evaluation of the whole body for bone metastases.[59]
Sarcomas: In the elderly population, many sarcomas are secondary to a pre-existing disorder of the bone, such as Paget's disease, or lesions treated by radiation. Chondrosarcoma must also be kept in mind, especially when isolated osteolytic lesions of the pelvis are seen, as this is the most common primary sarcoma of bone in adults.[60] The cartilaginous nature of the lesion may be suggested by the presence of calcifications or by a lobulated hyperintense lesion in an MRI [Figure 14].
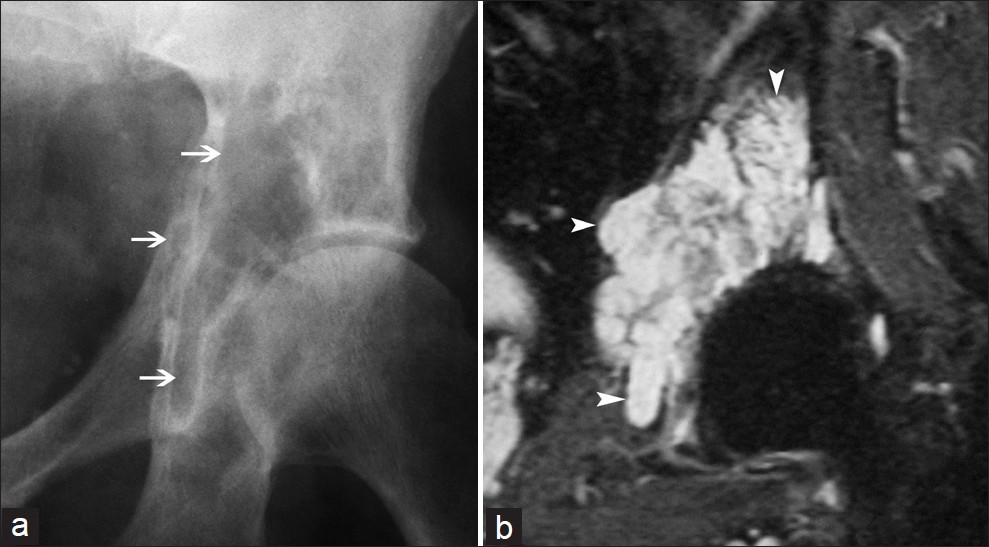
- Chondrosarcoma of the pelvis in (a) conventional radiography appears as an isolated osteolytic lesion (arrows), (b) Coronal T2-weighted image demonstrates a lobulated hyperintense lesion (arrowheads).
Myeloma: Myeloma is a characteristic disease in the elderly population, with a peak incidence in the eighth decade that results from an unregulated, progressive proliferation of neoplastic monoclonal plasma cells that accumulate in the bone marrow, leading to anemia and marrow failure.[6162] Osteolytic lesions may be present on plain films, but differentiating osteoporotic vertebral compression fractures from those associated with myeloma is a common diagnostic dilemma, as bone loss may be the first sign revealing the latter disease. Indeed, widespread osteoporosis, due to cytokine-mediated osteoclast activation, is common in patients with myeloma.[63] This possible association must be kept in mind, particularly if other features are present, including unexplained back or bone pain.[61]
CONCLUSION
Special attention is required in this population, as an early diagnosis can avoid delay in treatment, which is associated with increased morbidity and mortality. Besides, a better understanding of musculoskeletal diseases can lead to the implementation of effective preventive measures, thus reducing public health expenditure, and improving the quality of life in the elderly.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/39/99151
REFERENCES
- Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269-76.
- [Google Scholar]
- Morphology, mechanisms and pathology of musculoskeletal ageing. J Pathol. 2007;211:252-9.
- [Google Scholar]
- Imaging of diseases of the axial and peripheral skeleton. Radiol Clin North Am. 2008;46:703-33. vi
- [Google Scholar]
- Diagnosis of osteoporosis and assessment of fracture risk. Lancet. 2002;359:1929-36.
- [Google Scholar]
- Sacral insufficiency fractures in the elderly. J Bone Joint Surg Br. 1994;76:882-6.
- [Google Scholar]
- Falls in the elderly: A prospective study of risk factors and risk profiles. Am J Epidemiol. 1996;143:1129-36.
- [Google Scholar]
- Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646-56.
- [Google Scholar]
- Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res. 2005;20:185-94.
- [Google Scholar]
- Vertebral size in elderly women with osteoporosis.Mechanical implications and relationship to fractures. J Clin Invest. 1995;95:2332-7.
- [Google Scholar]
- Vertebral fractures and mortality in older women: A prospective study.Study of Osteoporotic Fractures Research Group. Arch Intern Med. 1999;159:1215-20.
- [Google Scholar]
- Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet. 1999;353:878-82.
- [Google Scholar]
- Bone Diseases: Macroscopic, histological, and radiological diagnosis of structural changes in the Skeleton.Softcover reprint of hardcover. (1st ed. 2000 ed). New York (NY): Springer; 2011.
- [Google Scholar]
- Discrimination of metastatic from acute osteoporotic compression spinal fractures with MR imaging. Radiographics. 2003;23:179-87.
- [Google Scholar]
- Spinal Imaging: Diagnostic Imaging of the Spine and Spinal Cord. (1o ed). New York (NY): Springer; 2007.
- [Google Scholar]
- Radiologic aspects of diffuse idiopathic skeletal hyperostosis in the spine. AJR Am J Roentgenol. 1977;129:913-8.
- [Google Scholar]
- Cervical spine injury in the elderly: Imaging features. Skeletal Radiol. 2001;30:1-7.
- [Google Scholar]
- Prevalence of diffuse idiopathic skeletal hyperostosis in Budapest, Hungary. Rheumatology (Oxford). 2002;41:1335-6.
- [Google Scholar]
- Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res. 2004;19:532-6.
- [Google Scholar]
- Osteoporosis: Diagnosis and management. (1o ed). London (UK): Taylor & Francis; 1998.
- [Google Scholar]
- MRI and CT of insufficiency fractures of the pelvis and the proximal femur. AJR Am J Roentgenol. 2008;191:995-1001.
- [Google Scholar]
- Insufficiency fracture.A survey of 60 cases and review of the literature. Joint Bone Spine. 2003;70:209-18.
- [Google Scholar]
- Sacral insufficiency fractures: An unsuspected cause of low back pain. Br J Rheumatol. 1998;37:789-93.
- [Google Scholar]
- Common rheumatologic diseases in elderly patients. Mayo Clin Proc. 1995;70:1205-14.
- [Google Scholar]
- Clinical, radiologic, demographic, and occupational aspects of hand osteoarthritis in the elderly. Semin Arthritis Rheum. 2001;30:321-31.
- [Google Scholar]
- Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The framingham study. Am J Epidemiol. 2002;156:1021-7.
- [Google Scholar]
- Osteoarthritis.A review of musculoskeletal aging and treatment issues in geriatric patients. Geriatrics. 2004;59:28-32. quiz 35
- [Google Scholar]
- Rotator cuff tears: Clinical, radiographic, and US findings. Radiographics. 2005;25:1591-607.
- [Google Scholar]
- The modic vertebral end plate and marrow changes: Pathologic significance and relation to low back pain and segmental instability of the lumbar spine. AJNR Am J Neuroradiol. 2008;29:838-42.
- [Google Scholar]
- Therapeutic challenges in the management of gout in the elderly. Geriatrics. 2008;63:13-8.
- [Google Scholar]
- [The current role of ultrasound in the assessment of crystal-related arthropathies] Reumatismo. 2009;61:216-21.
- [Google Scholar]
- Calcium pyrophosphate dihydrate crystal deposition disease revisited. Radiology. 1996;200:1-9.
- [Google Scholar]
- Pyrophosphate arthropathy: A clinical and radiological study of 105 cases. Ann Rheum Dis. 1982;41:371-6.
- [Google Scholar]
- Septic arthritis in patients aged 80 and older: A comparison with younger adults. J Am Geriatr Soc. 2005;53:1210-3.
- [Google Scholar]
- Imaging of musculoskeletal soft tissue infections. Skeletal Radiol. 2010;39:957-71.
- [Google Scholar]
- Role of scintigraphy in musculoskeletal and spinal infections. Radiol Clin North Am. 2001;39:169-89.
- [Google Scholar]
- Imaging of musculoskeletal and spinal tuberculosis. Radiol Clin North Am. 2001;39:329-42.
- [Google Scholar]
- Role of ultrasound in musculoskeletal infections. Radiol Clin North Am. 2001;39:191-201.
- [Google Scholar]
- Radiological prevalence of Paget's disease of bone in British migrants to Australia. Br Med J. 1978;1:1655-7.
- [Google Scholar]
- Paget's disease of bone in The Netherlands: A population-based radiological and biochemical survey--the Rotterdam Study. J Bone Miner Res. 2004;19:566-70.
- [Google Scholar]
- Bone Disease in Rheumatology. (1o ed). Philadelphia (PA): Lippincott Williams & Wilkins; 2004.
- [Google Scholar]
- Essentials of Skeletal Radiology. Third. Baltimore (MD): Lippincott Williams & Wilkins; 2004.
- [Google Scholar]
- Magnetic resonance imaging versus radionuclide scintigraphy in screening for bone metastases. Clin Radiol. 1999;54:448-51.
- [Google Scholar]
- ABC of clinical haematology.Multiple myeloma and related conditions. BMJ. 1997;314:960-3.
- [Google Scholar]
- Oncohaematologic disorders affecting the skeleton in the elderly. Radiol Clin North Am. 2008;46:785-98. vi
- [Google Scholar]




