
Translate this page into:
Macrodystrophia Lipomatosa: Radiologic-Pathologic Correlation
Address for correspondence: Dr. Umesh C Parashari, Department of Radio Diagnosis, Era's Lucknow Medical College, Lucknow, UP, India. E-mail: drumesh.rd@gmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Macrodystrophia lipomatosa (MDL) is a rare cause of congenital macrodactyly, characterised by progressive proliferation of all mesenchymal elements, with disproportionate increase in fibro-adipose tissue. It occurs most frequently in lower limbs along the distribution of the medial plantar nerve. MDL presents as localised gigantism of the hand or foot and comes to clinical attention for cosmetic reasons, mechanical problems secondary to degenerative joint disease, or development of neurovascular compression. Here, we report a case of MDL, with altered soft tissue growth due to an earlier surgery, making clinical diagnosis difficult. However, with a complete radio-clinical work-up and review of the history, a provisional diagnosis of MDL was made, which was confirmed by histopathology and during surgery.
Keywords
Fat
local gigantism
macrodystrophia lipomatosa
macrodactyly

INTRODUCTION

Macrodystrophia lipomatosa (MDL) is an unusual form of local hypertrophy also called local gigantism. It is congenital in origin but not hereditary. It is classified as a developmental anomaly. There is marked increase in all mesenchymal elements such as bone, tendons, nerves, vessels, and particularly fibro-adipose tissue.
We report a case of MDL, with altered soft tissue growth resulting from an earlier surgery, making clinical diagnosis difficult. However, after radio-clinical work-up and review of the history, a provisional diagnosis of MDL was made, which was subsequently confirmed by histopathology.
CASE REPORT
A 22-year-old man presented with a disproportionate enlargement of the second, third, and fourth toes of the left foot since birth. There was no history of pain, neurovascular symptoms, or family history of neurofibromatoses. The patient had undergone surgical procedure in the left foot during childhood for the same complaint, and the scar of the earlier surgery was present over the plantar aspect of the foot. On physical examination, a non-tender, non-pulsatile, firm soft tissue mass was palpable over the dorsum of the left foot, with true macrodactyly of the second, third, and fourth toes with plantar deviation. The overlying skin was thick, pale, and glossy without any pitting edema or bruit [Figure 1].

- Photograph shows macrodactyly of the left foot involving second, third, and fourth toes with plantar angulation of the toes.
A plain X-ray of the left foot was performed that revealed soft tissue swelling along the dorsal aspect of the foot, over the second, third, and fourth toes, with diffuse enlargement of the third metatarsal and proximal phalanges of the second, third, and fourth toes with fusion of the third and fourth metatarsal bases. Osteoarthritic changes were noted in metatarsals and metatarsophalangeal joints of the involved toes. A small osseous protuberance over the lateral aspect of the second metatarsal was also noted. There was no evidence of osteolytic or sclerotic lesions, periosteal reaction, or any abnormality in any other bone [Figure 2].

- Plain radiograph shows soft tissue swelling involving second, third, and fourth toes with hypertrophy of phalanges and plantar angulation of the distal end of the affected toes.
Gray-scale ultrasound and colour flow Doppler revealed diffuse soft tissue thickening, without any abnormal calcifications or abnormal blood flow. Computed tomography (CT) of the left foot was performed, which showed marked proliferation of fat containing soft tissue [Figure 3]. A radiological diagnosis of MDL was made in view of the findings described earlier.
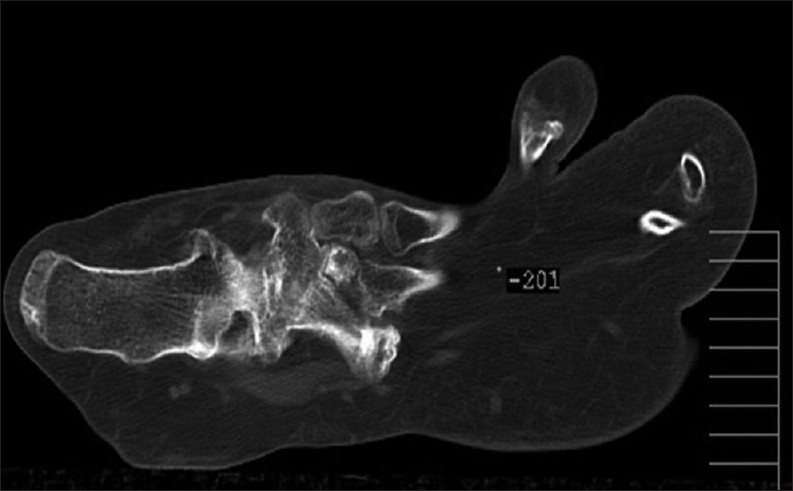
- Computed tomography shows abundant soft tissue with fat density, and fanning of phalanges.
After making the diagnosis, treatment planned was to perform a debulking procedure. Fishmouth incision revealed marked hypertrophy of fat, with adhesions between the skin and periosteum (dermato-osseous bands). A trans-metatarsal amputation was done for the elongated extremity [Figure 4]. Hypertrophied metatarsal bones were cut from the neck and myoplasty was performed between dorsal and plantar compartments [Figure 5]. Debulking of the remaining compartment with orthotic supplementation gave a functional cosmetic foot. Postoperative histopathology of the tissue revealed abundant adipose tissue, thus confirming the diagnosis of MDL [Figure 6].
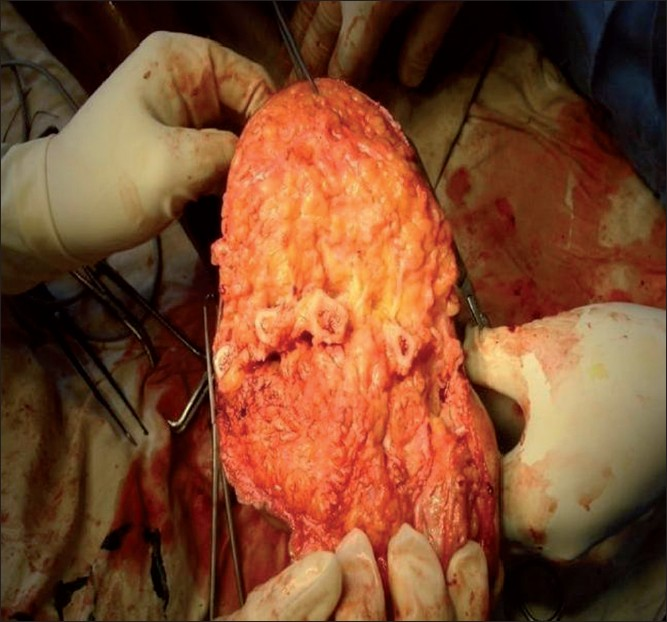
- Intraoperative photograph shows abundant adipose tissue and trans-metatarsal amputation.

- Postoperative photograph taken after myoplasty.
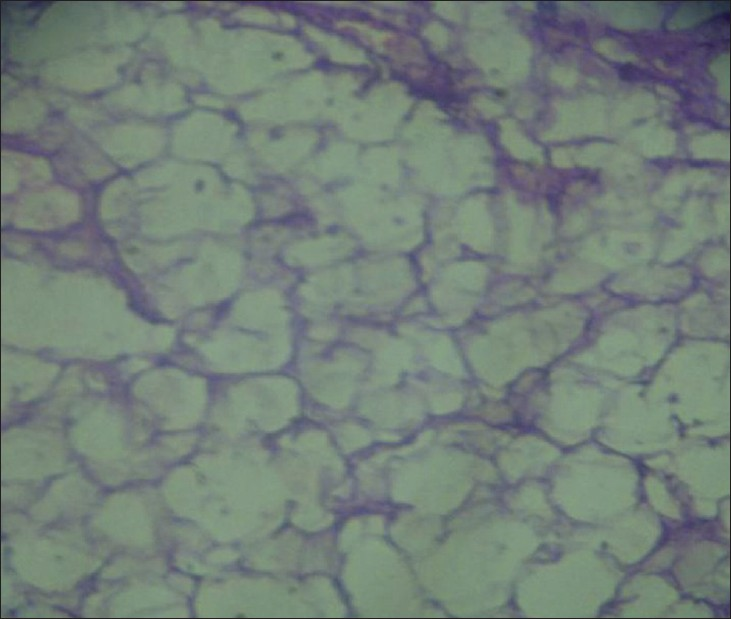
- Histopathology shows abundant adipose tissue.
Cases reported so far have shown excessive soft tissue growth at the distal end and volar aspect of the digit, with dorsal deviation and splaying of digits. But the case in our study is an exception, with marked soft tissue growth over the dorsal aspect of the digit with plantar deviation. Some of the unique features of our case include plantar flexion of the toes, elongation of the extremity including all tarsal bones, fanning of toes, callosity in plantar aspect of the foot, presence of dermato-osseous bands, and thickened periosteum.
DISCUSSION
Macrodactyly is an unusual congenital anomaly in which there is hamartomatous proliferation of soft tissue of the affected digit, which is also called local gigantism.[1] The disorder is congenital in origin, but not hereditary. It is characterised by excessive growth of fibro-fatty tissue with unusually large fatty lobules, apparently fixed by a mesh of dense fibrous tissue. Hypertrophy and tortuosity of the digital nerve, a striking feature in macrodactyly of the hand, is notably absent in cases affecting the foot.[2]
Exact Etiology of the disorder is not known; however, Inglis[3] has described three probable mechanisms: abnormal nerve supply, abnormal blood supply, or abnormal humoral mechanisms. The rate of accelerated growth varies among patients and also among affected digits. Progressive macrodactyly is more common than the static type. It can be present at birth along with syndactyly, digital deviation, thenar eminence hypertrophy, palmar and forearm hyperplasia.[4] Association with small osseous protuberances resembling osteochondromas and lipomas in other parts of the body have also been reported.[5] Its involvement is almost always unilateral as seen in our case. The lower limb is more frequently involved than upper limb, which is typically along a specific sclerotome, with the most common sites being second and third digits corresponding to the median nerve and medial plantar nerve in upper and lower limbs, respectively.[6] Involvement of the fifth digit is a rare occurrence.
Different imaging modalities play a role in the evaluation of MDL. The differential diagnoses include neurofibromatosis, hemangiomatosis, lymphangiomatosis, Proteus syndrome, and fibrolipomatous hamartoma (FLH). Neurofibromas are visible in neurofibromatosis, which demonstrate a marked hyperintensity on magnetic resonance imaging (MRI) in T2-weighted (T2W) images. These are seen in close proximity to nerves. Presence of positive family history, cutaneous lesions, and bilaterality favour the diagnosis of neurofibromatosis, while in macrodystrophia, lipomatosa hypertrophy occurs along a nerve territory. Presence of unilaterality, and fat within the nerve sheath favour MDL. Lymphangiomas are present as focal or diffuse swellings with pitting edema. On CT scan, these appear as multiseptated hypodense masses. On MRI, these appear hyperintense to muscle on T1W and hyperintense to fat on T2W images. A bruit may be palpable in hemangiomatosis, and on MRI, long repetition time/echo time (TR/TE) sequences show a septate configuration of high-signal intensity channels, corresponding to the vascular channels and fibrous strands. Klippel-Trenaunay-Weber syndrome is a rare condition, usually present from birth. It involves port wine stains, excess growth of bones and soft tissue, and varicose veins. Osseous growth is not seen in both lymphangiomatosis and hemangiomatosis. In Proteus syndrome, hemi-hypertrophy occurs that may simulate MDL, but other associated abnormalities like calvarial changes, pulmonary cysts, pigmented nevi, and intra-abdominal lipomas favour the diagnosis of Proteus syndrome. FLH of the nerve is a rare tumour-like condition. In this condition, mature fat infiltrates the neural sheath, with most lesions occurring in the median nerve. Pathologically, in FLH, the deposition of fat occurs within the nerve sheath, while in MDL it occurs throughout the involved part of the digits/extremity. In FLH, neural fascicles separated by fat and connective tissue gives a speckled appearance on MRI.
Amputation is the ultimate therapeutic modality and it is indicated in most cases involving the large digits.[7] Other surgical procedures performed in macrodactyly include stripping of the nerves from their branches or removal of a part of the nerve and end-to-end anastomosis to relieve pain.[89]
CONCLUSION
Determination of the cause of macrodactyly is clinically difficult due to many probable etiologies. Radiological findings help distinguish this condition from other causes of localised gigantism. Differentiating between these conditions is important, as they differ in their course, prognosis, complications, and treatment.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp? 2011/1/18/78264
REFERENCES
- Local gigantism (a manifestation of neurofibromatosis): Its relation to general gigantism and to acromegaly illustrating the influence of intrinsic factors in disease when development of the body is abnormal. Am J Pathol. 1950;26:1059-76.
- [Google Scholar]
- Clinical analysis of 73 cases of macrodactyly. Zhonghua Wai Ke Za Zhi. 2008;46:514-7.
- [Google Scholar]
- Macrodystrophia lipomatosia: A case report. Acta Orthop Traumatol Turc. 2004;38:220-3.
- [Google Scholar]
- Macrodactyly. In: Green D, Hotchkiss R, Pederson W, eds. Greens operative hand surgery (4th ed). Philadelphia: Churchill Livingstone; 1999. p. :533-44.
- [Google Scholar]
- Congenital deformities of the hand and forearm. Philadelphia: Saunders; 1974. p. :610-60.




