
Translate this page into:
Left Internal Carotid Artery Agenesis Associated with Basilar and Left Vertebral Artery Aneurysm
Address for correspondence: Dr. Sadιk Ahmet Uyanιk, Department of Radiology, Ankara Numune Education and Research Hospital, Sιhhiye, Ankara, Turkey. E-mail: sado-86@hotmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Agenesis of the internal carotid artery (ICA) is a rare congenital anomaly. Most of the patients are asymptomatic and it is usually discovered incidentally by computed tomography (CT) or magnetic resonance imaging (MRI). There is close association of the cranial aneurysms and subarachnoid hemorrhage with ICA agenesis. We present a case of a 61-year-old male with left ICA agenesis associated with basilar artery and left vertebral artery aneurysms. The patient complained of headaches and numbness on the right-side of the face. Physical examination showed high blood pressure (210/90 mmHg). Neurological examination revealed nystagmus and decreased sensation on the right-side of the face. Agenesis of left ICA, left carotid canal with basilar and left vertebral artery aneurysms were demonstrated incidentally using CT, MRI, and digital subtraction angiography, as a part of an evaluation for suspected cerebrovascular accident.
Keywords
Agenesis
basilar artery aneurysm
internal carotid artery

INTRODUCTION

Agenesis of the internal carotid artery (ICA) is a rare congenital anomaly with an incidence of 0.01%.[12] ICA agenesis was first presented by Tode in 1787, on a postmortem examination.[3] In 1954, Verbiest reported a case with ICA agenesis recognized by cerebral angiography.[4] The cause of the carotid agenesis is not known, but may be secondary to an insult to the developing embryo.[5] Most patients are asymptomatic, since collateral blood flow provides sufficient cerebral circulation. Patients may later present with subarachnoid hemorrhage secondary to aneurismal rupture, transient ischemic attack, or cerebrovascular insufficiency.
Collateral flow is most commonly supplied through the circle of Willis, but may also be provided by embryonic vessels or the external carotid artery.[6] There is a close association with ICA agenesis and intracranial aneurysms.[78] We report a case of left ICA agenesis associated with basilar and left vertebral artery aneurysms.
CASE REPORT
A 61-year-old male patient presented with headaches and numbness on the right-side of the face. Physical examination showed high blood pressure (210/90 mmHg). Neurological examination revealed nystagmus and decreased sensation on the right-side of the face. The cranial nerve and cerebellar examination were normal. Non-contrast computed tomography (CT) revealed no infarcted area but showed the aneurysms of the basilar and left vertebral artery. Absence of the petrous part of the left carotid canal was overlooked on the non-contrast CT examination. MR imaging showed two contiguous fusiform basilar artery and one left vertebral artery aneurysms, absence of normal flow-voids in the cavernous and petrous portion of the left ICA, and the petrous carotid canal was atretic. There was a small ischemic area in the left occipital lobe with abnormal diffusion restriction observed as hypointense on T1-weighted and as hyperintense on T2- weighted, FLAIR images [Figure 1a,b]. On the non-contrast CT the ischemic area was not identified because the examination was applied in the first 24 hours after the onset of the symptoms.
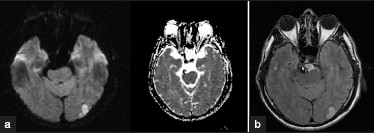
- (a) DWI/ADC MR images show restricted diffusion on the left occipital lobe. (b) T2/FLAIR image shows ischemic signal change on the left occipital lobe and basilar artery aneurysm.
Computed tomography angiography revealed agenesis of the left ICA and left carotid canal [Figure 2]. The caliber of the left common carotid artery (CCA) was diminished and the left CCA terminated in the external carotid artery (ECA), with complete absence of the cervical, petrous, cavernous, and supraclinoid segments of the left ICA [Figure 3a,b]. The right CCA was normal in caliber. Both CT and DSA showed two fusiform basilar artery and one left vertebral artery aneurysms. The left vertebral artery aneurysm was on the distal part of the V4 segment. Bilateral posterior inferior cerebellar arteries (PICA) were normal. One of the basilar artery aneurysm was encountered on the proximal part of the artery before the origin of the anterior inferior cerebellar arteries (AICA). The second aneurysm was found between the origins of the AICA's and superior cerebellar arteries. The AICA's were normal in caliber [Figure 4a–d].

- CT through the skull base reveals absence of the left carotid canal and basilar artery aneurysm.

- (a) Coronal thick-slab MIP image from a contrast-enhanced CTA shows a diminished caliber of the left CCA, terminating in the external carotid artery. The cervical left ICA is absent. The right CCA is normal in caliber. (b) DSA image shows the absence of the entire left ICA.

- (a) DSA image shows two fusiform basilar artery aneurysms and left vertebral artery aneurysm. (b) 3D volume rendered CTA image shows the basilar artery aneurysms. (c) Coronal thick-slab MIP image from a contrastenhanced CTA shows basilar and left vertebral artery aneurysms. (d) Axial thick-slab MIP image from a contrast-enhanced CTA shows prominent PcOA continuing with left MCA.
DSA examination demonstrated that the left anterior cerebral artery (ACA) was supplied through a patent anterior communicating artery (ACoA), and the left middle cerebral artery (MCA) was supplied by the basilar artery via the left posterior communicating artery (PoCoA). Collateral circulation between the left ECA and ICA was not encountered [Figure 5]. Transcranial Doppler sonography showed increased flow velocity in the left posterior cerebral artery [Figure 6].
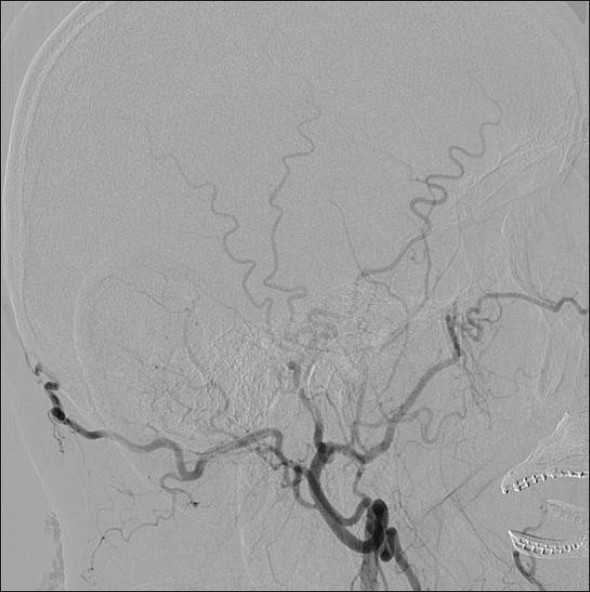
- DSA image of the left ECA. Collateral circulation was not encountered between left ECA and ICA.

- Transcranial color flow Doppler ultrasound shows increased flow velocity in left posterior cerebral artery.
DISCUSSION
ICA agenesis is a rare congenital anomaly, with an estimated incidence of 0.01%, with more frequent symptom encountered in adults rather than in children or adolescent patients.[12] Relatively few symptomatic cases of absence of the ICA have been reported in children, suggesting that initially the collateral pathways are sufficient to support cerebral perfusion.[5] This condition is known to occur more frequently in left sided ICA′s. The ratio between right and left ICAs is 1:3.[9]
Lie[5] referred to agenesis as a complete absence of the entire ICA and carotid canal. The etiology is not known but may be secondary to an insult to the developing embryo. ‘Hypoplasia’ describes the condition when a portion, or remnant, of the artery is present and when the initial segment of the ICA artery is normal in size.[5]
The ICAs are derived from portions of the first and third aortic arches and paired dorsal aorta, when the embryo has attained the 3-mm stage.[10] The roots of the ICAs are formed from the third aortic arches. The dorsal aorta form the intermediate portions of the ICAs, and the distal part of the ICAs are formed from the first aortic arches.[56] Agenesis of the ICA depends on the abnormal regression, involution or atresia of the first and third aortic arches and dorsal aorta in the 20-24-mm embryonic stage. The ECA's arise from aortic sacs and migrate up to the third arches. The portions of the third arches proximal to the ECAs become the CCAs.[8] Although the ICA originates from the third and first aortic arch, the origin of the CCA and ECA remains controversial. Some investigators argue that both the proximal ICA and the ECA arise jointly from the third aortic arch, and thus agenesis of the ICA should be accompanied by absence of the ipsilateral ECA. Others argue that the ECA and CCA can develop normally in the setting of ICA agenesis, as the former arises independently from the aortic sac. The latter seems more plausible, as numerous cases of ICA agenesis exist in the literature with normally developed ECA systems.[5611] The carotid canal develops in association with the ICA. The skull base does not begin to form until the 5th to 6th weeks of fetal life. If the embryonic primordium of the ICA fails to develop before the 3rd and 5th embryonic weeks, the ICA and the carotid canal cannot develop.[1213]
Collateral circulation accompanying ICA agenesis can be classified into three forms; 1) through the circle of Willis, 2) persistent embryonic vessels, 3) transcranial anastomosis from the ECA.[8] Tsurata et al,[14] proposed three types of collateral channels via the circle of Willis. In Type I, the ipsilateral ACA is supplied by the contralateral ICA, opposite to the ICA agenesis, via the ACoA. The MCA is supplied by the basilar artery via the PoCA. In Type II, the ipsilateral ACA and MCA are supplied by the contralateral ICA via patent ACoA. In Type III, ipsilateral ACA and MCA are supplied by the transcranial anastomoses that develop from ECA or contralateral ICA or primitive vessels. In our case, Type I anastomosis was determined by CT and angiographic examination.
Patients with agenesis of the ICA are often asymptomatic because of the collateral pathways. However, patients may present with headaches, seizures or neurological deficits secondary to cerebral ischemia, or intracranial hemorrhage.[8] Our patient had nystagmus and decreased sensation on the right-side of the face. There was a small ischemic area in the left occipital lobe with abnormal diffusion restriction observed as hypointense on T1-weighted and as hyperintense on T2-weighted, FLAIR images. On DSA there was not any occlusion of the cranial vessels. The ischemic area may be due to thromboembolic event or microangiopathic changes.
Diagnosis of ICA agenesis entails documenting the absence of the ICA by conventional angiography, MRA or MSCT angiography, and the absence of the carotid canal by CT. Collateral flow is most commonly supplied through the circle of Willis, but may be also provided by embryonic vessels or the external carotid artery.
Intracranial vascular anomalies can be associated with ICA agenesis. The incidence of intracranial aneurysm in association with ICA agenesis has been reported in 25-43% of the patients, which is much higher than that found in general population, 2-4%.[78] Two mechanisms have been postulated to explain this strong association between ICA agenesis and intracranial aneurysm; 1) the aneurysm may develop secondary to hemodynamic derangement, or 2) the aneurysm may form during embryonic life because of a developmental error. The first mechanism might be attributed to the increased hemodynamic load on the normal side vessels. Lee et al.[8] reported that in their series of six patients, aneurysms arose ipsilateral side to the aplasic ICA, supporting a congenital origin as opposed to hemodynamic factors. The fusiform basilar and left vertebral artery aneurysms in our case may have arisen secondary to hemodynamic stress on the vertebral and basilar artery by supplying the left middle cerebral artery via the PCoA. The increased flow velocity in the left posterior cerebral artery might reflect the increased hemodynamic stress placed on the posterior circulation.
Uni- or bilateral ICA agenesis associated with basilar artery aneurysm has been published in the literature. Elazab et al[15] reported a 2-month-old baby presented with right oculomotor nerve palsy associated with right ICA agenesis and basilar artery aneurysm. Lee et al[8] presented one case of basilar artery aneurysm and hypoplasia of bilateral ICA on a review of nine patients with ICA agenesis-hypoplasia.
Our patient has no complaints at present and is being followed up with periodic physical and neurological examination.
CONCLUSIONS
ICA agenesis is a rare vascular anomaly and is typically discovered incidentally as patients are often asymptomatic. Congenital absence of the ICA is associated with a higher incidence of aneurysm formation. Patients with ICA agenesis or hypoplasia should therefore undergo evaluation for the presence of intracranial aneurysms. Patients may present with cranial nerve deficits, cerebral ischemia, or subarachnoid hemorrhage secondary to complications of associated aneurysm formation. This rare anomaly must be distinguished from ICA stenosis or occlusion. The collateral circulation should also be documented by conventional angiography, particularly prior to carotid endarterectomy, transsphenoidal hypophyseal surgery or inducing hypotension. Collateral flow is most commonly supplied through the circle of Willis, but may be also provided by embryonic vessels or the external carotid artery.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2011/1/1/60/91133
REFERENCES
- Bilateral ‘hypoplasia’ of the internal carotid arteries. Neurology. 1968;18:1149-56.
- [Google Scholar]
- Cerebral hemiatrophy, hypoplasia of internal carotid artery and intracranial aneurysm. Arch Neurol. 1987;44:232-5.
- [Google Scholar]
- Agenesis of the Left Internal Carotid Artery Associated with anterior communicating artery aneurysm: Case Report. Turk Neurosurg. 2007;17:273-6.
- [Google Scholar]
- Radiologic findings in a case with absence of the left internal carotid artery and compression of several cranial nerve roots in the posterior fossa by the basilar artery. Med Contemp. 1954;71:601-9.
- [Google Scholar]
- Congenital anomalies of the carotid arteries. Amsterdam: Excerpta Medica; 1968. p. :44-9.
- [Google Scholar]
- Congenital absence of the internal carotid artery: Case reports and review of the collateral circulation. AJNR Am J Neuroradiol. 2001;22:1953-9.
- [Google Scholar]
- Agenesis of left internal carotid artery, common carotid artery, and main trunk of external carotid artery associated with multipl cerebral aneurysyms. Surg Neurol. 1987;27:177-81.
- [Google Scholar]
- Congenital absence of the internal carotid artery. Cardiovasc Intervent Radiol. 1999;22:74-8.
- [Google Scholar]
- The development of the cranial arteries in the human embryo. Contrib Embryol. 1948;32:207-62.
- [Google Scholar]
- Congenital absence of the cervical and petrous internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1989;10:435-9.
- [Google Scholar]
- Unilateral agenesis and hypoplasia of the internal carotid artery: A report of three cases. Neuroradiology. 2005;47:311-5.
- [Google Scholar]
- A case of complete absence of the internal carotid artery associated with an aneurysm of anterior communicating artery. No To Shinkei. 1977;5:895-900.
- [Google Scholar]
- Internal carotid artery agenesis and basilar artery aneurysm with third nerve palsy. Pediatr Neurol. 2010;42:451-4.
- [Google Scholar]




