
Translate this page into:
Incidental Finding of Dual Ectopic Thyroid on Computed Tomography Angiography
Address for correspondence: Dr. Antonio Pierro, Department of Radiology, Fondazione di ricerca e cura “Giovanni Paolo II,” Università Cattolica del Sacro Cuore, Largo Gemelli 1, Campobasso, Italy. E-mail: apierrojonico@libero.it
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The presence of simultaneous two ectopic foci of thyroid tissue (dual ectopic thyroid) is rare, and few cases have been reported in the literature. The ectopic thyroid tissue is an extremely uncommon embryological aberration due to the alterations occurring during the embryological development with incomplete migration of thyroid precursors. Commonly ectopic thyroid tissue is a midline structures, but the lateral location is possible but very rare. Ectopic thyroid is common in women and can vary in size from a microscopic focus to a few centimeters. The normal process of migration of the thyroid can be interrupted at various levels determining a lingual ectopy, a sublingual ectopic, prelaryngeal ectopy, or mediastinic ectopy. Intrathoracic and subdiaphragmatic organs are other sites where the ectopic thyroid tissue may be present. In most of the cases, ectopic tissue is a lingual thyroid and this condition can be totally asymptomatic, discovered incidentally, or occurs with symptoms such as dysphonia, dysphagia, dyspnea, and hemoptysis. Sublingual or suprahyoid ectopia is rare and even rarer are the cases of two foci of ectopic thyroid tissue simultaneously present. On imaging, the ectopic tissue shows the same characteristics of orthotopic thyroid tissue and similarly can undergo goiterous and cancerous transformation. We report a case of incidental dual ectopic thyroid in lingual and suprahyoid level in a 72-year-old female patient, asymptomatic and with normal thyroid function, who underwent computed tomography (CT) angiography before vascular surgery for the treatment of carotid stenosis. The presence of a lingual thyroid can lead to a difficult and dangerous intubation, with possible fatal consequences. For this reason, the discovery of these abnormalities has totally changed the patient management who has been subjected to endovascular treatment, instead to the classical surgery.
Keywords
Dual ectopia
ectopic thyroid
incidental
lingual thyroid
suprahyoid thyroid


INTRODUCTION
The thyroid gland is composed of two lobes, the right and the left lobe, commonly interconnected by a parenchymal bridge called isthmus. The gland is localized in the anterior and anterolateral part of the larynx and the trachea, approximately at the level of the second and third tracheal ring, posterior to the infrahyoid strap muscles. Two distinct cell types, thyroid follicular cells and parafollicular cells, compose the thyroid gland.
From median thyroid anlage, along the midline of the floor of the primitive pharynx, the endodermal thickening between the first and second pharyngeal pouches originates the follicular cells.
This endodermal thickening (the thyroid bud) around the 4th week of development elongates into a bilobate diverticulum (the primitive thyroid). In the next 3 weeks, the diverticulum engages the underlying mesenchymal tissue and descends in the midline of the neck, front to the hyoid bone and subsequently in the infrahyoid portion of the neck. At the end of the 7th week of gestation, the thyroid reaches its final location in pretracheal position.
The diverticulum pathway during its descent forms a small canal, the thyroglossal duct (TGD), which connects the tongue with the primordial thyroid gland. Subsequently, around the 8th week of gestation, the TGD undergoes a regressive process before the final formation of the thyroid. The caudal portion of the TGD may persist in some individuals forming the pyramidal lobe (Lalouette's pyramid). The opening of the TGD into the tongue, named foramen cecum, represents a definitive pit at the apex of the sulcus terminalis on the dorsum of the tongue [Figure 1]. The lateral thyroid anlagen (ultimobranchial bodies), deriving from the fifth branchial pouches, insinuates inferiorly in both sides of the neck providing the parafollicular cells. Finally, the two buds of the thyroid, the medial and the lateral, merge together to form the gland in its entirety.[12]

- Scheme of course of the thyroid during embryological development: the thyroglossal duct is a small epithelial channel between the foramen cecum of the tongue and the thyroid gland that develops during migration and descent of the thyroid to its final location. If the descent process and migration of the thyroid is not successful during embryological development, an ectopic thyroid gland can develop at any point along this tract.
The embryology knowledge allows us to understand the anatomical variants.
Rarely, the normal descent of thyroid anlages may fail, leading to the genesis of ectopic thyroid tissue, typically as midline structures. During the embryonic development, the normal process of migration of the thyroid can be interrupted at various levels determining a lingual ectopy (ectopic thyroid included in the base of the tongue), or a sublingual or suprahyoid ectopic (ectopic thyroid tissue between the geniohyoid and mylohyoid muscles or just above the geniohyoid muscle, respectively), or a prelaryngeal ectopy (anterior to the larynx), or a mediastinic ectopy. Parotid glands, lung, heart, breast, esophagus, and subdiaphragmatic organs are other sites where the ectopic thyroid tissue may be present.[3] In 90% of cases, ectopic tissue is a lingual thyroid; its incidence range between 1 in 3000 and 1 in 100,000 cases.[1] In 70% of cases, ectopic thyroid gland was absent from the pretracheal region. The lingual thyroid is common in women and can vary in size from a microscopic focus to a few centimeters; this condition can be totally asymptomatic, discovered incidentally, or occurs with symptoms such as dysphonia, dysphagia, dyspnea, and hemoptysis.[345]
The lingual thyroid is the most common form of ectopia, and at present, about 400 cases have been reported. The cases of suprahyoid ectopia are rare and even rarer are the cases of two foci of ectopic thyroid tissue present simultaneously.[6]
We present an extremely rare case of dual ectopic thyroid (dual ectopia) in a totally asymptomatic woman. This patient was candidate for carotid endarterectomy, but the timely identification of this anomaly on CT angiography has changed patient management, by preferring endovascular treatment than surgery, then avoiding the occurrence of serious complications during intubation.
CASE REPORT
A 72-year-old female patient, with a symptomatic carotid stenosis previously identified by ultrasonography, has come to our attention to perform a CT angiography of the neck vessels. CT angiography examination showed the presence of a severe degree of carotid stenosis (equal to about 85% calculated with the North American Symptomatic Carotid Endarterectomy Trial method); therefore, the patient was candidate to perform a carotid endarterectomy (CEA).
However, the CT angiography has identified some significant incidental findings that have profoundly changed the patient management.
CT angiography identified an oval soft-tissue mass, well circumscribed with regular margins, with size of 34 mm × 28 mm × 23 mm, localized at the base of the tongue along the midline, with avid and inhomogeneous enhancement. This mass changed the aspect of the base of the tongue showing a major bulging on the lumen of the oropharynx, with a significant reduction of the caliber of the air column. More inferiorly, just above the geniohyoid muscle on the midline and in proximity to the hyoid bone, we detected another oval, soft-tissue mass with the same characteristics previously described, and a size of 12 mm × 22 mm × 22 mm. Finally, CT angiography revealed the absence of thyroid tissue in its normal position [Figure 2].

- A 72-year-old-female patient with a symptomatic carotid stenosis. Axial computed tomography images demonstrate: (a) absence of the thyroid in its physiological localization (yellow arrowhead), (b and c) lingual and suprahyoid thyroid (yellow arrowheads). Volume rendering and multiplanar reformations images demonstrate: (d-f) the suprahyoid location of both foci of ectopic thyroid tissue in the tongue base (white arrow) and just above the course of geniohyoid muscle (yellow arrow) and the severe reduction of the oropharynx caliber (yellow arrowhead).
The knowledge of the embryologic thyroid course, the absence of thyroid gland in its normal position, the location of the two masses along the midline, and their appearance on CT-scans suggest a dual ectopic thyroid, a lingual thyroid (in the base of the tongue) and suprahyoid thyroid (just above the geniohyoid muscle on the midline, in close proximity to the hyoid bone), respectively.
The ultrasound evaluation of the sublingual mass, performed by a linear array transducer (10–15 MHz), documented the typical ultrasound characteristics of the thyroid tissue [Figure 3].
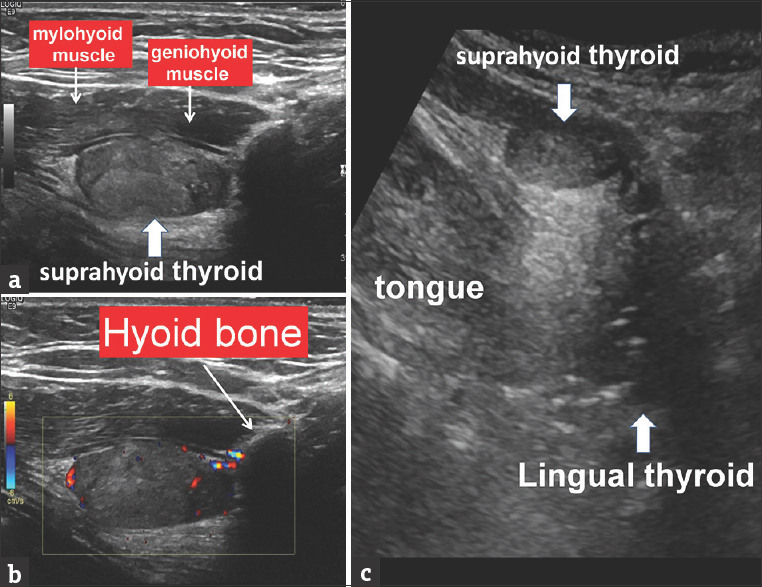
- A 72-year-old female patient with a symptomatic carotid stenosis. Ultrasound examination showed: (a and b) Soft-tissue mass, vascularized, with sonographic findings suggestive of thyroid tissue, located just above the geniohyoid muscle in the sublingual and suprahyoid space. (c) With convex-array scanner, in more cranial and posterior position, at the level of the tongue base, there is a hypoechoic oval mass indicate a lingual thyroid.
The patient was then evaluated by otorhinolaryngology and the diagnosis of lingual thyroid was clinically confirmed. Thyroid function tests were found in the normal range.
This patient was originally scheduled for CEA which is effective in preventing ipsilateral ischemic events in patients with symptomatic moderate and high-grade stenosis. The radiological detection and subsequently clinical confirmation of lingual thyroid addressed the patient to an endovascular procedure, by carotid angioplasty and stenting. This alternative approach was chosen to minimize the risks of an endotracheal intubation, such as hemorrhage and compromised airway. In particular, the large blood vessels on the surface of the lingual thyroid could be traumatized by the insertion of any instruments during intubation, with potential onset of hemorrhage and compromised airway.[7]
DISCUSSION
An abnormal embryological development of the thyroid tissue and its incomplete migration cause the development of ectopic thyroid tissue at different sites from its normal pretracheal location. An ectopic thyroid is rare abnormality that occurs in about 1 in 3000–1 in 10 000 people.[4]
The ectopic thyroid locations are usually along the midline of the neck and the pathway of the TGD, between the foramen cecum and the thyroid gland during development.
The lateral location of the ectopic thyroid is rare, but possible; however, in the side localizations, the ectopic thyroid is always closely adjacent to the infrahyoid strap muscles.[2]
However, ectopic thyroid tissue can also be present in different sites from the normal downward path during development; in fact, it may be found in the intratracheal, intrathoracic (mediastinum, lungs, and heart), and subdiaphragmatic location (gallbladder, porta hepatis, ovaries, adrenals, pancreas, duodenum, and mesentery, small bowel mucosa, uterus, and vaginal wall).[8]
The base of tongue is the most frequent (about 90% of cases) location of ectopic thyroid tissue (known as lingual thyroid); this condition can be totally asymptomatic, discovered incidentally, or occurs with symptoms such as dysphonia, dysphagia, stomatolalia, sensation of foreign body, cough, sleep apnea, dyspnea, and hemoptysis.[3458]
On imaging, the ectopic tissue shows the same characteristics of orthotopic thyroid tissue. Because of its intrinsic content of iodine, the CT examination performed without administration of contrast medium shows a mildly increased attenuation (70 HU ± 10) compared to adjacent muscles. The CT examination performed with contrast medium administration presents an avid homogeneous enhancement. Typically, on T1-weighted MR (magnetic resonance) images, ectopic thyroid tissue appears isointense to mildly hyperintense compared to adjacent muscles and mildly hyperintense on T2-weighted MR images, with variable enhancement after gadolinium administration.
On CT and MR imaging the sagittal plane is certainly to be preferred because these ectopic tissue islands are typically midline structures.[2]
Scintigraphy with technetium-99 m, iodine-131 or iodine-131 is critical in the presence of masses of the neck, suspicious for ectopic thyroid tissue, especially if localized along the midline, thanks to its high sensitivity.[9]
Sonography is a noninvasive imaging method to evaluate the presence of the ectopic and orthotopic thyroid tissue. Using this imaging modality, the lingual thyroid usually appears as a solid mass with low echogenicity, showing the same aspect of the typical thyroid parenchyma.[1011] The color-power-Doppler technique increases the sensibility of sonography.[10] In addition, for deeply localized tissues (as lingual thyroid), the use of convex probes with low frequency is preferable.[12]
In analogy with the orthotopic thyroid tissue, the ectopic thyroid can undergo goiterous and cancerous transformation.[1314]
However, unknown ectopia, in particular the lingual thyroid, poses several other serious problems, as difficulties in intubation during surgery with possible fatal consequences because of hemorrhaging and airway compression. This way, an a-priori identification of lingual thyroid, is essential for the surgeon and the anesthesiologist to plan assisted anesthetic procedures required to minimize the risks.[715]
CONCLUSION
This case report highlights the importance of presurgical evaluation and the role of multidisciplinary communication between physicians and radiologists to avoid possible fatal consequences of intubation during surgery.
Our work describes the extremely rare case of the presence of two ectopic foci of thyroid tissue simultaneously present in a patient. We have emphasized that in the presence of an ectopic thyroid focus, it is necessary to check for the existence of additional ectopic focuses which may pose a serious risk for the patient.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2017/7/1/30/212074
REFERENCES
- Anatomy and embryology of the thyroid and parathyroid glands. Semin Ultrasound CT MR. 2012;33:104-14.
- [Google Scholar]
- Imaging of ectopic thyroid tissue and thyroglossal duct cysts. Radiographics. 2014;34:37-50.
- [Google Scholar]
- Lingual thyroid causing dysphagia and dyspnoea. Case reports and review of the literature. Acta Otorhinolaryngol Ital. 2009;29:213-7.
- [Google Scholar]
- CT and MRI findings of developmental abnormalities and ectopia varieties of the thyroid gland. Diagn Interv Radiol. 2012;18:335-43.
- [Google Scholar]
- Hemoptysis caused by ectopic lingual thyroid. Quant Imaging Med Surg. 2015;5:480-2.
- [Google Scholar]
- Thyroid scintigraphy in detecting dual ectopic thyroid: A review. Eur J Nucl Med Mol Imaging. 2008;35:843-6.
- [Google Scholar]
- Ectopic thyroid tissue: Anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011;165:375-82.
- [Google Scholar]
- The ectopic thyroid gland and the role of nuclear medicine techniques in its diagnosis and management. Hell J Nucl Med. 2008;11:168-71.
- [Google Scholar]
- Radiology quiz case 2.Dual ectopic subhyoid and lingual thyroids. Arch Otolaryngol Head Neck Surg. 2007;133:941-2.
- [Google Scholar]
- Lingual thyroid: Ultrasound assessment and diagnosis. J Med Ultrasound. 2014;22:167-9.
- [Google Scholar]
- Morphological, diagnostic and surgical features of ectopic thyroid gland: A review of literature. Int J Surg. 2014;12(Suppl 1):S3-11.
- [Google Scholar]




