
Translate this page into:
Dual left anterior descending artery: A case report

*Corresponding author: Hunaina Shahab, Department of Cardiology, Mount Sinai West, New York, United States. hunaina.shahab@mountsinai.org
-
Received: ,
Accepted: ,
How to cite this article: Kassem J, Yildiz A, Gowda M, Shahab H. Dual left anterior descending artery: A case report. J Clin Imaging Sci. 2024;14:47. doi: 10.25259/JCIS_122_2024
Abstract
Dual left anterior descending (LAD) coronary artery is a rare anatomical variant with significant clinical implications. Recognizing this variant is crucial for accurate diagnosis and effective management, particularly in the context of revascularization strategies. We present a 71-year-old male with a history of dyspnea on exertion with baseline wall motion abnormality on a transthoracic stress echocardiography irreversible after exercise. Coronary computed tomography angiography revealed a dual LAD system: The left short LAD (LAD1) originating from the left main coronary artery and the right LAD (LAD2) arising separately from the right coronary cusp, distinct from the right coronary artery ostium. Having different origins and courses, both LADs supply the LAD territory. Our case is notable for two main reasons: The rarity of this particular type of dual LAD anatomy and the unique course of the LAD2, which, to our knowledge, has not been described in any previous case report. Although rare, dual LAD coronary artery should be considered in patients with atypical short LAD. Comprehensive imaging and a thorough understanding of coronary artery variants are essential for accurate diagnosis and effective management.
Keywords
dual left anterior descending
congenital anomalous coronary arteries
separate right coronary artery and LAD2 ostia

INTRODUCTION
Normal coronary artery anatomy is characterized by the presence of two ostia rising from the left and right coronary cusps (RCCs). The left coronary system originates from the left coronary cusp, giving rise to the left main coronary artery (LMCA) that bifurcates into the left anterior descending artery (LAD) and the left circumflex coronary artery (LCX) which courses around the atrioventricular groove, and the right coronary system originates from the RCC and courses backward in the right atrioventricular groove.[1]
Congenital anomalous coronary arteries (CACAs) are rare and challenging to recognize. Coronary anomalies can occur as primary isolated forms, or as secondary forms in association with congenital heart disease (such as pulmonary atresia with intact interventricular septum or hypoplastic left heart syndrome with aortic atresia and severe mitral stenosis).[1]
The most common CACA is the separate origin of the LAD and the LCX with an incidence of 0.41% followed by LCX arising from the right coronary artery (RCA), with an incidence of 0.37%.[2]
Dual LAD is an uncommon condition characterized by different anatomical variations, all refer to two distinct arteries supplying all or a portion of the LAD territory, often a short LAD and a long LAD. The short LAD usually ends in the mid-septum but can extend high in the proximal portion.[2] The long LAD pathway frequently varies proximally and can go beyond the usual pathway, but the typical characteristic is that it reaches the distal of the anterior interventricular sulcus (AIVS).[2]
This paper aims to highlight a rare variation of the dual LAD anatomy where LAD2 originates from the RCC, separate from the ostium of the RCA.
CASE REPORT
A 71-year-old male with a history of type II diabetes mellitus, hyperlipidemia, and hypertension was referred to the cardiology clinic following an abnormal ECG, which revealed sinus bradycardia and a new interventricular conduction delay with a QRS interval of 130ms. The patient denied experiencing chest pain, either at rest or during exertion, but reported dyspnea on exertion, specifically when climbing one flight of stairs.
Given these findings, the patient underwent an exercise transthoracic stress echocardiography, which was notable for moderate shortness of breath, possibly indicating an anginal equivalent. The stress electrocardiogram was non-diagnostic due to baseline ST and T wave abnormalities. Echocardiography also revealed baseline akinesia involving the basal septum and basal inferior wall, with no evidence of reversible ischemia.
To further evaluate for coronary artery disease, a Coronary Computed Tomography Angiography (CCTA) was performed. The CCTA demonstrated dual left anterior descending (LAD) artery anatomy. The first LAD (LAD1) originated from the left main coronary artery (LMCA) and terminated in the proximal anterior interventricular sulcus (AIVS), while the second LAD (LAD2) originated separately from the right coronary cusp (RCC) via a separate ostium from the right coronary artery (RCA) and extended to the distal AIVS [Figures 1 and 2]. The CCTA also showed a calcified plaque causing 30% stenosis in the proximal LAD1. Additionally, a branching, medium-sized ramus intermedius coronary artery was observed, free of stenosis.
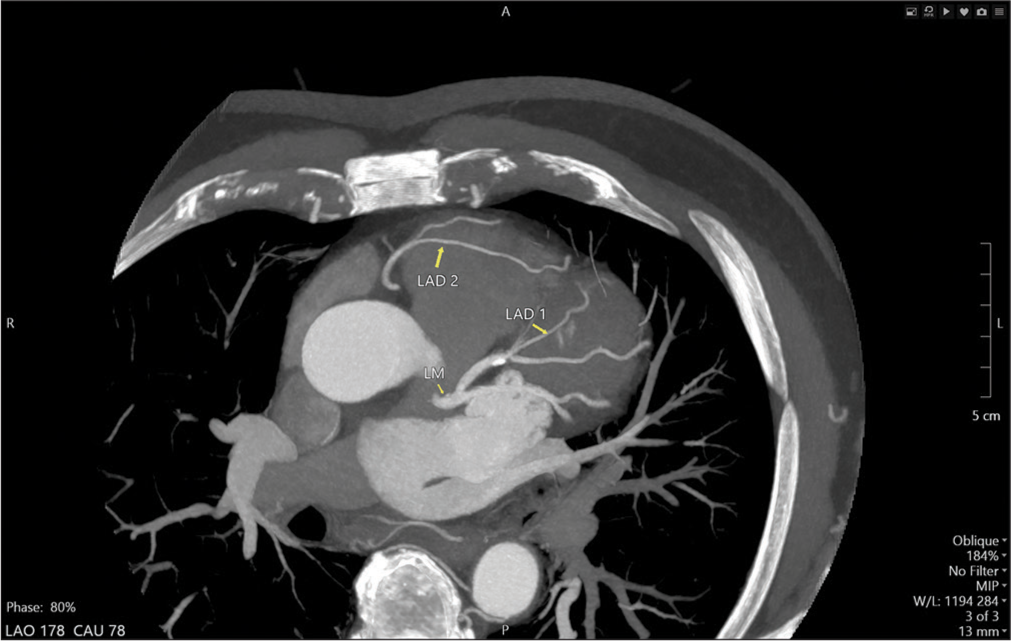
- Maximum intensity projection computed tomography coronary angiography image shows the short left anterior descending (LAD1 yellow arrow) arising from the left main (LM yellow arrow) coronary artery and terminating in the proximal anterior interventricular sulcus (AIVS). The right left anterior descending (LAD2 yellow arrow) arising from the right coronary cusp and terminating in the distal AIVS.
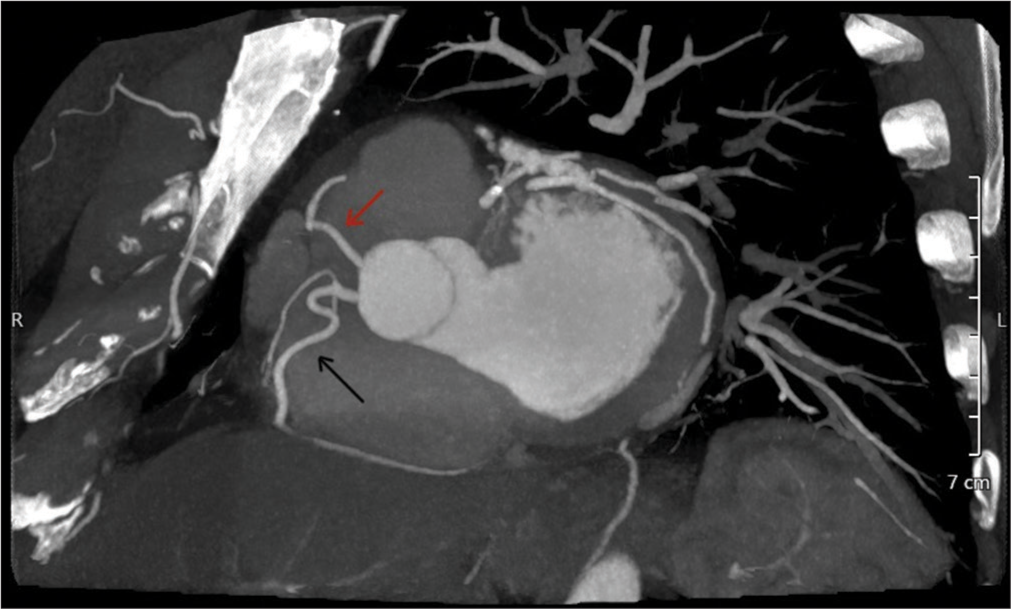
- Maximum intensity projection computed tomography coronary angiography image showing the two separate ostia of the right coronary artery (black arrow) and the right left anterior descending (red arrow).
Given the findings, the patient was initiated on guideline-directed medical therapy, with no current indication for invasive coronary angiography.
DISCUSSION
Since the first recognition of dual LAD anatomy, there have been multiple suggestions for a clear classification of the anatomical variations. Beginning with Spindola-Franco et al. in 1983, followed by numerous case reports and case series with unclassified types of dual LAD, Jariwala et al. finally suggested a new classification of the various anatomical variations of dual LAD based on angiographic and autopsy findings, in an attempt to cover the unclassified types of dual LAD anatomy.[3]
Group I or the “split” dual LAD system: LAD1 and LAD2 bifurcate from the proper LAD coming from the LMCA. In this group, the whole left coronary system and its major branches arise from the left coronary sinus (LCS).
Group II or the “true” dual LAD system: The dual LAD originates partially from the LCS and the right coronary sinus (RCS). The left-sided LAD or LAD1 (coming from the LCS) terminates in the proximal AIVS and the right-sided LAD or LAD2 originates from the RCS or any segment of the RCA and enters the distal IAVS to terminate into the LV apex
Group III or the “anomalous” dual LAD system: The entire left coronary system arises from the RCS and lacks a constant morphological feature.
These three groups further divide into subgroups with a variety of characteristics, complicating the understanding of dual LAD anatomy and adding to its diversity.
In our patient, the anterior wall of the LV was supplied by two LADs. The LAD1 emerged from the LMCA ending abruptly in the proximal IAVS. The LAD2 originated from the RCC separately from the RCA ostium, traversed toward the left side, anterior to the right ventricular outflow tract (RVOT), and entered the mid AIVS to terminate distally [Figure 3].
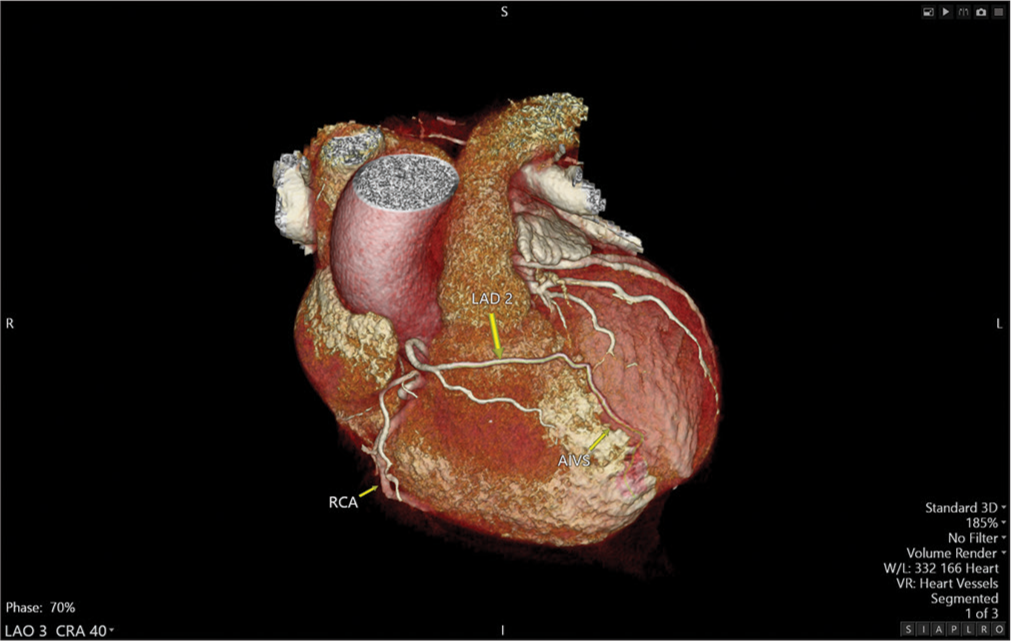
- Three-dimensional volume rendered computed tomography coronary angiography image shows the right left anterior descending arising from the right coronary cusp traverses to the left side anterior to the right ventricular outflow tract and terminates in the distal anterior interventricular sulcus. (LAD2 (yellow arrow): Long left anterior descending artery, RCA (yellow arrow): Right coronary artery, AIVS (yellow arrow): Anterior interventricular sulcus).
Our case falls under class IIA based on the new classification proposed by Jariwala et al.[3] representing a rare entity within this subgroup. To the best of our knowledge, there are only two reported cases of LAD2 originating from RCC separate from the RCA: Deora et al.[4] and Prasad et al.[5] describing similar cases but with a different LAD2 course: The LAD2 after rising from the RCC, traversed toward the left, between the RVOT and aortic root, terminating in the mid to distal interventricular groove.
About only 20% of dual LAD anomalies have symptoms while the majority are asymptomatic, as in our case.[3]
Diagnosis is mainly incidental and based on the suspicion of coronary artery abnormalities on cardiac imaging. CCTA, coronary magnetic resonance angiography, and transthoracic echocardiography are valuable non-invasive imaging modalities in the diagnosis of such cases.[6] Coronary angiography, an invasive procedure, is still the gold standard for diagnosis given its ability to perform corrective intervention for coronary artery atherosclerotic disease if required, but CCTA is more 3D omniplanar in assessing the origin, course, and connection with other cardiac and non-cardiac structures.[6] These modalities can be used for planning surgical revascularization when needed, which requires a precise understanding of the coronary anatomy. The presence of a dual LAD system, with all its variations, should be clearly identified for the revascularization of the correct arterial system and the prevention of inappropriate arteriotomy.[7]
CONCLUSION
Overall, a short LAD, identified on any imaging modality, should prompt consideration of a dual LAD system, particularly if there is an absence of coronary arteries supplying the left ventricle apical region.
Recognizing and understanding the dual LAD anatomy is crucial in the decision-making process of revascularization, whether by surgical or percutaneous catheter-based approaches. Detailed anatomical knowledge of the dual LAD system can optimize procedural outcomes, ensuring comprehensive care for patients with this unique coronary artery configuration.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Congenital anomalies of the coronary arteries. Heart. 2005;91:1240-5.
- [CrossRef] [PubMed] [Google Scholar]
- Dual left anterior descending artery: Clinical overview and interventional management. J Tehran Heart Cent. 2023;18:146-50.
- [CrossRef] [PubMed] [Google Scholar]
- Dual left anterior descending artery: Case series based on novel classification and its therapeutic implications. Indian Heart J. 2022;74:218-28.
- [CrossRef] [PubMed] [Google Scholar]
- Reporting a novel variant of type VI dual left anterior descending artery: A rare coronary anomaly. BMJ Case Rep. 2015;2015:bcr2015211128.
- [CrossRef] [PubMed] [Google Scholar]
- Comment on: Dual LAD with anomalous origin of long LAD from right coronary sinus: A variant of type VI LAD. Indian J Radiol Imaging. 2017;27:362-3.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of anomalous origin of coronary artery detected by multi-detector computed tomography at one center. J Cardiol. 2011;57:69-76.
- [CrossRef] [PubMed] [Google Scholar]
- A rare case of a type IV dual left anterior descending artery and ectopic left anterior descending and circumflex arteries requiring surgery. J Tehran Heart Cent. 2022;17:71-4.
- [CrossRef] [PubMed] [Google Scholar]




