
Translate this page into:
Breast Involvement by Hematologic Malignancies: Ultrasound and Elastography Findings with Clinical Outcomes
Address for correspondence: Dr. Hulya Aslan, Department of Radiology, Faculty of Medicine, Baskent University, Adana Dr. Turgut Noyan Teaching and Medical Research Center, Dadaloglu Mh, Adana, Turkey. E-mail: hul_yaaslan@hotmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
Hematological malignancies very rarely involve the breast. The aim of this study is to retrospectively evaluate B-mode ultrasound (US) and elastography (ES) findings of breast involvement by hematologic malignancies with clinical outcomes.
Materials and Methods:
All core-needle biopsy results that were performed at our tertiary breast center from January 2013 to September 2016 were searched. Our search revealed 9 patients with breast involvement either by leukemia or lymphoma. All patients were examined using B-mode US and ES. US and ES findings were analyzed with the consensus of two radiologists, and clinical outcomes were noted.
Results:
The mean age of the study population was 41.6 years (range, 20–83 years). Two patients showed diffuse hypoechoic parenchymal infiltration. The elasticity assessments of these lesions were soft and intermediate. The remaining 7 patients had mass lesions. The elasticity assessment of these masses according to Breast Imaging Reporting and Data System US was as follows: Soft (n = 1), intermediate (n = 4), high (n = 2).
Conclusions:
It is important to consider that hematologic malignancies may appear as soft or intermediate lesions on ES. Patients’ history and clinical background should help us to consider breast involvement. In addition, the clinical outcomes may not be related with elasticity assessments.
Keywords
Breast
elastography
leukemia
lymphoma
ultrasound


INTRODUCTION
Hematological malignancies very rarely involve the breast.[1] Lymphoma and leukemia are the most common hematological malignancies affecting the breast.[2] The published data on clinical and radiological features of breast leukemia and lymphoma depends predominantly on case reports or case series. Mammography, magnetic resonance imaging (MRI) and B-mode ultrasound (US) findings of breast leukemia and lymphoma have already been reported.[1345678] However, elastography (ES) findings of breast involvement by hematological diseases have rarely been reported.[91011] Gkali et al., reported a case of primary non-Hodgkin's lymphoma of the breast that was soft, and Barr et al., reported a case of breast lymphoma with a soft lesion on ES.[910] Then, Barr et al., also reported four cases of primary breast lymphoma that presented with soft lesions.[11]
ES is a recently developed US technique enabling the evaluation of tissue stiffness. The American College of Radiology includes elasticity assessment in the fifth edition of Ultrasonographic Breast Imaging Reporting and Data System (BI-RADS US).[12] Recently, there is an increasing number of studies assessing the role of ES in detecting breast malignancies, especially primary breast carcinoma.[13141516] In addition, ES has been shown to provide additional information in differentiating between benign and malignant breast lesions, and determining biopsy. Strain and Shear Wave ES are two different ES techniques. It has been reported that Shear Wave ES is a more objective method than strain ES. Shear wave ES enables quantitative measurement of tissue stiffness.[17] In this study, we aimed to analyze B-mode US and ES findings of patients with clinical outcomes.
MATERIALS AND METHODS
Our Institutional Review Board approved this retrospective study and waived the informed consent. We searched all core-needle biopsy results performed at our breast center between the dates of January 2013 and September 2016. Our search revealed 9 patients having breast involvement due to hematological malignancies. All the diagnoses were confirmed using US-guided core-needle biopsy. One patient had strain ES and 8 patients had Shear Wave ES images. B-mode US imaging findings and ES findings were analyzed. In addition, clinical outcomes of the patients were noted.
Real-time whole B-mode breast US examinations and ES were performed on all patients using ES or Shear-Wave ES. We used two US systems (Acuson S 2000, Siemens, Erlangen, Germany) one of which only enables strain ES and the second enables Shear-Wave ES. A linear transducer that enables scanning with a frequency range of 4 − 9MHz was used. Two radiologists reviewed the cases at the same time on consensus and conferred on every case. There was a case report form, and the radiologists were requested to decide the pattern of the infiltration (diffuse, solitary or multiple mass), determine the BI-RADS categorization of the mass, and describe both US and ES findings together. The elasticity assessments were done by general impression of color-coded maps, quantitative values (including strain ratio), and Shear-Wave Velocity (SWV). Virtual touch imaging (VTI) maps were also used when available.
Statistical analysis was performed using the statistical package SPSS software (version 17.0, SPSS Inc., IL, USA). If continuous variables were normal, they were described as mean ± standard deviation (P > 0.05 in Kolmogorov–Smirnov test or Shapira–Wilk [n < 30]), and if they were not normal, they were described as the median.
RESULTS
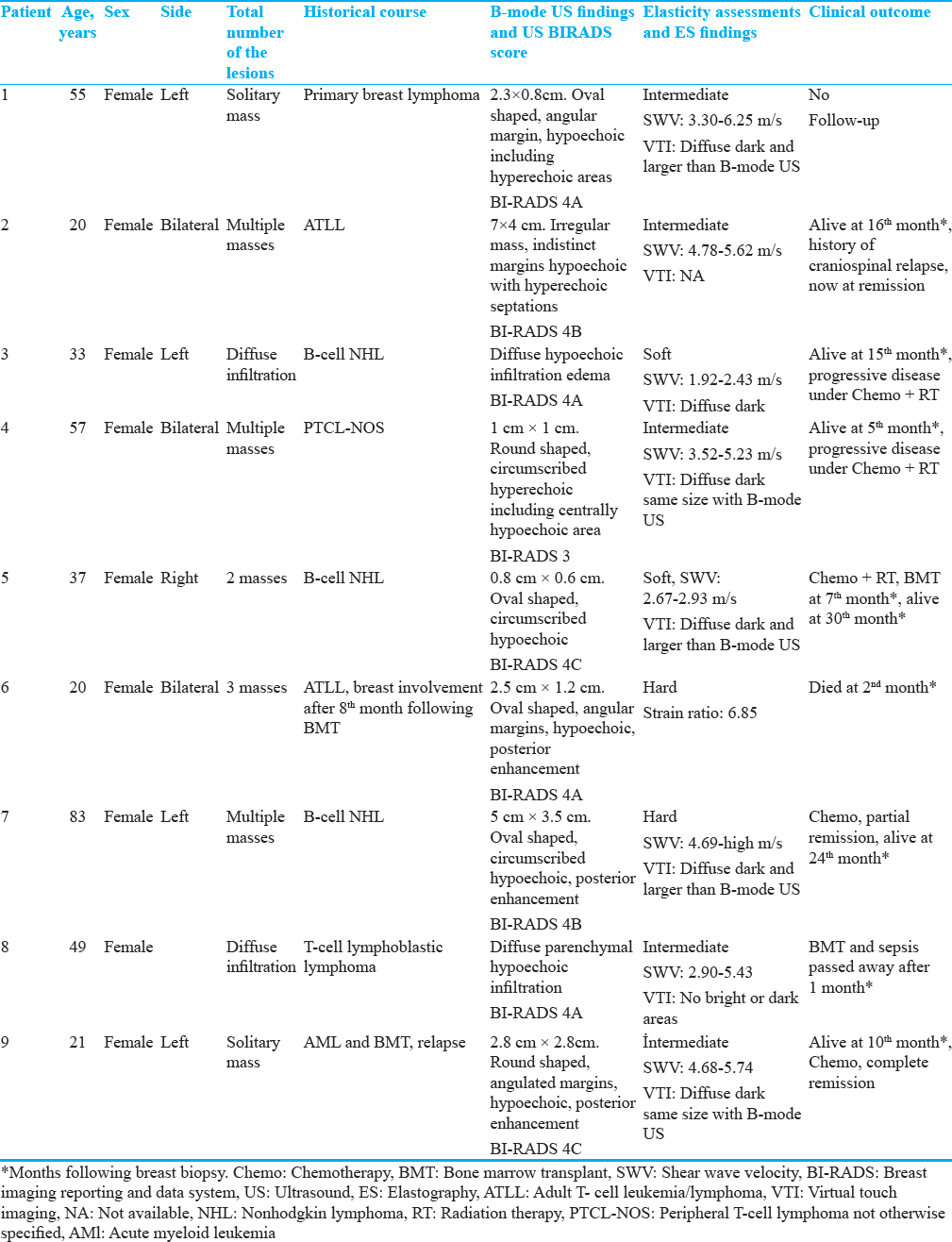
Patient characteristics, B-mode US, and ES findings and clinical outcomes are summarized in Table 1. The mean age of the study population was 46.6 years (range, 20–83 years). All patients were female. One patient had primary breast lymphoma whereas eight of the patients had secondary involvement of breast with leukemia or lymphoma. B-mode US images were available for all patients. One patient was examined using strain ES and 8 patients were examined using Shear-Wave ES. Three patients had bilateral, and 6 patients had unilateral involvement. None of the lesions had calcifications. Two patients had diffuse infiltration and 7 patients had mass lesions.
Diffuse infiltration (n = 2)
Two patients that had diffused parenchymal infiltration had similar B-mode US findings including diffuse hypoechoic finger-like infiltration of the normal breast parenchyma [Figure 1]. One patient had bilateral diffuse and one had left-sided diffuse parenchymal infiltration. One of these patients had accompanying skin edema that can be detected through US. These infiltrations had no posterior acoustic features. The elasticity assessments of these lesions were soft and intermediate. The patients with diffuse infiltration of the breast had a poor prognosis. One of them had already passed away, and the other had a progressive disease that was being treated.
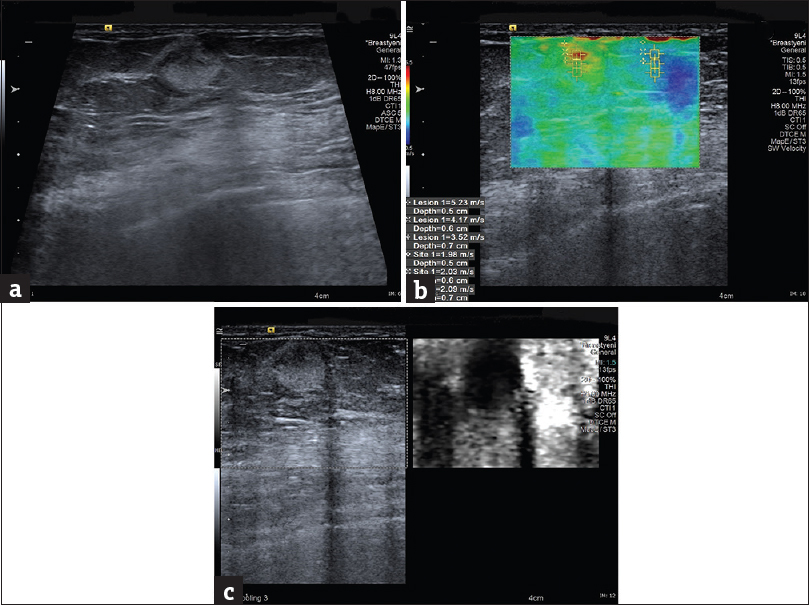
- 57 year's old female with a diagnosis of peripheral T-cell lymphoma not otherwise specified (a) B-mode Ultrasound showed a well-circumscribed round shaped hyperechoic lesion including centrally hypoechoic areas within the mass. (b) Shear Wave elastography demonstrates Shear Wave velocities from 3.52 to 5.23 m/s within the mass. (c) Virtual Touch Imaging method demonstrates diffuse dark lesion with same size as B-mode ultrasound.
Mass lesions (n = 7)
The size of the tumors varied from 0.8 to 7.0 cm, which was the largest diameter (median, 2.5 cm.). Two patients had a unilateral solitary mass. Five patients had more than one lesion, either unilateral or bilateral. Three of these seven masses had circumscribed, and the remaining 4 had uncircumscribed margins [Figure 2]. The BI-RADs scores of the patients were as follows: BIRADS 3 (n = 1), BIRADS 4A (n = 2), BIRADS 4B (n = 2), and BIRADS 4C (n = 2). The elasticity assessments of the patients were as follows: soft (n = 1), intermediate (n = 4), high (n = 2). SWVs are summarized in Table 1. Five of these patients were examined by grayscale VTI maps. VTI maps showed that, in 3 of these lesions, the lesion was diffuse dark and larger than B-mode. Using VTI, two patients were found to have diffuse dark lesions, that were on the same size compared with B-mode US.
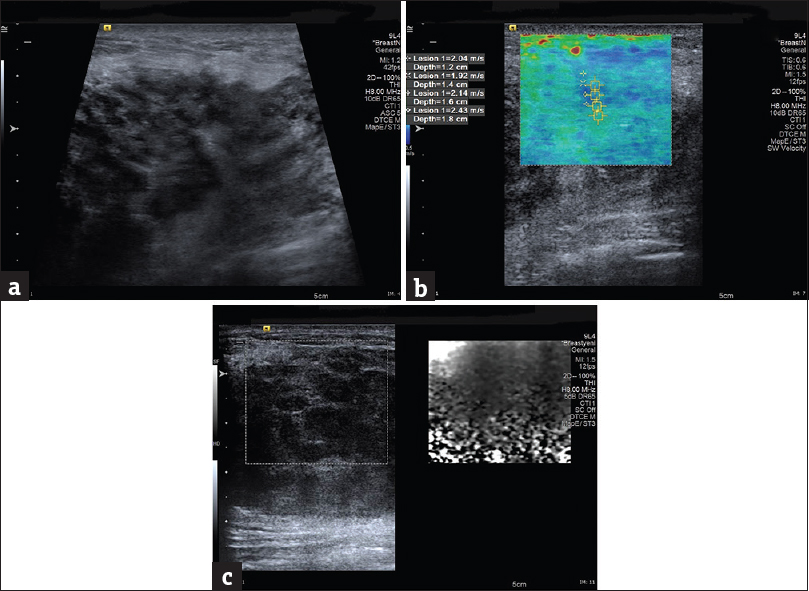
- 33 year's old female with a diagnosis of non-Hodgkin lymphoma. (a) B-mode ultrasound shows diffuse hypoechoic infiltration of the normal breast parenchyma. (b) Shear Wave elastography demonstrates Shear Wave velocities from 1.92 to 2.43 m/s. (c) Virtual touch imaging method demonstrates diffuse dark lesion.
DISCUSSION
Breast manifestations of hematological malignancies are rare.[3] Radiologic features of breast leukemia and lymphoma have been reported only sporadically through case reports and have been nonspecific.[12] Mammography reveals masses and architectural distortions. US shows mainly hypoechoic, microlobulated, or indistinct masses. MRI showed nonspecific imaging findings, including single or multiple enhancing masses or nonmass like enhancing lesions, and restricted diffusion.[4578]
A prior history of hematological malignancies may be helpful in diagnosing secondary breast lesions; however, the breast manifestation may be the initial diagnosis of systemic diseases.[18] Another reason to differentiate primary breast cancer from hematological involvement among the patients with hematological malignancies is because it affects both treatment and clinical outcome of the disease.
The purpose of this article is to describe the US and ES findings of hematological malignancies of the breast and assess the correlations between imaging findings and clinical outcomes.
In our study population, both lymphoma and leukemia demonstrated diffuse parenchymal infiltration. On the other hand, mass lesions were more common than diffuse parenchymal involvement among our study population. Mass lesions showed both circumscribed and uncircumscribed margins. The hypoechoic echo pattern was the most common echo pattern. Mass lesions manifested as either a solitary mass or multiple masses. In general, higher strain ratios and SWVs suggested malignant lesions in the breast. In our study, mass lesions showed elasticity assessments from soft to high. High elasticity scores may alert us to further investigate the lesions. In the literature, different cutoff SWVs-ranging from 4.1 to 5.2 m/s-were reported to differentiate malignant lesions from benign ones.[10192021] However, the potential risk is the lesions with low elasticity assessments. Previously reported studies showed the potential role of quantitative and qualitative ES in affecting the BI-RADS score.[2223] In our study, only one patient was categorized as having BI-RADS 3; however, the majority of the patients were considered as having BI-RADS 4 lesions.
Although the follow-up period of the patients was short, the prognosis seemed to be poor with breast involvement by hematological malignancies. Both soft and hard lesions showed poor prognosis, so the prognosis appeared to be poor regardless of elasticity scores. ES findings may not be a predictive value in assessing the treatment response or survival rate. Previously, regarding breast involvement with lymphoma, it was reported that the prognosis appeared to be mainly related to age, stage of the disease, and the histological type of the disease.[24]
The limitations of the current study were the relatively limited number of patients, the nonblinded image evaluation, and the retrospective nature of the study. Short-term follow-up is another limitation.
CONCLUSIONS
We reported 9 patients with breast involvement due to lymphoma and leukemia. Both B-mode US and ES showed various imaging findings. It is important to consider that both lymphoma and leukemia may show soft or intermediate elasticity assessment. In this regard, the patients’ history and clinical background cause us to consider breast involvement in leukemia and lymphoma patients. It appears that there was no correlation between the elasticity assessment and clinical outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2017/7/1/42/219453
REFERENCES
- Lymphoma affecting the breast: A pictorial review of multimodal imaging findings. J Breast Cancer. 2013;16:254-65.
- [Google Scholar]
- MR imaging of malignant primary breast lymphoma: Including diffusion-weighted imaging, histologic features, and a literature review. Jpn J Radiol. 2013;31:668-76.
- [Google Scholar]
- The discrepancy between the radiological findings and clinical signs should suggest the possibility of a lymphoproliferative lesion.’Mammographic appearance of malignant lymphoma of the breast. Radiology. 1980;135:623-6.
- [Google Scholar]
- Magnetic resonance imaging features of breast leukemia. Magn Reson Med Sci. 2013;12:309-13.
- [Google Scholar]
- Multicentric granulocytic sarcoma of the breast: Mammographic, sonographic, and MR findings. Clin Imaging. 2006;30:271-4.
- [Google Scholar]
- Primary non-Hodgkin lymphoma of the breast: Ultrasonography, elastography, digital mammography, contrast-enhanced digital mammography, and pathology findings. Ultrasound Q. 2015;31:279-82.
- [Google Scholar]
- Shear-wave elastography of the breast: Value of a quality measure and comparison with strain elastography. Radiology. 2015;275:45-53.
- [Google Scholar]
- ACR BI-RADSR ultrasound. In: ACR BI-RADS®. Atlas, Reston, VA: Breast Imaging Reporting and Data System, American College of Radiology; 2013.
- [Google Scholar]
- Shear-wave elastography and greyscale assessment of palpable probably benign masses: Is biopsy always required? Br J Radiol. 2016;89:20150865.
- [Google Scholar]
- Elastography by acoustic radiation force impulse technology for differentiation of benign and malignant breast lesions: A meta-analysis. J Med Ultrason (2001). 2016;43:47-55.
- [Google Scholar]
- Added value of shear-wave elastography for evaluation of breast masses detected with screening US imaging. Radiology. 2014;273:61-9.
- [Google Scholar]
- Use of shear wave elastography to differentiate benign and malignant breast lesions. Diagn Interv Radiol. 2014;20:239-44.
- [Google Scholar]
- Non-Hodgkin lymphoma of the breast: Imaging characteristics and correlation with histopathologic findings. Radiology. 1994;192:157-60.
- [Google Scholar]
- Shear-wave elastography improves the specificity of breast US: The BE1 multinational study of 939 masses. Radiology. 2012;262:435-49.
- [Google Scholar]
- Clinical application of shear wave elastography (SWE) in the diagnosis of benign and malignant breast diseases. Breast Cancer Res Treat. 2011;129:89-97.
- [Google Scholar]
- Quantitative shear wave ultrasound elastography: Initial experience in solid breast masses. Breast Cancer Res. 2010;12:R104.
- [Google Scholar]
- Diagnostic value of commercially available shear-wave elastography for breast cancers: Integration into BI-RADS classification with subcategories of category 4. Eur Radiol. 2013;23:2695-704.
- [Google Scholar]
- ShearWave™ Elastography BE1 multinational breast study: Additional SWE™ features support potential to downgrade BI-RADS®-3 lesions. Ultraschall Med. 2013;34:254-9.
- [Google Scholar]
- Primary non-Hodgkin malignant lymphoma of the breast. An immunohistochemical study of seven patients and literature review of 152 patients with breast lymphoma in Japan. Cancer. 1992;70:2451-9.
- [Google Scholar]




