
Translate this page into:
An Unusual Case of Gallium Scan Mimicking a Bone Scan
Address for correspondence: Dr. Ameya Puranik, 6, Amber Palace Apts, Chittaranjan Road, Vile Parle (E), Mumbai – 400 057, India. E-mail: adpuranik@hotmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Gallium-67 localization is based on the fact that it binds to plasma proteins like transferrin and lactoferrin, which have iron-binding sites. Abnormal biodistribution of gallium-67 citrate can occur in iron-overload states. We report one such case of gallium scan mimicking a bone scan due to skeletal uptake of gallium.
Keywords
Bone scan
gallium scan
transfusion

INTRODUCTION

Gallium-67 (Ga-67) citrate is a nonspecific inflammation imaging agent. Various disease states and medications can alter iron levels in the body, and hence affect Ga-67 binding.[1] We report a case of pyrexia of unknown origin where abnormal biodistribution of Ga-67 in the skeleton was observed.
CASE REPORT
A 23-year-old young male, with pyrexia of unknown origin, was referred to our department for a whole body Gallium scan, in order to detect the primary disease focus. The patient had a history of high-grade continuous fever for the past month and no other complaints. Routine hemogram showed low hemoglobin levels (6.6 gram percent). He received five blood transfusions over 48 hours. This resulted in increased hemoglobin level of 9.2 gram percent on the day of the gallium scan. Blood culture, urine and stool examinations revealed no abnormal finding. Posteroanterior chest radiograph was normal. Gallium scan was acquired at 24 hours after an intravenous injection of 5 mCi of Ga-67 citrate. Simultaneous anterior and posterior images were acquired on a Dual Head GE Infinia Hawkeye Single Photon Emission Computed Tomogaphy/Computed Tomography (SPECT/CT) scanner, using a medium energy collimator using 20% energy windows set at 93, 184, 297 keV photopeaks. Whole body images were acquired for 1,00,000 counts anteriorly and posteriorly. These images [Figures 1a and 1b] revealed diffuse tracer uptake in the skeleton with no uptake at normal physiological sites. There was a focus of uptake in the region of left kidney [Figure 1a -arrow]. This was identical to a whole body 99m Tc Methylene Diphosphonate (MDP) bone scan. However, transaxial SPECT CT images of the abdomen [Figure 1c - axial CT, 1d - fused images] revealed that the focus corresponded to bowel activity. A detailed review of history and mechanism of distribution of Ga-67, suggested that the skeletal uptake of gallium was due to iron overload following blood transfusions.
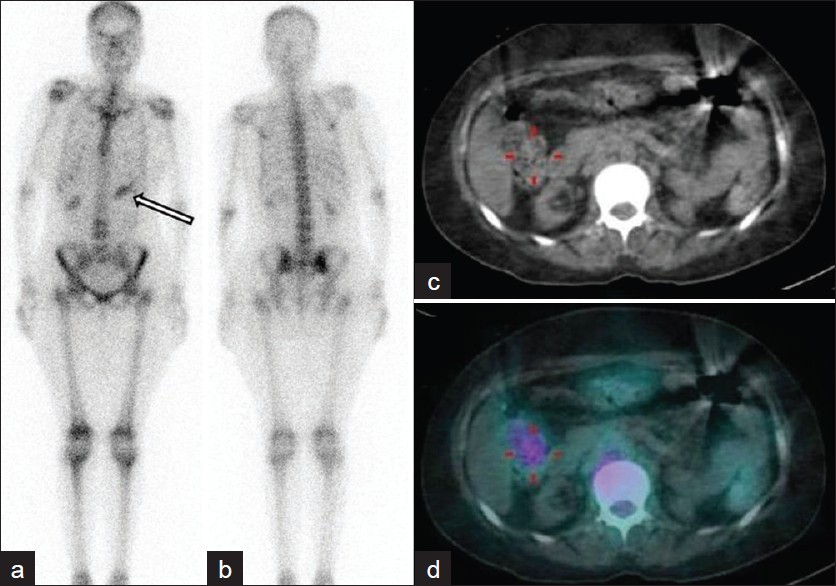
- Whole body gallium scintigraphy (a) anterior and (b) posterior images show diffuse skeletal tracer uptake. Focal tracer uptake seen in the region of left kidney on anterior images (arrow). (c) Axial CT image shows focal tracer uptake corresponding to bowel uptake of gallium, better appreciated on (d) fused SPECT CT image.
DISCUSSION
The primary uptake mechanism involves a carrier-mediated transport system, with Ga-67 binding to transferrin, to cross-cell membranes. Following entry into the cell, Ga-67 binds to other iron binding complexes, mainly lactoferrin and transferrin.[2] Normal biodistribution of gallium is seen in liver (highest uptake), spleen, salivary glands, nasopharynx, lacrimal glands, breast (in pregnant and lactating women), lungs (diffuse uptake upto 24 hours), kidneys and bladder (route of excretion in first 24 hours) and colon (route of excretion after 24 hours). In the given scenario, multiple blood transfusions led to an iron-overload state, thereby resulting in saturation of binding capacity of serum transferrin.[3] As a result, there is no Gallium uptake at physiological sites expressing transferrin receptors. This results in increased bone uptake of tracer resulting in a gallium scan mimicking a whole body bone scan. Similar situation is encountered in patients post chemotherapy or post-G–CSF (Granulocyte-Colony Stimulating Factor) administration; however, the diffuse uptake is due to marrow hyperstimulation.[4] There are similar reports in literature highlighting the diffuse uptake of Ga-67 in the bones.[5] This case is another one showing similar findings. Moreover, it once again highlights the importance of knowing the detailed history of the patient and adequate patient preparation, prior to any diagnostic procedure. Detailed history is important in scintigraphic procedures, since a lot of drugs and biological products interfere with the binding of the tracer due to saturation of the receptor sites, thereby reducing the tracer uptake or altering the normal pathway of biodistribution, as seen in our case.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/16/95430
REFERENCES
- Modification of distribution of Ga-67 in man by administration of iron. Br J Radiol. 1980;53:563-71.
- [Google Scholar]
- Altered 67Ga citrate distribution in patients with multiple red blood cell transfusions. AJR Am J Roentgenol. 1982;139:755-9.
- [Google Scholar]
- Diffuse bone increase uptake of gallium-67 related to cyclophosphamide and recombinant human granulocyte-colony stimulating factor (rHuG-CSF) administration. Nuklearmedizin. 2000;39:78-80.
- [Google Scholar]
- A generalized increase in uptake of gallium-67 in bone. Semin Nucl Med. 1984;14:143-5.
- [Google Scholar]




