
Translate this page into:
Multiple Mycotic Aneurysms of the Abdominal Aorta Illustrated on MDCT Scanner
Address for correspondence: Dr. Amit Nandan Dhar Dwivedi, Department of Radiodiagnosis and Imaging, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, Uttar Pradesh, India. E-mail: amitnandan21@yahoo.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Infective mycotic aneurysm of the aorta is a rare and life-threatening disease. A patient presenting with constitutional symptoms and pulsatile abdominal mass should raise a suspicion of mycotic aneurysm. Early detection of aortic mycotic lesions in such patients should play a key role in the treatment of aortic aneurysms. Multiple mycotic aneurysms of abdominal aorta in a young male are a rare manifestation of the disease. Multidetector computerized tomography (CT) is an essential tool in identifying the etiology, pathogenesis, protean manifestations of systemic tuberculosis, and ultimately deciding the course of treatment.
Keywords
Abdominal aorta
multidetector computerized tomography
mycotic aneurysm
systemic tuberculosis


INTRODUCTION
Osler first used the term “mycotic aneurysm” in 1885 to describe a mushroom-shaped aneurysm in a patient with subacute bacterial endocarditis. This may create considerable confusion, since “mycotic” is typically used to define fungal infections. However, mycotic aneurysm is still used for all extracardiac or intracardiac aneurysms caused by infections, except for syphilitic aortitis.[1] The term “infected aneurysm,” proposed by Jarrett and associates,[2] is more appropriate, since few infections involve fungi. Staphylococcus and Streptococcus species are the most common causes of infected aneurysms. Mycobacterium and fungi, such as Candida albicans and Aspergillus, are rare causes of infected aneurysms and only few cases of such multiple chronic granulomatous mycotic abdominal aorta aneurysms have been reported as per our literature search.[34] Clinical diagnosis of mycotic abdominal aneurysms is difficult. Depending on the location, mycotic aortic aneurysm usually manifests as abdominal pain with or without a pulsatile mass,[5] causing aneurysmal mass effect, chest pain, dysphagia, hoarseness, and the complications include fistula, perforations, bleeding, and rupture. Multidetector computerized tomography (CT) angiography allows early detection and characterization of abdominal aortic aneurysms. Identifying the underlying etiology is important in deciding the appropriate management of the aneurysm.
CASE REPORT
A 28-year-old Indian male with chronic weakness, loss of appetite, and a pulsatile mass in the abdomen was referred to our department for radiological evaluation. The patient was normotensive, non-smoker, non-diabetic, and was admitted for alteration of his general state, including weight loss, dizziness, and mild fever (38°C) for past 1 month. Laboratory evaluation evidenced elevated white cell count [20,000 per cubic mm (normal 3000–11,000)] and C-reactive protein (CRP). Tuberculin skin test was positive. Blood culture result was negative for Staphylococcus and Streptococcus species, Salmonella, Gram-negative bacteria, such as Escherichia coli, Klebsiella, and Pseudomonas mycobacterium, and fungi, such as C. albicans and Aspergillus. The patient had no history of tuberculosis or any previous intravascular procedure. Abdominal ultrasound (USG) showed mild hepatosplenomegaly and multiple significantly enlarged, heterogeneous, necrotic, conglomerate retroperitoneal lymph nodes including periportal and peripancreatic nodes. Color flow Doppler examination demonstrated multiple variable-sized aneurysms of abdominal aorta with pulsatile flow in the center and thrombus at the periphery. A CT angiography of whole abdomen was performed and the images were evaluated using multiplanar reconstruction and 3D volume rendering techniques. The CT angiography revealed multiple saccular aneurysms with thin irregular walls, arising from the abdominal aorta [Figures 1 and 2]. Two aneurysms were seen, one at suprarenal aorta and measuring 5.2 × 2.5 cm and the other involving infrarenal abdominal aorta and measuring 4.5 × 4 cm. One of the aneurysms was causing near-total compression of right renal artery, resulting in chronic renal parenchymal changes secondary to ischemia [Figure 3]. Multiple enlarged (largest 2.8 cm in short-axis dimension) para-aortic lymph nodes were identified in the vicinity of the aneurysms showing evidence of internal necrosis [Figure 4]. No evidence of any abnormally enhancing mass lesion or bowel wall thickening could be identified. Screening of thorax for aneurysms was unremarkable. A USG-guided core biopsy of the retroperitoneal (pre-para aortic) lymph node was performed. The lymph node biopsy revealed central caseous necrotic material with epithelioid cells and macrophages consistent with tubercular etiology [Figure 5]. Based on the biopsy results, a presumptive diagnosis of tubercular aneurysm was made, and the patient was put on anti-tubercular treatment and advised surgical management of abdominal aortic aneurysms. On follow-up, the patient responded well to the anti-tubercular drug therapy, as there was reduction in the size of the retroperitoneal lymph nodes including pre-para aortic and peripancreatic nodes, as compared to previous pre-treatment scans. Post anti-tuberculosis treatment, the patient was advised open surgical/endovascular stenting procedures.

- 28-year-old male presenting with nonspecific symptoms of abdominal pain weakness and pulsatile abdominal mass on examination later diagnosed with mycotic abdominal aneurysm underwent computerized tomography angiography (CTA) of abdomen. 3D reconstructed image shows two large saccular aneurysms (arrows) arising from the abdominal aorta, one arising anteriorly and the other arising posteriorly.

- 28-year-old male presenting with nonspecific symptoms of abdominal pain weakness and pulsatile abdominal mass on examination later diagnosed with mycotic abdominal aneurysm underwent computerized tomography angiography of abdomen. Maximum intensity projection reformatted image in sagittal plane of abdomen shows two abdominal aortic saccular aneurysms (arrows).

- 28-year-old male presenting with nonspecific symptoms of abdominal pain weakness and pulsatile abdominal mass on examination later diagnosed with mycotic abdominal aneurysm underwent computerized tomography angiography of abdomen. CECT abdomen with maximum intensity projection reformatted image in axial plane shows pre-para aortic necrotic lymphadenopathy (white straight arrow) compressing right renal artery at its origin, thus causing chronic renal parenchymal changes on the right side (white arrowhead).

- 28-year-old male presenting with nonspecific symptoms of abdominal pain weakness and pulsatile abdominal mass on examination later diagnosed with mycotic abdominal aneurysm underwent computerized tomography angiography of abdomen. Contrast-enhanced CT axial section of abdomen shows enlarged para-aortic lymph nodes (arrowhead) in the vicinity of aneurysm (black arrow).
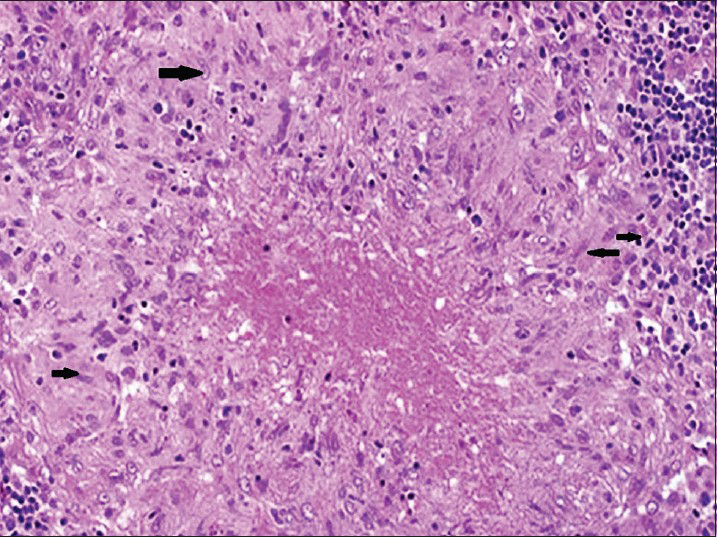
- 28-year-old male presenting with nonspecific symptoms of abdominal pain weakness and pulsatile abdominal mass on examination later diagnosed with mycotic abdominal aneurysm underwent computerized tomography angiography of abdomen. Microphotograph of core biopsy specimen from the retroperitoneal lymph node (hematoxylin and eosin, ×400 magnification) shows caseous necrosis with surrounding epithelioid cells (modified macrophages, black arrows), suggesting a tubercular etiology.
DISCUSSION
Infected aneurysm (or mycotic aneurysm) is defined as an infectious break in the wall of an artery with formation of a blind, saccular out-pouching that is contiguous with the arterial lumen.[6] The aorta is the most commonly involved artery and can be involved either by hematogenous diffusion or extension from a contiguous focus, either direct or indirectly via the lymphatic, such as lymph node, or a nearby infectious lesion. Mycotic aneurysm secondary to chronic granulomatous infection of the aorta is a rare and life-threatening disease. Depending on the location, infective aortic aneurysm usually manifests as abdominal pain with or without a pulsatile mass causing aneurysmal mass effect, chest pain, dysphagia, hoarseness, and the complications include fistula, perforations, bleeding, and rupture. This patient discussed here presented with a 1 month history of non-specific constitutional symptoms and signs of chronic infection like fever, weight loss, loss of appetite, and abdominal pain. In our case, based on the histopathology of the retroperitoneal lymph node, we made a presumptive diagnosis of tubercular abdominal aortic aneurysms. Blood culture result was negative for Mycobacterium, and it has been reported in the literature that sterile blood cultures occur in 18–50% of patients with infected aneurysms.[789] We reviewed all the cases of mycotic aneurysms reported in the English language scientific literature from 1945 till date. So far, a total of 39 cases have been published in the literature. A patient presenting with constitutional symptoms and pulsatile abdominal mass should raise a suspicion of infective mycotic aneurysm. Multidetector CT angiography is the imaging modality of choice for the detection and characterization of infected aneurysms. The imaging features of infected aneurysms of the aorta vary from the typical features of atherosclerotic aneurysms in both pattern of involvement and location of aneurysms. Early changes of aortitis preceding aneurysmal formation include an irregularly thickened arterial wall, peri-aortic edema, and a peri-aortic soft tissue mass. Tubercular abdominal aortic aneurysms are of saccular type having multilobulated appearance with thickened, hazy, and interrupted wall, along with adjacent necrotic lymphadenopathy and vertebral erosions.[10] The other differential diagnoses include aneurysms secondary to cystic medial necrosis and lymphomas due to other malignant retroperitoneal infiltrative lymph nodal masses. The specific management of an infected aneurysm must be individualized and is dependent on the characteristics of the aneurysm (location, morphology, and presence and extent of hemorrhage), patient characteristics, and available expertise. Therapeutic options include open surgery, endovascular stent placement, endovascular embolization, medical therapy, or a combination of these. In general, small, asymptomatic, and unruptured infected aneurysms can be managed with a trial of intravenous antibiotics for 4–6 weeks along with surveillance imaging. Our patient was put on anti-tubercular drug therapy for 9 months and on follow-up, the patient responded well to drug therapy as there was reduction in the size of the retroperitoneal lymph nodes compared to the previous pre-treatment scans. Following drug therapy, the patient underwent endovascular stenting procedure and is doing well at present without any postoperative complications. Large, ruptured, or symptomatic infected aneurysms require emergent or urgent open surgery in combination with antibiotic therapy. Infected aneurysms show a mixed response to medical therapy, and there are no predictive imaging features. They can undergo complete thrombosis, decrease in size, or enlarge, or new infected aneurysms can develop. Enlarging or residual aneurysms at surveillance imaging are triaged to surgical management. Newer endovascular techniques remain controversial because the introduction of a foreign body within an infected field is against general surgical principles. Worldwide, the incidence of tuberculosis is increasing with cases reported from the western world due to its association with Acquired Immunodeficiency Disease/Human Immunodeficiency Virus (HIV) infection. Early detection of aortic tubercular lesions in patients should play a key role in the efficiency of tubercular aortic aneurysm treatment. Tuberculosis is a common disease in developing countries and can affect any organ system, with unusual features and systemic manifestations.
CONCLUSION
Tuberculosis is endemic in developing countries and its incidence has also increased in the western world, especially among patients with HIV infection. This case report presents a case of multiple mycotic aneurysms of abdominal aorta of tubercular etiology in a young male to highlight the unusual manifestations of systemic tuberculosis. Multidetector CT is an essential tool in identifying the etiology, pathogenesis, protean manifestations of systemic tuberculosis, and ultimately deciding the course of treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2015/5/1/49/163993
REFERENCES
- Endocarditis and intravascular infections. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases (5th ed). Philadelphia: Churchill Livingstone; 2000. p. :888-92.
- [Google Scholar]
- Experience with infected aneurysms of the abdominal aorta. Arch Surg. 1975;110:1281-6.
- [Google Scholar]
- Tuberculous aneurysm of the aorta presenting with uncontrolled hypertension. J Vasc Interv Radiol. 2001;12:521-3.
- [Google Scholar]
- Infected aortic aneurysms: Aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001;34:900-8.
- [Google Scholar]
- Protean manifestations of mycotic aneurysms. AJR Am J Roentgenol. 1978;131:1019-25.
- [Google Scholar]
- Association Universitaire de Recherche en Chirurgie (AURC). Infected aneurysms of neck and limb arteries: A retrospective multicenter study. Ann Vasc Surg. 2001;15:197-205.
- [Google Scholar]
- Bacteriologic and surgical determinants of survival in patients with mycotic aneurysms. J Vasc Surg. 1984;1:541-7.
- [Google Scholar]




