
Translate this page into:
A Rare Cause of Acute Abdomen: Jejunal Diverticulosis with Perforation
Address for correspondence: Dr. Ibrahim Aydin, Department of Surgery, School of Medicine, Recep Tayyip Erdogan, University, Rize - 53100, Turkey. E-mail: ibrahimaydn@msn.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Jejunal diverticulosis is generally asymptomatic and is associated with high morbidity and mortality secondary to complications, especially in elderly patients. We present a case report of a 74-year-old female patient with jejunal diverticulosis and perforation due to diverticulitis.
Keywords
Acute abdomen
diverticulosis
jejunal diverticulitis
perforation


INTRODUCTION
Jejunal diverticulosis is generally seen in elderly patients, and it is relatively rare. Jejunal diverticula are generally asymptomatic, as a result, are usually only incidentally detected. Jejunal diverticulosis is associated with small bowel obstruction, bleeding, or perforation. We present a case report of a 74-year-old female who presented with jejunal diverticular perforation.
CASE REPORT
A 74-year-old female patient was admitted to the Emergency Room with sudden onset of abdominal pain, nausea, and vomiting. Her physical examination revealed diffuse abdominal tenderness and abdominal rebound tenderness. Her laboratory tests were normal, except for elevated white blood cell count (WBC 13200/mm≥). Abdominal X-ray image in upright position showed two gas fluid lesions in the small intestine [Figure 1]. A computed tomography (CT) scan with intravenous (IV) contrast revealed multiple diverticula on the mesenteric wall of the small intestine and dilated intestinal loops proximal to the diverticula, but no free air or fluid [Figure 2]. Due to the acute symptoms, exploratory laparotomy surgery was performed. Multiple diverticula were seen located between 40th and 100th cm distal to the ligament of Treitz. A necrotic, perforated diverticulum was present in the distal part of the jejunal segment [Figure 3]. The 60-cm long jejunal segment was excised and end-to-end anastomosis was performed. The patient did not experience any postoperative complications, recovered completely and was discharged on Day 7. Histopathological examination showed multiple diverticula on the small intestinal wall closer to the mesenteric side as well as necrosis and a 5-mm perforation hole on one of the diverticula. The area of perforation was filled with fibrinous exudate. The diverticula were false diverticula, and only the mucosa and submucosa were herniated.
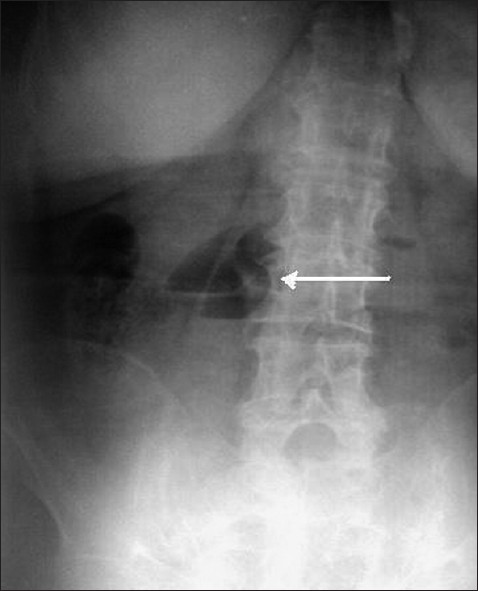
- 74-year-old female patient with sudden onset of abdominal pain, nausea, and vomiting diagnosed with jejunal diverticulosis and perforation. Upright abdominal X-ray image shows small bowel obstruction and air-fluid area (arrow).
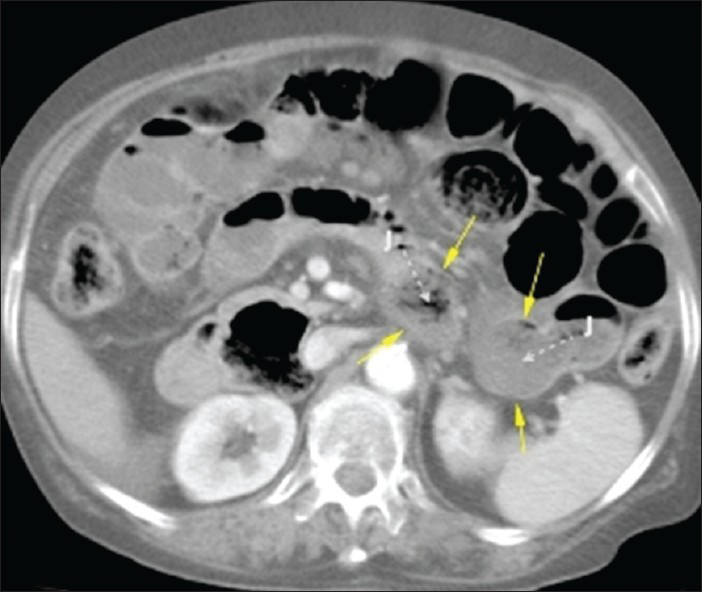
- 74-year-old female patient with sudden onset of abdominal pain, nausea, and vomiting diagnosed with jejunal diverticulosis and perforation. Contrast-enhanced abdominal CT image shows two jejunal diverticula (arrows). Direction of the diverticula from their origin is shown with dashed white arrows (J: Jejunum).
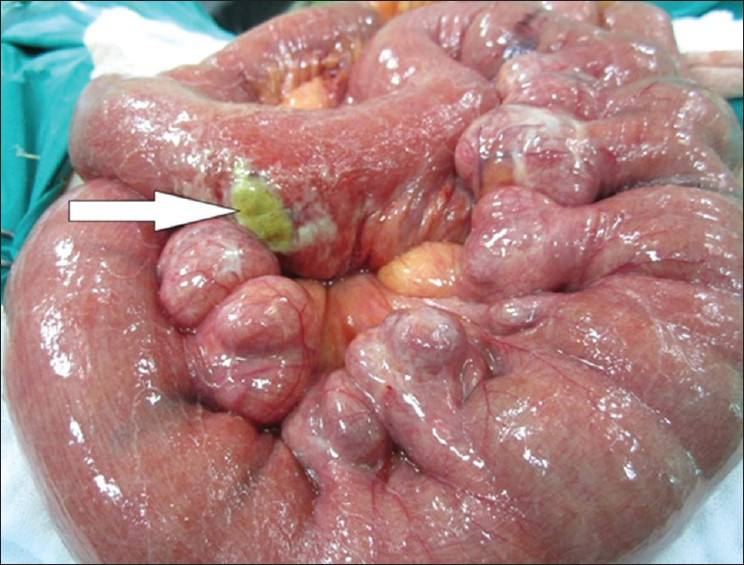
- 74-year-old female patient with sudden onset of abdominal pain, nausea, and vomiting diagnosed with jejunal diverticulosis and perforation. Photograph taken during abdominal exploration, shows multiple diverticula on the mesenteric side of the jejunum, and a perforation hole due to necrosis on one of the di verticula in the distal part (arrow).
DISCUSSION
Jejunal diverticulosis is a rare condition, with a reported incidence rate of 0.1-1.5%.[1] The diverticula are generally seen in elderly patients and are false pulsion diverticula, containing only mucosal and submucosal layers. Diverticula are formed due to an increase in pressure inside the lumen at the entrance to the mesenteric vessels where the wall is weaker.[2] Our case was an elderly patient, and the diverticula were located at the entrance of the mesenteric vessels; this is consistent with previous reports in the literature.[12]
Seventy-five percent of the diverticula in the small intestine are located in the proximal jejunum, 20% in the distal jejunum, and 15% in the ileum.[3] Jejunal diverticula range in size from a few millimeters to 10 cm. In the present case, the diverticula were located in the proximal jejunum, and the perforated diverticulum was approximately 3 cm in size.
The diverticula are generally asymptomatic. At times, the symptoms can be mild, such as chronic nonspecific abdominal pain, but they can also be life-threatening, such as malabsorption, diverticulitis, hemorrhage, obstruction, and perforation.[4] Acute necrotizing inflammation, trauma, and foreign bodies can cause diverticular perforation. The most important complications of diverticula, which require urgent surgery are perforation, massive gastrointestinal bleeding, and intestinal obstruction.[5] Perforation occurs in 2.3-6.4% of patients with jejunal diverticulosis.[6]
Our case had diverticular perforation due to necrosis and peritonitis as a result of the perforation. In cases of perforation, free air under the diaphragm may not always be visible in chest X-rays. Although barium scan of the small intestine is one of the best radiological contrast study to visualize diverticula, it is contraindicated in case of perforation or acute diverticulitis to suggest a perforation.[7] Abdominal CT scans have been found to be helpful in the diagnosis of jejunal perforation.[8] Their importance in the diagnosis of abscess forming diseases (appendicitis, diverticulitis, and Crohn's disease) has gradually become more apparent.
The chest X-rays of our patient showed no sign of free air under the diaphragm, and diagnosis was based on the abdominal CT with IV contrast. Patients with perforated jejunal diverticulum often have localized or diffuse peritonitis. Novak et al., indicated that percutaneous drainage and IV antibiotic administration is sufficient for treatment of patients in stable condition with localized peritonitis.[9] However, for patients with symptoms of generalized peritonitis, emergency laparotomy and segmental intestinal resection is recommended.[10] Our case had multiple jejunal diverticula and peritonitis due to perforated diverticulum.
CONCLUSION
Jejunal diverticula is rare and mostly asymptomatic. Patients may have nonspecific symptoms, such as chronic abdominal pain and change in bowel habits. However, the morbidity and mortality rates may increase due to perforation, obstruction, and bleeding. If acute abdomen due to perforation is suspected, jejunal diverticulosis and diverticular perforation must be considered in the differential diagnosis.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/31/115763
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Nonmeckelian jejunal or ileal diverticulosis: An analysis of 112 cases. Surgery. 1994;116:726-32.
- [Google Scholar]
- Small intestine diverticula: Is there anything new? World J Gastrointest Surg. 2011;27:49-53.
- [Google Scholar]
- Giant and multiple jejunal diverticula presenting as peritonitis a significant challenging disorder. J Med Life. 2012;5:308-10.
- [Google Scholar]
- Small bowel diverticulosis: Perceptions and reality. J Am Coll Surg. 1997;184:383-8.
- [Google Scholar]
- Acquired jejunuileal diverticulosis and its complications: A rewiew of the literature. Am Surg. 2008;74:849-54.
- [Google Scholar]
- Jejunal diverticulae: Reports of two cases with review of literature. Indian J Surg. 2009;71:238-44.
- [Google Scholar]
- Jejunal diverticulosis: Findings on CT in 28 patients. AJR Am J Roentgenol. 2008;190:1286-90.
- [Google Scholar]
- Nonsurgical management of acute jejunal diverticulitis: A rewiew. Am J Gastroenterol. 1997;92:1929-31.
- [Google Scholar]
- Perforated jejunal diverticulitis: Personal experience and diagnostic with therapeutical considerations. Ann Ital Chir. 2000;71:95-8.
- [Google Scholar]




