
Translate this page into:
Retrograde Pyelogram during intended Cystogram: A Rare complication of a common procedure
Address for correspondence: Dr. Shanmugasundaram Rajaian, Department of Urology, MIOT Hospitals, 4/112, Mount Poonamallee Road, Chennai - 600 089, Tamil Nadu, India. E-mail: ssrl25@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Inadvertent placement of the urinary catheter into the ureter can cause several complications. We describe a rare complication during cystogram due to unrecognized inadvertently placed urinary catheter in ureter, resulting in a life-threatening situation. A 47-year-old multiparous female underwent total laparoscopic hysterectomy for adenomyosis. During early postoperative period, she developed vesicovaginal fistula and transvaginal repair of fistula was done. During filling cystography done at 2 weeks, she developed right loin pain and urosepsis. Contrast extravasation was seen in the right renal subcapsular space with Foley's catheter inside the right ureter. Subsequently, she recovered well.
Keywords
Cystogram
extravasation
sepsis
ureteric catheterization


INTRODUCTION
Inadvertent placement of the catheter into the ureter is rare. It can occur while placing the catheter both by per-urethral and suprapubic route. It can also occur due to inadvertent catheter migration after placement. It results in complications such as ureteric obstruction, ureteric rupture, and sepsis. We report a patient for whom acute extravasation of contrast and urosepsis occurred during cystogram due to inadvertent placement of the urinary catheter into the ureter.
CASE REPORT
A 47-year-old multiparous female presented with menorrhagia secondary to adenomyosis. She underwent total laparoscopic hysterectomy with bilateral salphingoopherectomy. On the 2nd postoperative period, she had continuous watery leakage per vaginally. Subsequent cystoscopy confirmed 4 mm size trigonal vesicovaginal fistula (VVF) and patulous right ureteric orifice. Transvaginal VVF repair with Martius flap interposition was done. She was discharged with the catheter, and to ascertain bladder healing, a cystogram was advised at 2 weeks. She had a static cystogram in another peripheral hospital and developed right loin pain, fever, and chills. With features of urosepsis, she was readmitted and resuscitated. Her blood and urine culture grew Escherichia Coli. Retrospective inspection of the plain X-ray of the kidney, ureter, and bladder (KUB) region showed the tip of the Foley's catheter on the right side of the pelvis well above the normal position [Panel a, Figure 1]. The presence of Foley's balloon in the dilated right ureter with contrast extravasation in the subcapsular region of the right kidney was noted [Panel b, Figure 1]. The Foley's catheter was deflated and repositioned under fluoroscopic guidance as the immediate measure. Subsequent plain computed tomography (CT) KUB revealed curvilinear right subcapsular collection of extravasated contrast [Panel a, Figure 2] and perinephric stranding with absence of periureteric extravasation [Panel b, Figure 2]. She was managed with intravenous antibiotics without the need for intervention in the intensive care unit; she recovered well and was discharged from the hospital. She was voiding well without any leakage of urine.
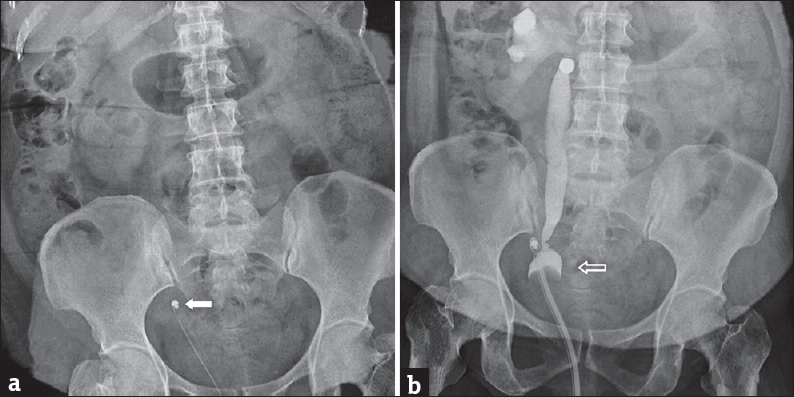
- A 47-year-old female underwent transvaginal repair for vesicovaginal fistula acquired after a hysterectomy. (a) Plain X-ray of kidney, ureter, and bladder region shows deviation of the tip of the Foley's catheter toward the right side pelvic wall (white solid arrow). (b) Filling cystogram showing the presence of inflated Foley's catheter (hollow white arrow) inside the lower part of the right ureter with pyelogram and extravasation of the contrast agent around the kidney.
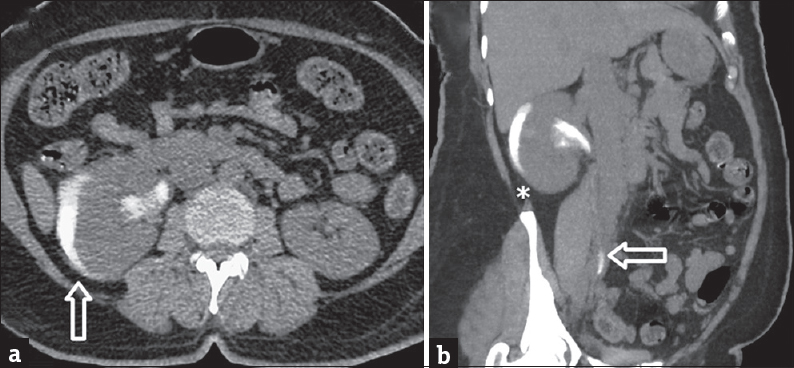
- A 47-year-old female underwent transvaginal repair for vesicovaginal fistula acquired after a hysterectomy. (a) Axial section of the plain computed tomography scan of kidney, ureter, and bladder region shows persistent subcapsular curvilinear crescentic contrast extravasation (vertical hollow white arrow) around the right kidney. (b) The coronal section shows right perinephric stranding (asterisk) and intact ureteric continuity (horizontal hollow white arrow).
DISCUSSION
Inadvertent placement of urinary catheters in ureters has been reported and known to cause complications such as obstruction,[1] ureteric rupture,[2] sepsis,[3] and tumefaction.[4] It often goes unrecognized till complications occurred as in our case. The patient may present with loin pain, lower abdominal pain, abdominal distension, pericatheter leak, and features of pyelonephritis. Usually, diagnosis is made during evaluation for high clinical suspicion of misplaced catheter denoted by symptoms such as obstructed drainage and decreased urine output. Ultrasound examination would be sufficient to assess the position of the catheter and the status of the ipsilateral renal unit. In our case, the daily urine output through the catheter was about 1.5–1.7 l a day. Hence, there was no suspicion of misplaced catheter and it was identified only during the cystogram. Cystograms are often done after reconstructive surgery of lower urinary tract to assess the integrity of the repair and to decide on time of catheter removal. Check cystogram is done in the following occasions: after partial cystectomy, orthotopic neobladder, bladder augmentation, anastomotic urethroplasty, radical prostatectomy, VVF repair, vesicourethral reflux surgery, and as a part of pretransplant evaluation. However, the need for doing routine cystograms has been questioned and is advised in selected cases only.[5] Patients with neurogenic bladder on long-term catheter change have contracted bladder and altered anatomy while vesicoureteric reflux patients have patulous ureteric orifice and hence more chances of wrong catheter placement.[1] Short-tip catheters can be used for regular catheter change in neurogenic bladder patients. If resources are available, bedside ultrasound can be used to confirm the catheter tip.[1] If there is suspicion of ureteric rupture, CT urography may be done to confirm the diagnosis. Partial ureteric injury can be managed with double J (DJ) stenting. Complete ureteric injury may require percutaneous nephrostomy (PCN) in the immediate setting and need for open repair in the future. A patient presenting with sepsis, if not resolving on antibiotics, needs diversion either by DJ stenting or PCN if there is hydronephrosis. This case is reported to reemphasize the importance of doing filling cystogram if needed, only with adopted precautions such as gravity filling of contrast under pulsed fluoroscopy and under vigilant care of a radiologist or urologist. Abnormal position of urethral catheter in scout X-ray film before cystogram might suggest the inadvertent placement of it into ureter as in our case. Careful repositioning of the catheter to its normal location under fluoroscopy is mandatory to avoid serious complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2018/8/1/55/247346
REFERENCES
- Inadvertent placement of a urinary catheter into the ureter: A report of 3 cases and review of the literature. Asian J Urol. 2017;4:256-61.
- [Google Scholar]
- Mid-ureteral rupture: A rare complication of urethral catheterization. Urology. 2012;80:e65-6.
- [Google Scholar]
- Obstructed kidney and sepsis secondary to urethral catheter misplacement into the distal ureter. BMJ Case Rep 2015 2015 pii: bcr2014207757
- [Google Scholar]
- Inadvertent insertion of a Foley's catheter through the orifice of a duplex ureter during catheterisation for laparotomy. Gynecol Surg. 2011;8:99.
- [Google Scholar]
- Selective indication for check cystogram before catheter removal following robot assisted radical prostatectomy. Indian J Urol. 2016;32:120-3.
- [Google Scholar]




