
Translate this page into:
Use of CBCT in the Successful Management of Endodontic Cases
Address for correspondence: Dr. Dax Abraham, E-144 East of kailash, New Delhi -110065, E-mail: daxsusan2105@yahoo.co.in
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The purpose of this article is to emphasize the use of Cone Beam Computed Tomography (CBCT) for root canal treatment. Two case reports are presented where CBCT has been used to locate and eventually treat extra canals in maxillary first molars. Dental clinicians should be aware of the anatomical variations in maxillary molars. CBCT should be an essential part of the diagnosis prior to initiating root canal treatment.
Keywords
CBCT
maxillary molar
six canals

INTRODUCTION

Extensive research has been carried out in recent years regarding the unusual anatomy of permanent maxillary first molar tooth. Knowledge of the common anatomic characteristics and their possible variations is essential, because the non-treatment of even one canal can lead to endodontic treatment failure. The usual root canal anatomy of maxillary first molars have been described as three roots with three canals, with the commonest variation being the presence of a second mesiobuccal (MB) canal. This variation shows an incidence between 18% and 96.1%. Maggiore et al., reported the maxillary first molar having six canals namely two MB, three palatal (P), and one distobuccal (DB).[1] The occurrence of two canals in DB roots has been less frequent and has been reported in 3.6% of maxillary molars. Martinez-Berna and Ruiz-Badanelli reported three cases in which the maxillary first molars had presented six root canals (three in MB, two in DB, and one in P root).[2] Adanir reported six canals with one MB, two mesiopalatal (MP), two DB, and one P.[3] Alavi et al., and Thomas et al., reported the incidence of two canals in the DB root as 1.90% and 4.30%, respectively. Currently, technological advances have witnessed the introduction of CBCT to facilitate the assessment of internal anatomic variations of root canals. This imaging modality has been very useful in identifying anatomic features of the tooth and variations of the root canal system. Two-dimensional images are not effective in endodontic diagnosis and treatment planning.
We present two case reports and discuss the successful endodontic management of a maxillary first molar presenting with three roots and six root canals. This unusual morphology was confirmed with the help of CBCT scans.
CASE REPORTS
Case 1
A 19-year-old female patient presented to the Department of Conservative Dentistry, with pain in the maxillary right first molar that had persisted for the past two days. The pain became more intense on thermal stimuli and upon mastication. Detailed clinical examination revealed dental caries (mesio-occlusal) on the maxillary right first molar, which was tender to percussion. Periodontal assessment revealed a normal physiological status. The heating test using gutta percha stick (an endodontic dental chair side diagnostic tool) revealed a lingering pain after the removal of the stimulus. The heating test was first performed on the contralateral tooth and then on the adjacent tooth.
A preoperative radiograph in relation to the involved tooth revealed deep caries in the mesio-occlusal portion of the tooth involving the pulp space with periodontal ligament space widening in relation to MB root [Figure 1].

- Case 1. A 19-year-old female patient with pain in the right molar. Preoperative intra-oral periapical dental X-ray film shows deep caries on the mesial aspect (white arrow) of maxillary right first molar with pulpal involvement (dashed arrow).
A detailed review of the clinical and radiographic findings led to the diagnosis of acute irreversible pulpitis with acute apical periodontitis. Endodontic treatment was suggested and the procedure was explained to the patient.
The tooth was anesthetized with 1.8 mL (30 mg) 2% lignocaine containing 1:200,000 epinephrines (Xylocaine; AstraZeneca Pharma Ind Ltd, Bangalore, India) followed by rubber dam isolation and an endodontic access cavity was established. Clinical examination with a DG-16 endodontic explorer (Hu-Friedy, Chicago, IL) revealed two canal openings in each of the MB, and P root and one opening in the DB root. During further examination using surgical loupes a second canal was suspected in the DB orifice.
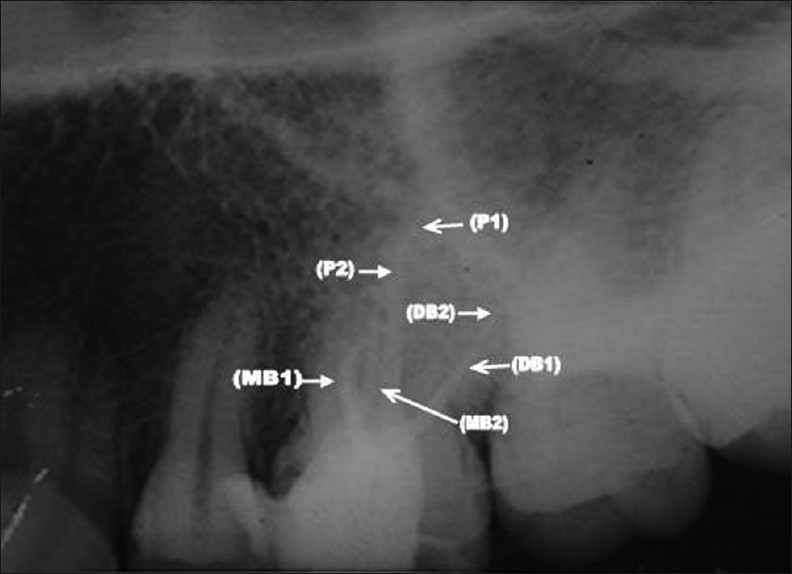
The working length was determined with the help of an apex locator (Tri Auto ZX, J Morita, Tokyo, Japan) and later confirmed using a radiograph. Multiple working length radiographs were taken at different angulations [Figure 2].

- Case 1. Intra-oral periapical dental X-ray film shows endodontic files in all six canals (MB1 (A), MB2 (B), DB1 (C), DB2 (D), P1 (E) and P 2 (F) of maxillary right first molar.
To confirm the unusual morphology it was decided to obtain a CBCT image of the tooth after obtaining the informed consent of the patient. With the files placed in the MB, DB, and P canals the scan was conducted. As it can be clearly seen in the CBCT image [Figure 3], the arrows in the figure point to the extra canals and the white dots indicate the instrument placed in the three located canals. An interim dressing of Cavit (3M ESPE) was placed. Further an intraoral image was taken to visualize the canals [Figures 4 and 5].

- Case 1. CBCT image of the maxillary right first molar. The white dots represent the position of endodontic files in the MB, DB and P orifices. The arrows depict the extra orifices (MB2, DB2 and P2).

- Case 1. Intra-oral photograph of the maxillary right first molar shows the two MB orifices and the two DB orifices.

- Case 1. Intra-oral photograph of the maxillary right molar shows the two P orifices.
In the next appointment the tooth was asymptomatic. Cleaning and shaping of the canals were performed under rubber dam isolation using ProTaper Nickel Titanium (NiTi) rotary instruments with a crown down technique, till File no. F2. Irrigation of the canals was done between each instrumentation using 2.5% NaOCl and 17% EDTA. Normal saline was used as the final irrigant.
The canals were subsequently dried with absorbent paper points and obturated using the F2 ProTaper cone and ZnOE sealer [Figure 6]. The tooth was then restored with a posterior composite Synergy D6 (Coltene, Whaledent). The patient was then advised to do a full coverage restoration.
- Case 1. Intra-oral peri-apical dental X-ray film clearly shows all the canals filled with gutta percha as a filling material. (MB1 canal, MB2 canal, DB1 canal, DB2 2 canal, P1 canal, P2 canal).
Case 2
A 25-year-old female patient presented to the Department of Conservative Dentistry, with pain in the maxillary left first molar for the past two days. Clinical and radiographic findings led to the diagnosis of acute irreversible pulpitis with apical periodontitis. Endodontic treatment was suggested and the procedure was explained to the patient.
After administration of adequate anesthesia endodontic access cavity was prepared. Clinical examination with a DG-16 endodontic explorer (Hu-Friedy, Chicago, IL) revealed two canal openings in the MB canal. The working length was determined with the help of an apex locator (Tri Auto ZX, J Morita, Tokyo, Japan) and later confirmed using a radiograph. To confirm the extra canal and to check for any aberrations in canal anatomy it was decided to obtain a CBCT image of the tooth. An interim dressing of Cavit (3M, ESPE) was placed and after an informed consent of the patient the CBCT image of the maxilla was performed. The image clearly reveals two canals in the MB orifice of the tooth [Figure 7]. Also a C-shaped orifice was seen in the P canal which helped to plan the correct technique for canal preparation.

- Case 2. A 25-year-old female patient with pain in the left first molar. CBCT image of the maxillary left first molar shows the MB2 orifice (black arrow) and C-shaped P orifice (white arrow).
Pulp extirpation was completed in all the canals and an interim dressing of Cavit (3M, ESPE) was placed in the canals.
In the subsequent check-up the tooth was found to be asymptomatic. Cleaning and shaping of the canals were performed under rubber dam isolation using ProTaper NiTi rotary instruments with a crown down technique till File no. F2. Irrigation of the canals was done after each instrumentation using 2.5% NaOCl and 17% EDTA. Normal saline was used as the final irrigant.
The canals were subsequently dried with absorbent paper points and obturated using the F2 ProTaper cone and ZnOE sealer [Figure 8]. The tooth was then restored with a posterior composite Synergy D6 (Coltene, Whaledent). The patient was then advised to do a full coverage restoration.

- Case 2. Intra-oral periapical dental X-ray film shows all the canals are filled with gutta percha as a filling material. (MB canal, MB2 canal, DB canal, and P canal).
DISCUSSION
A variety of study methods such as radiographs, magnification, clinical evaluations, dye injection, tooth sectioning and scanning electron microscopy have been discussed and reported by several authors for the detection of additional root canals.[4] Newer diagnostic methods such as computerized axial tomography (CT) scanning greatly facilitate access to the internal root canal morphology by allowing the operator to look at multiple slices of tooth roots and their root canal systems.[5] With CT scans, it is possible to reconstruct overlapping structures at arbitrary intervals, and, thus, the ability to resolve small subjects is increased. Additional advantage is the drastic reduction in scan time and effective dosages. CT scans are still not as accurate and do not limit the dosage to low as reasonably achievable.[6]
The use of newer diagnostic imaging modality as CBCT is fast gaining importance in diagnosis of unusual root canal morphology. The amount of information gained from conventional radiographs and digitally captured periapical radiographs is limited by the fact that the three-dimensional anatomy of the area is compressed into a two-dimensional image. CBCT has been used in endodontics for the effective evaluation of the root canal morphology along with the diagnosis of endodontic pathology, assessing root and alveolar fractures, analysis of re-absorptive lesions, identification of non-endodontic pathology, and pre-surgical assessment before root end surgery.[7–9]
The present case report emphasizes the use of CBCT for the identification of multiple root canals and subsequent success of the root canal treatment.
Matherne et al., in a study concluded that CBCT images resulted in the identification of greater number of root canal systems than digital images. Baratto Filho et al., evaluated the internal morphology of maxillary first molars by ex vivo and clinical assessments. They concluded that CBCT scanning along with the use of an operating microscope can be used as a good method for initial identification of maxillary first molar internal morphology. In a study by Jojo Kottoor et al., CBCT axial images confirmed the presence of three roots and seven root canals, namely mesiobuccal1 (MB1), mesiobuccal2 (MB2), mesiobuccal3 (MB3), distobuccal1 (DB1), distobuccal2 (DB2), mesiopalatal (MP) and distopalatal (DP).[10]
Furthermore although the occurrence of MB2 in maxillary first molars is very frequent, the other point that needs to be emphasized is the revelation of the C-shaped canal orifice for the palatal canals that helps the operator to choose the required biomechanical preparation.
CONCLUSION
The prognosis of an endodontic case definitely improves when CBCT is used for locating the extra canals. The current CBCT technology may have its limitations but one cannot totally rule out the possibility of using CBCT as a diagnostic tool for endodontic purposes.
ACKNOWLEDGMENT
The authors acknowledge the contribution of Dr. Sonam Mahajan and Dr. Pragya Tripathi Postgraduate students, Institute of Dental Studies And Technologies, Kardrabd, Modinagar, Uttar Pradesh, India, in the preparation of this manuscript.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/50/100370
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- An unusual maxillary first molar with four roots and six canals: A case report. Aust Dent J. 2007;52:333-5.
- [Google Scholar]
- Analysis of the internal anatomy of maxillary first molars by using different methods. J Endod. 2009;35:337-42.
- [Google Scholar]
- New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int Endod J. 2009;42:447-62.
- [Google Scholar]
- Spiral volumetric CT with single-breadth-hold technique, continuous transport and continuous scanner rotation. Radiology. 1990;176:181-3.
- [Google Scholar]
- The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40:818-30.
- [Google Scholar]
- Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34:87-9.
- [Google Scholar]
- Maxillary first molar with seven root canals diagnosed with cone beam computed tomography; a case report. J Endod. 2010;36:915-21.
- [Google Scholar]




