
Translate this page into:
TRAP Sequence - An Interesting Entity in Twins
Address for correspondence: Dr. Srinivas Prasad, R.H, B1 Prakruthi Apartments, Railway Men Colony, LG Halli, RMV, Bangalore, Karnataka, India. E-mail: drsrinivasprasad@gmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Twin reversed arterial perfusion (TRAP) sequence, is a rare malformation occurring in monozygotic multiple gestations. One well-developed normal (pump) twin and the other twin with absent cardiac structure (acardiac), who is hemodynamically dependent on the normal (pump) twin are characteristic of this syndrome. The acardiac twin develops multiple anomalies that make survival difficult. The prognosis of the pump twin is variable with mortality rate ranging from 50% to 70%. Complications that affect the prognosis of the pump twin include complications of congestive cardiac failure due to increased cardiac demand, prematurity secondary to preterm delivery, and polyhydramnios. Because of these complications prompt detection, follow-up, and treatment of this condition is very important. We report two cases of TRAP sequence that emphasizes the importance of gray-scale and color Doppler imaging in diagnosis, detection of poor prognostic features, follow-up, and management of TRAP sequence.
Keywords
Acardiac twin
color doppler
TRAP sequence
ultrasound

INTRODUCTION

Twin reversed arterial perfusion (TRAP sequence), previously termed as ‘acardiac twin gestation’, represents a syndrome characterised by vascular anastamosis and partial or complete lack of cardiac development in one of the twins. It is a rare complication unique to monozygotic, multiple pregnancies. This condition occurs in 1 in 35000 pregnancies and in 0.3% of all monozygotic twin gestations.[12] Without prompt detection, follow-up, and treatment, mortality rates for pump twins have been noted to be as high as 50% to 70%.[12] Early sonographic diagnosis, appropriate follow-up, and intervention have been associated with substantial improvements in survival.[34] We report two cases that emphasize the value of gray-scale ultrasound and color Doppler techniques for both diagnosis of TRAP sequence and detection of prognostic features.
CASE REPORTS
Case 1
A 26-year-old female with G1P0L0A0 (Gravida 1/Para 0/Obortus 0) underwent ultrasound examination to detect the presence of congenital anamolies. Ultrasound scan revealed monochorionic, monoamniotic, twin pregnancies. The pump twin was normal. The recipient twin demonstrated well-developed lower limbs, partially developed lumbar and thoracic spine, absent cervical spine, under-developed abdominal and chest organs. Heart was absent, head and face were absent, and upper limbs were absent [Figure 1]. Cystic hygroma with diffuse soft tissue edema [Figure 2] and single umbilical artery [Figure 3] with reversal of flow [Figure 4] were detected. The weight of the recipient twin was less than 70% of the pump twin. Polyhydramnios was noted as Amniotic fluid Index (AFI) was 29 cm. Complications and options for treatment were discussed with the patient. Patient opted to continue the pregnancy without any treatment.

- Sonogram of Case 1 recipient twin demonstrates well-developed lower limbs, partially developed abdomen and thorax, absent head and upper limbs and diffuse soft tissue edema.

- Sonogram of Case 1 recipient twin demonstrates thickened soft tissue along the dorsal aspect suggestive of cystic hygroma.

- Color Doppler sonographic image of Case 1 demonstrates two vessel umbilical cords with single umbilical artery.
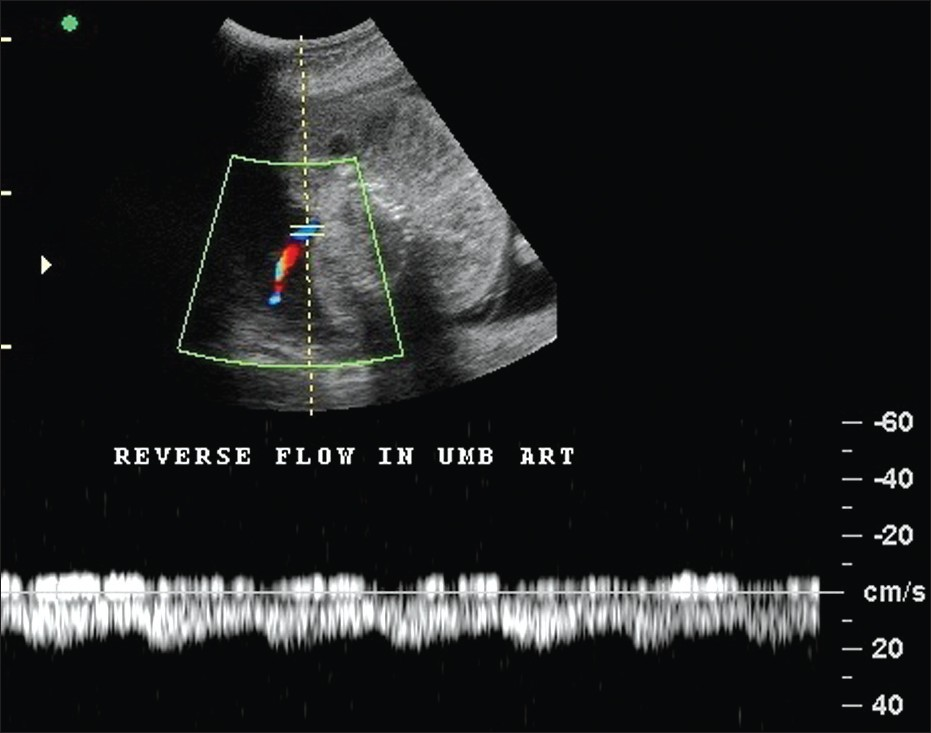
- Pulsed Doppler sonographic image of Case 1 demonstrates reversal of flow in the umbilical artery.
Case 2
A 22-year-old G3 P1 L1 A1 female who had complaints of lower abdominal pain was referred to our department for sonography. Ultrasound findings showed monochorionic, monoamniotic, twin gestations with one normal twin (pump twin) and the other twin (recipient twin) demonstrating multiple anomalies. The recipient twin had well-developed lower limbs that were directed posteriorly [Figure 5], underdeveloped abdomen with absent anterior abdominal wall, underdeveloped chest with hypoplastic ribs, absent cardia, underdeveloped upper limbs with single forearm bone, oligodactyly and club hand [Figure 6], cystic hygroma with diffuse soft tissue edema [Figure 7], microcephaly with dilated lateral and third ventricles [Figure 7], bilateral cleft lip/palate, and single umbilical artery with reversal of flow in umbilical vessels. The weight of the recipient twin was less than 70% of the pump twin. Polyhydramnios was noted as AFI was 28 cm. Later the patient was subjected to TRAP circulation ablation using a 20-gauge needle and absolute alcohol (0.5 ml) under the guidance of color Doppler sonography. Color Doppler sonography on the next day confirmed the absence of blood flow in the recipient twin. Patient was monitored regularly with gray-scale and Doppler scans. These revealed no evidence of volume overload in the pump twin. At 35 weeks of gestation, emergency lower section caesarean section (LSCS) was carried out, as the patient went into labor. A healthy male twin (pump twin) weighing 2.03 kg and an anomalous twin (recipient) were delivered [Figure 8].

- Sonogram of Case 2 recipient twin demonstrates well-developed lower limbs with diffuse soft tissue edema.

- Sonogram of Case 2 recipient twin demonstrates club hand.

- Sonogram of Case 2 recipient twin demonstrates diffuse soft tissue edema and cystic hygroma (arrow).

- Specimen of Case 2 recipient twin demonstrates microcephaly, cystic hygroma, bilateral cleft lip, club hand, under developed chest and omphalocele.
DISCUSSION
TRAP sequence is a rare anomaly that occurs in monozygotic twins. The etiology and patho-physiological mechanisms are not well understood. Many investigators have put forward the hypothesis that disruption of organogenesis occurs secondary to the presence of reversed flow through an abnormal artery-to-artery placental anastamosis resulting in cardiac and other malformations.[4] However, other researchers propose the hypothesis that initial abnormal cardiac formation during embryogenesis initiates the development of this anomaly.[5]
In TRAP sequence, the normal twin acts as the ‘pump’ twin which donates blood to the abnormal twin called ‘recipient’ twin through an abnormal artery-to-artery or venous-to-venous communication in the placenta. This results in reversal of flow in the umbilical cord vessels of the recipient twin, oxygenated blood enters the fetus through the umbilical artery and deoxygenated blood leaves the fetus through the umbilical vein, which is opposite to the normal blood flow pattern to a fetus. This has led to the term TRAP sequence for this anomaly.[6] As a result of an imbalance in the inter-fetal circulation, the caudal aspect of the perfused fetus receives blood with relatively more nutrients and oxygen than the upper torso, resulting in better development of pelvis and lower extremities. Fully de-saturated blood then flows in a retrograde fashion to the upper body and head, leading to faulty development of the heart and upper torso, which are either completely absent or severely deformed.[6]
Congenital anomalies are present in about 9% of pump twins. The overall perinatal mortality of pump twins is 50-55%. This is generally due to either polyhydraminos leading to premature delivery or secondary to congestive cardiac failure developing due to the increased cardiac output secondary to the abnormal inter-fetal circulation.[6] This high cardiac output also increases perfusion of the fetal kidneys, resulting in overproduction of fetal urine and polyhydramnios.
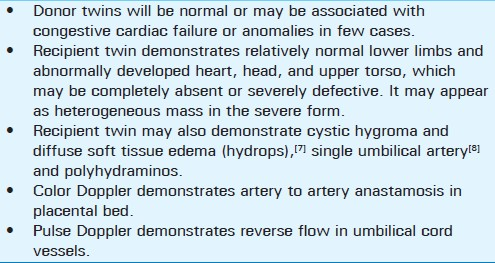
The sonographic findings that aid in diagnosis of TRAP sequence are summarized in Table 1.
CONCLUSION
Role of sonography in the management of TRAP sequence cases
Weight ratio
The twin reversed-arterial-perfusion sequence (TRAP-sequence) carries a poor prognosis with a mortality rate of approximately 50%. The prognosis is directly related to the weight of the recipient twin and the pump twin. Higher the weight of the recipient twin the more likely is the development of cardiac insufficiency in the pump twin. The weight of the acardiac twin cannot be calculated from the values of the head circumference, abdominal circumference, and femur length using the standard formulae (such as Hadlock's). Instead, the weight (in grams) of the acardiac twin is calculated using the following formula: (1.2 × longest length2) - (1.7 × longest length).[7] Recently, Wong and Sepulveda suggested using the abdominal circumference ratio as a prognostic factor in evaluating the impact of the acardiac fetus on the pump twin.[8] When the ratio of the weight of the acardiac fetus to the weight of the donor fetus is greater than 70%, the incidence of preterm delivery is 90%, that of polyhydramnios is 40%, and that of congestive heart failure in the pump twin is 30%. In comparison, the corresponding rates are 75%, 30%, and 10%, respectively, when the ratio is less than 70%.[9]
Vessel occlusion
Prenatal treatment involves occlusion of blood flow to the acardiac twin by endoscopic (fetoscopic) ligation, laser coagulation of the umbilical cord, bipolar cord cauterization, ablation using radiofrequency, or with absolute alcohol.[10] Alcohol treatment was used in Case 2. The indications for prenatal treatment with vessel occlusion include polyhydramnios, cardiac dysfunction, hydrops of the pump twin, or a relatively large weight of the acardiac twin.[7]
Use of digoxin
Fetal cardiac insufficiency can be diagnosed and treated with digoxin. Treatment is initiated after the sonographic diagnosis of fetal cardiac insufficiency.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/56/100997
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- The acardiac monster: A review of the world literature and presentation of 2 cases. Am J Obstet Gynecol. 1960;80:582-9.
- [Google Scholar]
- Perinatal outcome of forty-nine pregnancies complicated by acardiac twinning. Am J Obstet Gynecol. 1990;163:907-12.
- [Google Scholar]
- Twin reversed arterial perfusion (TRAP) sequence: A study of 14 twin pregnancies with acardius. Semin Perinatol. 1983;7:285-93.
- [Google Scholar]
- Multiple pregnancy: Acardiac twins. In: Pathology of the Human Placenta (2nd ed). New York NY: Springer; 1995. p. :792-810.
- [Google Scholar]
- Sonography of multifetal pregnancy. In: Rumack Carol M, ed. Diagnostic ultrasound Vol 2. (3rd ed). Missouri: Elsivier Mosby; 2005. p. :1207-9.
- [Google Scholar]
- Ultrasound evaluation of multiple pregnancies. In: Callen PW, ed. Ultrasonography in obstetrics and gynaecology (5th ed). Pennsylvania: W B Saunders; 2008. p. :286-8.
- [Google Scholar]
- Acardiac anomaly: Current issues in prenatal assessment and treatment. Prenat Diagn. 2005;25:796-806.
- [Google Scholar]
- Ultrasound evaluation of multifetal gestations. In: Callen PW, ed. Callen ultrasonography in obstetrics and gynaecology (4th ed). Pennsylvania: W B Saunders; 2000. p. :196-8.
- [Google Scholar]




