
Translate this page into:
Telescoping Technique to Engage Left Main Coronary Artery in a Case of Giant Aortic Aneurysm in a Geriatric Patient
Address for correspondence: Dr. Rahul Vasudev, Department of Internal Medicine, New York Medical College, St. Joseph's Regional Medical Center, Paterson, NJ 07503, USA. E-mail: drrahulvasudev@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We present a case of a geriatric male with giant ascending aortic aneurysm (AAA) who underwent successful coronary angiography using telescoping technique for evaluation his coronary arteries before surgery for AAA. Since the ascending aorta and root were extremely dilated, we knew it would not have been possible to engage the coronaries using regular catheters and standard technique. Hence, telescopic technique was used. Amplatz left 3 (AL3) 7F (French) guide catheter (90 cm) was initially used, and nonselective injection of contrast was done to see the coronary ostium. After that, a 5F multipurpose catheter (110 cm) was telescoped through 7F AL3 guide catheter to engage the ostium of the left main coronary artery. Using this technique, images of coronaries were obtained, and it showed minimal luminal irregularities in major epicardial coronary arteries. The patient underwent successful surgery with aortic valve replacement and excision of aneurysm with graft placement. Although this technique has been described previously in enlarged aortas, this is the first to our knowledge use of telescoping technique in giant aortic aneurysm in a geriatric patient.
Keywords
Cardiac catheterization
cardiac imaging and giant aortic aneurysm
telescoping technique

INTRODUCTION
Giant aortic aneurysm is defined as aortic diameter >10 cm.[1] It is rare since most patients present with complications such as rupture before reaching that stage. The annual rate of rupture is 14%, once the diameter increases above 6 cm, and hence it is uncommonly seen in practice. Atherosclerosis is one of the most common causes of aortic aneurysm. Genetic causes include conditions such as aortopathy associated with bicuspid aortic valve, Marfan's syndrome, vascular type Ehlers–Danlos syndrome, Loeys–Dietz syndrome, and Turner's syndrome. Some other causes are giant cell arteritis, tuberculosis, syphilis, HIV-associated vasculitis, hereditary hemorrhagic telangiectasia, and medial agenesis.[1]
Evaluation of coronary arteries is usually required in patients ascending aortic aneurysm (AAA) before the patient is taken for surgery if there are risk factors. There are usually two options computed tomographic (CT) coronary angiography or conventional coronary angiography. In a giant aortic aneurysm, conventional angiography might not be possible as it is very difficult to engage the coronaries using regular catheters and standard technique. We describe the use of telescoping technique in such a patient. This is the first to our knowledge use of telescoping technique in giant aortic aneurysm in a geriatric patient.
CASE REPORT
A 78-year-old male with history of hypertension, dyslipidemia, and prosthetic aortic valve replacement presented to the emergency department with complaints of exertional shortness of breath for few days. Chest X-ray showed widened mediastinum. Subsequently, CT angiogram of the chest showed massively dilated ascending aorta with maximum diameter of 10.2 cm [Figure 1]. Transthoracic echocardiogram revealed normal ejection fraction with mild aortic insufficiency, well-functioning prosthetic aortic valve, and no aortic stenosis. His creatinine was 1.8 mg/dl, and he had received 150 ml of contrast for CT angiogram. It was necessary to evaluate his coronary arteries before surgery for AAA.
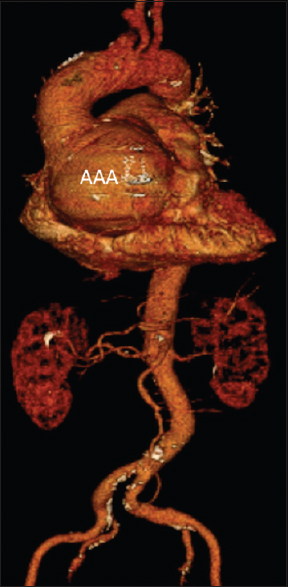
- A 78-year-old male with history of aortic valve replacement presented with dyspnea on exertion. Three dimensional reconstructed image of computed tomographic of the aorta shows giant aortic root of 10.2 cm labeled as ascending aortic aneurysm.
There were two options in this case: coronary CT angiography or conventional coronary angiography. Coronary CT angiography would require about 150 ml of contrast.[2] A diagnostic coronary angiogram can be done using about 50 ml of contrast.[3] Given his renal insufficiency, we decided to do conventional coronary angiography. Since the ascending aorta and root were extremely dilated, we knew it would not be possible to engage the coronaries using regular catheters and standard technique. Hence, telescopic technique was used. Amplatz left 3 (AL3) 7F (French) guide catheter (90 cm) was initially used, and nonselective injection of contrast was done to see the coronary ostium [Figure 2 and Video 1]. After that, a 5F multipurpose (MP) catheter (110 cm) was telescoped through 7F AL3 guide catheter to engage the ostium of the left main coronary artery [Figure 3 and Video 2]. Using this technique, images of coronaries were obtained, and it showed minimal luminal irregularities in major epicardial coronary arteries. Total of 50 ml contrast was used. The patient underwent successful surgery with aortic valve replacement and excision of aneurysm with graft placement. The most likely etiology of giant aortic aneurysm in our patient was atherosclerosis. However, we did not have any record of his previous aortic valve surgery, and we do not know if it was a bicuspid aortic valve. In that case, he could have had aortopathy associated with bicuspid aortic valve.
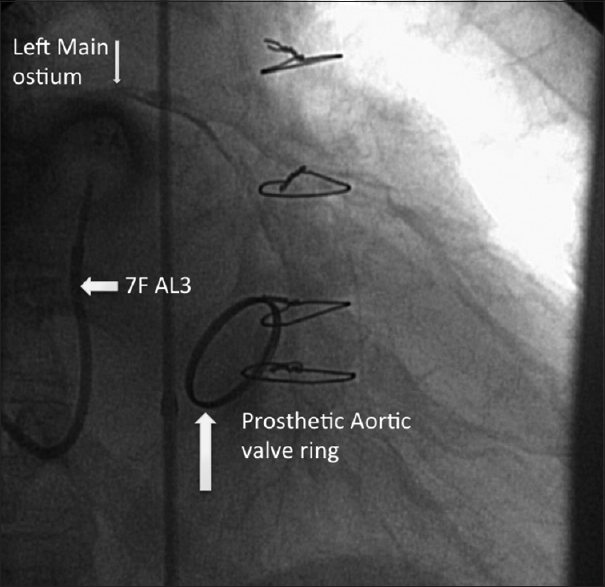
- A 78-year-old male with history of aortic valve replacement and giant aortic root. Coronary angiogram in left anterior oblique cranial view showing left main ostium (downward pointing arrow) through nonselective contrast injection by (leftward pointing arrow) 7 French Amplatz left 3 catheter.
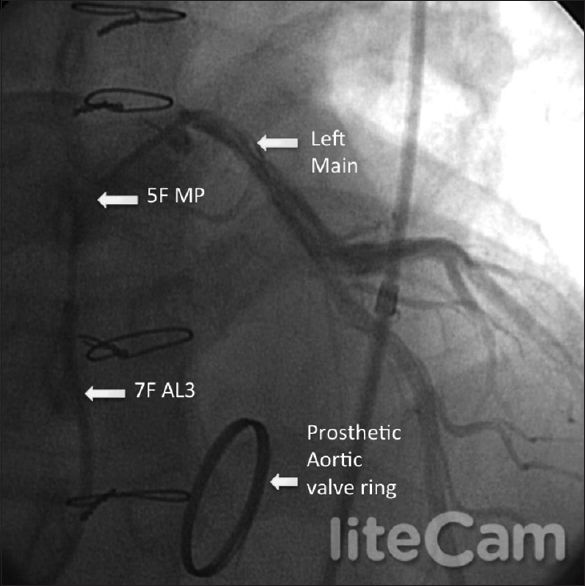
- A 78-year-old male with history of aortic valve replacement and giant aortic root. Coronary angiogram in left anterior oblique cranial view showing proper engagement of left main ostium with 5 French multipurpose catheter telescoped through 7 French Amplatz left 3 catheter. Left main is clearly seen branching into left anterior descending and left circumflex arteries.
DISCUSSION
Telescopic systems use has been described in carotid and brachial angiographic procedures.[45] It has also been described for balloon/stent delivery in coronaries.[6] However, there have been only three prior case reports of such technique in dilated aorta.[789] None of those cases had giant aortic aneurysm. Ours is the first case to show that coronary angiography can be performed relatively easily with the use of telescoping technique in geriatric patients who have giant aortic aneurysm. Two catheters with different diameters are required for this technique the larger one (guide catheter) and smaller one (telescoping catheter). First, the larger diameter catheter is advanced as far as it can go to the aorta and a non-selective injection should be done to indicate the ostium of the coronary artery. Then smaller diameter catheter (but longer in length compared to larger diameter catheter) is inserted through the larger diameter catheter and telescoped through it to engage the ostium of the coronary artery. By this technique, images of coronary arteries can be obtained. In cases of massively dilated aorta, a catheter-like AL that points upward is needed for the nonselective shot to show the ostium of the left main coronary artery. This catheter can be used as guide (7F AL3 in this case), and it should have an inner diameter slightly larger to fit the telescoping catheter. The telescoping catheter should be longer in length than the guide catheter to be able to engage the ostium as 5F MP catheter (110 cm) in our case, which was telescoped through 7F AL3 guide catheter to engage the ostium of the left main coronary artery. This technique can be used when CT coronary angiogram cannot be done due to renal insufficiency or arrhythmias such as atrial fibrillation (which precludes the use of CT coronary angiogram).
Advantages of conventional coronary angiography over CT coronary angiography are: (i) Functional assessment of stenosis can be done by fractional flow reserve for intermediate lesions, (ii) can be done in patients with arrhythmias such as atrial fibrillation or frequent atrial or ventricular premature contractions. Disadvantages include: it is invasive procedure and hence has associated risks such as bleeding, infection, and dissection.[2]
In the future, magnetic resonance angiography (MRA) might become a noninvasive option for such patients, but currently its use has been limited by limitations in visualizing distal segment and small branch disease. However, coronary MRA still has a role in the evaluation of anomalous coronary artery origins particularly in pediatric patients.[10]
CONCLUSION
Telescoping technique can be very helpful in geriatric patients for evaluation of coronaries when it is difficult to engage the coronaries using regular catheters and standard technique due to dilatation of ascending aorta and root, and when CT coronary angiogram cannot be done.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos Available on: www.clinicalimagingscience.org
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2016/6/1/42/192829
REFERENCES
- Giant dissecting aortic aneurysm in an asymptomatic young male. Case Rep Vasc Med. 2015;2015:958464.
- [Google Scholar]
- 64-multislice detector computed tomography coronary angiography as potential alternative to conventional coronary angiography: A systematic review and meta-analysis. Eur Heart J. 2007;28:3042-50.
- [Google Scholar]
- Ultra-low contrast volumes reduce rates of contrast-induced nephropathy in patients with chronic kidney disease undergoing coronary angiography. J Am Coll Cardiol. 2008;51:89-90.
- [Google Scholar]
- Super-selective cerebral angiography. III. Diagnostic use and therapeutic possibilities of the telescopic catheterization technic in the circulation area of the external carotid artery in man. Rofo. 1976;125:214-8.
- [Google Scholar]
- Successful crossing of a severe spasm of the brachial artery using a telescopic approach. Int J Cardiovasc Intervent. 2005;7:63-4.
- [Google Scholar]
- New method to increase a backup support of a 6 French guiding coronary catheter. Catheter Cardiovasc Interv. 2004;63:452-6.
- [Google Scholar]
- Coaxial technique for catheterization of the coronary arteries with a very dilated ascending aorta. Catheter Cardiovasc Interv. 2004;62:32-4.
- [Google Scholar]
- “Telescopic” technique for selective coronary angiography in severely dilated ascending aorta. Catheter Cardiovasc Interv. 2007;69:1078-9.
- [Google Scholar]
- Telescoping catheter technique for enlarged aortas. Catheter Cardiovasc Interv. 2009;74:1126-8.
- [Google Scholar]
- Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med. 2001;345:1863-9.
- [Google Scholar]




