
Translate this page into:
Seizure Mimicking Stroke: Role of CT Perfusion
Address for correspondence: Dr. Vishnumurthy Shushrutha Hedna, Department of Neurology, University of Florida, Gainesville, Florida 32611, USA. E-mail: vhedna@mail.ufl.edu
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Stroke mimics constitute 15--20% of all cases presenting to the emergency department, prominent among them being seizures, hypoglycemia, tumors, migraines, and posterior reversible leucoencephalopathy. They have also abnormal computerized tomography perfusion (CTP) findings. We report a case where CTP helped us to diagnose and treat a seizure when initial presentation was that of a stroke.
Keywords
CT perfusion
seizure
stroke mimic
stroke
stroke alert

INTRODUCTION

The CT perfusion (CTP) is an important modality in acute stroke imaging to delineate the infarct from ischemic penumbra especially when considering tissue plasminogen activators (t-pa) and endovascular intervention (EI). It is a very sensitive measure of cerebral blood flow dynamics playing a vital role in diagnosing stroke mimics like seizures, migraine, tumors, abscess, hypoglycemia, and posterior reversible encephalopathy syndrome (PRES), when they present to emergency department as a stroke.[1] Even though intravenous t-pa is the standard of care in acute ischemic strokes, if given to nonstroke patients, they may contribute to morbidity. We present a case report where CT perfusion of the brain played a significant role in the diagnosis and management.
CASE REPORT
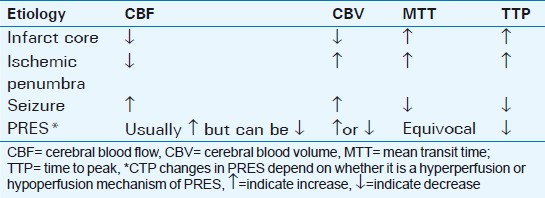
An 83-year-old male was brought in as a stroke alert. He was seen by paramedics (EMS) as obtunded, nonverbal, with left gaze deviation, and flaccid right extremity. There was no past medical history of seizures, but EMS noticed an episode of seizure on the way to the hospital and intubated him for airway protection. The risk factors included hypertension, COPD, and dyslipidemia. The NIH stroke scale on arrival was 20. The history and physical examination was limited in view of intubation and sedation. The plain CT head was normal. The brain CT perfusion (CTP) showed [Figures 1 and 2] reduced time to peak (TTP), increased cerebral blood flow (CBF), and volume (CBV). This made us suspect a diagnosis of seizure rather than a stroke. In ischemic stroke the core infarct would show increased time to peak (TTP), reduced cerebral blood flow (CBF), and volume (CBV) whereas penumbra would show increased time to peak (TTP), reduced cerebral blood flow (CBF) but increased blood volume (CBV) [Table 1]. The diagnosis of seizure was confirmed by further evaluation and treated successfully.
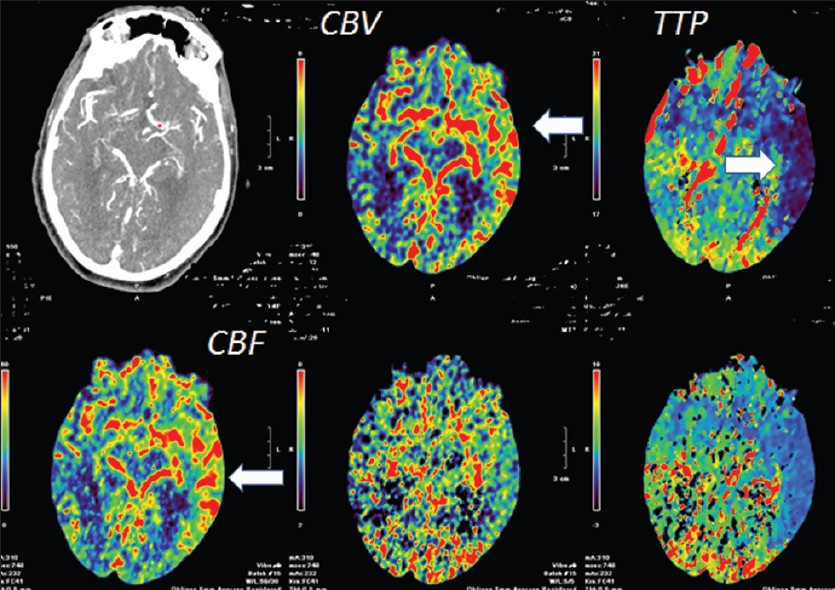
- CT perfusion axial view at the level of the sylvian fissure demonstrate reduced TTP (white arrows) in the parietal-temporal lobe with corresponding increase in cerebral blood flow (CBF) (white arrows) and cerebral blood volume (CBV) (white arrows) suggestive of increased blood flow in these areas. There was no much observable change in the MTT. Mean transit time (MTT), is a measure of the mean time for blood/contrast to perfuse a region of tissue. Cerebral blood volume (CBF) = CBV/MTT.
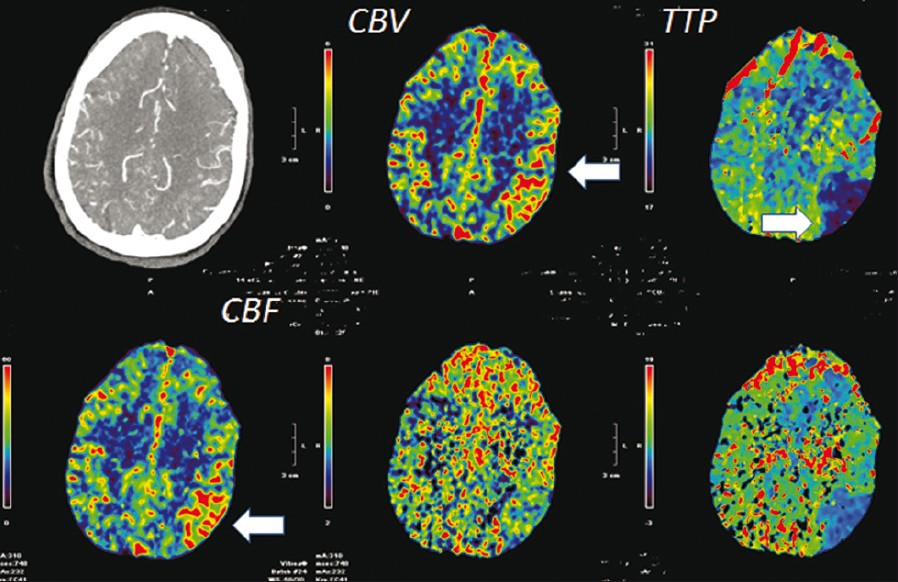
- CT perfusion axial view at the cerebral high convexity level demonstrate reduced TTP (white arrows) in the parietal-temporal lobe with corresponding increase in cerebral blood flow (CBF) (white arrows) and cerebral blood volume (CBV) (white arrows) suggestive of increased blood flow in these regions.
DISCUSSION
The CT perfusion is a quick, fast imaging modality which if incorporated in acute stroke imaging will shed light not only on the infarct size and penumbra but also delineate conditions mimicking stroke. When a patient presents with stroke-like symptoms and altered sensorium is one of the presenting complaints, the differential can be wide including intra-cerebral hemorrhage, large frontal infarcts, thalamic infarcts, infarcts involving the reticular activating system, hypoglycemia, postictal states, and other stroke mimics. Acute post-stroke epilepsy is not a rare entity and can present with focal neurological deficits mimicking stroke.[2] When the patient is obtunded, intubated, or in no position to participate in the clinical assessment, imaging plays a significant role. Since the ictal focus has high metabolic demand[3] due to excito-toxicity there will be hyperperfusion, which is manifested in the perfusion studies as above. Plain CT head without the perfusion in the above scenario with the described neurological examination would have wrongly led to intravenous thrombolysis. However, limitations for CT perfusion studies are exposure to additional radiation (also intravenous contrast), additional delay (15 minutes) in care, and cost of the procedure.
CONCLUSION
The brain CTP is a very sensitive imaging in acute strokes and can also play a pivotal role in diagnosis of stroke mimics. However, caution is advised in interpretation of perfusion images and needs to be done in conjunction with the clinical story rather than in isolation.
ACKNOWLEDGMENTS
Publication of this article was funded in part by the University of Florida Open-Access Publishing Fund.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/32/97728
REFERENCES
- Stroke vs. status epilepticus. A case report utilizing CT perfusion. J Neurol Sci. 2008;266:174-6.
- [Google Scholar]
- Seizures in acute stroke: Predictors and prognostic significance. The Copenhagen Stroke Study. Stroke. 1997;28:1585-9.
- [Google Scholar]
- Comparative study of interictal PET and ictal SPECT in complex partial seizures. Acta Neurol Scand. 1997;95:129-36.
- [Google Scholar]




