
Relationship Between Amniotic Fluid Index and Ultrasound Estimated Fetal Weight in Healthy Pregnant African Women
Address for correspondence: Dr. Ademola A. Adeyekun, Department of Radiology, University of Benin Teaching Hospital, Benin City, Nigeria. E-mail: adeyekunaa@yahoo.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Fetal weight (FW) estimation in late pregnancy is an important guide in obstetric care. Amniotic fluid protects the fetus against traumatic and infective insults. There possibly exists a relationship between FW and amniotic fluid index (AFI) that can be estimated by ultrasonography.
Materials and Methods:
Two hundred and fifty-eight low-risk pregnancies were prospectively studied by means of ultrasound over a 12-month period. FW was estimated using a combination of fetal parameters; bi-parietal diameter, fetal trunk cross sectional area, and femur length. AFI was assessed using the 4-quadrant method. Spearman's correlation was used to test possible relationship between amniotic fluid indices and estimated FW pairs. The level of statistical significance was set at P ≤ 0.05.
Results:
The mean AF1 and estimated fetal weight (EFW) pairs were as follows: at 27-29 weeks the values were 172.1 mm and 1,250.2 g; at 30-32 weeks AF1 and EFW values were 170.3 mm and 1,648.0 g; at 33-35 weeks values were 162.3 mm and 2,273.5 g; at 36-38 weeks values were 144.09 mm and 2,906.1 g; at 39-40 weeks AF1 and EFW values were 125.0 mm and 3,222.6 g. Overall, there was no statistically significant relationship between AFI and EFW (P > 0.05; r = 0.241).
Conclusion:
While FW calculations and amniotic index showed variations in value in late pregnancy, there does not appear to be a linear relationship between ultrasound estimate of FW and amniotic index. The implication of this is that fetal size need not be taken into cognizance when alterations in amniotic fluid values are noted.
Keywords
Amniotic fluid
foetal weight
ultrasound
Nigerian women

INTRODUCTION

Sonographic estimation of fetal weight (FW), especially in late pregnancy is an important guide in obstetric care. This is particularly important when dealing with growth restricted or large for date babies.[1] Armed with this information informed decisions about delivery can be taken, thereby minimizing perinatal morbidity and mortality.[2]
Amniotic fluid cushions the fetus from traumatic forces, cord compression, and pathogens, as well as playing an essential role in fetal lung development.[3] In late pregnancy, amniotic fluid production is largely dependent on fetal micturition[4] and renal size in the newborn has been shown to bear a significant relationship to birth weight.[5] It is therefore, reasonable to postulate a relationship between sonographically determined amniotic fluid index (AFI) and estimated FW.
Previous reports have investigated possible relationships between sonographically attained fluid index, and estimated fetal weight (EFW)[36] including the influence of AFI on the accuracy of sonographically EFW, among Caucasians. However, such studies are rare among Africans, especially Nigerians. This study was carried out to find out if any significant relationships exist between AFI and EFW in a Nigerian cohort of healthy pregnant women.
MATERIALS AND METHODS
This was a prospective study. Two hundred and fifty-eight low-risk pregnant subjects referred for routine ultrasound scans to the Radiology Department of the University of Benin Teaching Hospital, Nigeria were randomly selected over a 12-month period. Those with unsure dates, diabetes mellitus, and hypertensive disorders were excluded. Only those whose menstrual dates did not vary significantly from the estimated gestational age at first scan were enlisted. Approval of the Hospital's Ethics and Research Committee was sought and obtained.
Sonography was performed with a 3.5 MHz transducer (Fukuda Denshi; Fukuda Co Ltd, Japan). Cases found to have oligo- or poly-hydramnios and fetal anomalies were excluded. AFI was assessed using the four-quadrant technique as described by Phelan.[7] The sum of the measurements from the four quadrants was recorded for each subject. Fetal biometrics including biparietal diameter (BPD), using the cavum septum pellucidum as landmark, as depicted in Figure 1; fetal trunk cross sectional area (FTA) using the four chamber view of the heart, as illustrated in Figure 2; and the femur length (FL), with the ‘hook’ from the greater trochanter to the distal metaphysis included, as illustrated in Figure 3, were measured. The FW was automatically estimated by the scanner using a combination of the BPD, FTA, and FL, based on the in-built Osaka University system's formula. This is illustrated by Figures 4 and 5. All measurements were made by the first author. No patient was included more than once.
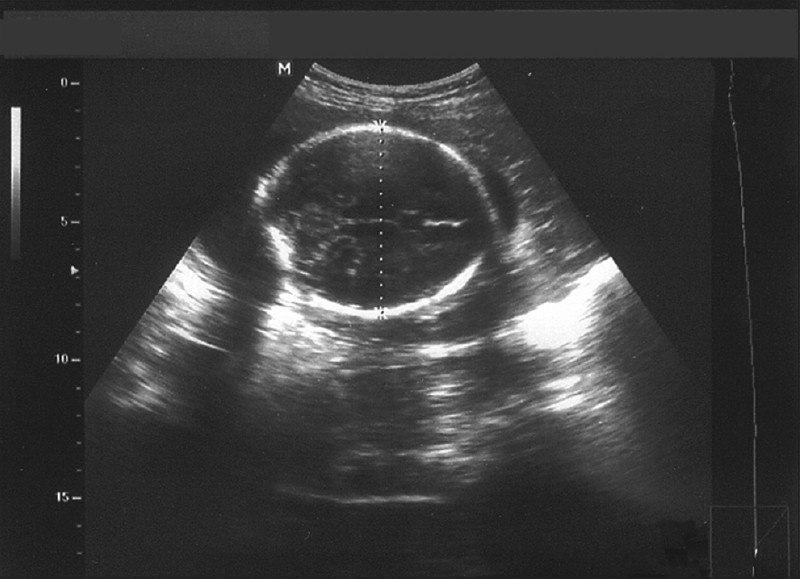
- Ultrasound scan of abdomen shows how biparietal diameter is measured.
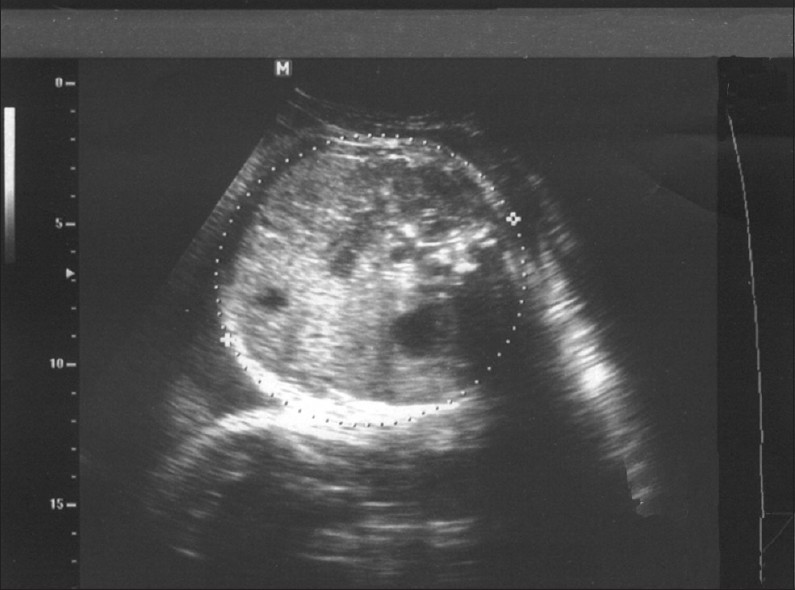
- Ultrasound scan shows how to measure fetal trunk cross sectional area, using the four chamber view of the heart.
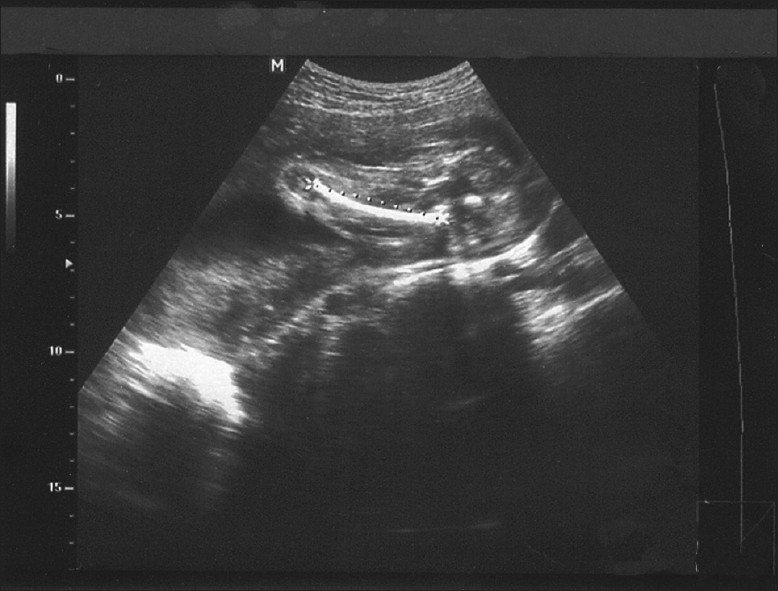
- Ultrasound scan shows how to measure femur length, with the ‘hook’ from the greater trochanter to the distal metaphysis included.

- Sample report 1 shows estimated fetal weight calculated by the Osaka University system's formula.
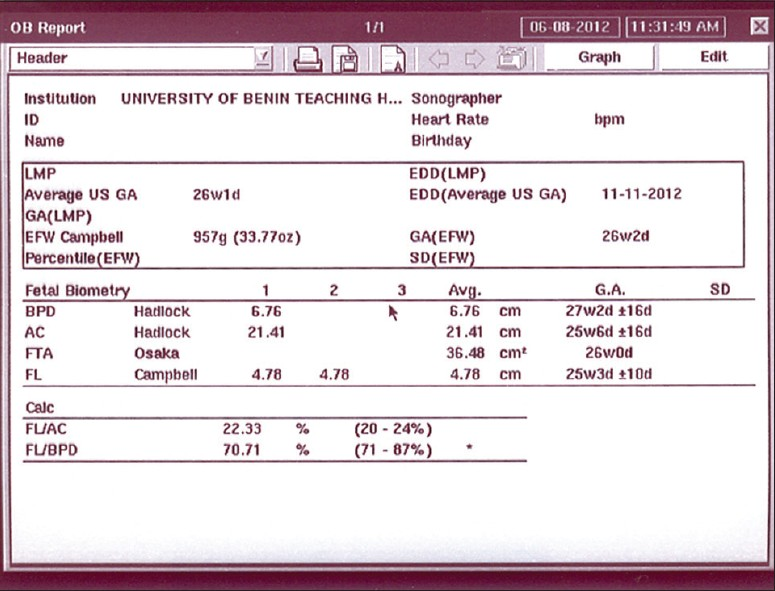
- Sample report 2 shows estimated fetal weight calculated by the Osaka University system's formula.
Data was entered into a Microsoft spreadsheet and analysed using the Statistical Package for the Social Sciences (SPSS version 16). Measurements were stratified into pairs of AFI and EFW as follows; 27-29 weeks, 30-32 weeks, 33-35 weeks, 36-38 weeks, and 39-41 weeks. Spearman's correlation was used to test possible relationship between the AFI and EFW pairs. The level of significance was set at “P” values less than or equal to 0.05.
RESULTS
A total of 258 subjects were sonographically examined. The mean age of the subjects was 29.1 ± 4.9 years, and parity ranged from 0 to 7, with a mean of 1.5. The mean maternal weight was 71.4 ± 13.6 kg, and height was 1.6 ± 0.5 m.
The number of subjects in each gestational group were distributed as follows; 64 (24.8%) in the 27-29 weeks, 56 (21.7%) in the 30-32 weeks; 48 (18.6%) in the 33-35 weeks; 50 (19.4%) in the 36-38 weeks, and 40 (15.5%) in the 39-41 weeks; as outlined in Table 1.
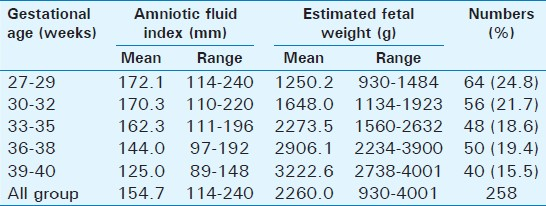
Table 1 also shows that the mean AFI and EFW values for 27-29 weeks gestation were 172.1 mm and 1250.19 g respectively; 30-32 weeks were 170.3 mm and 1,648.04 g; 33-35 weeks were 162.3 mm and 2,273.54 g; 36-38 weeks were 144.0 mm and 2,906.12 g; and 39-41 weeks were 125.0 mm and 3,222.65 g. Spearman's correlation values between AFI and EFW were 0.123, 0.472, 0.179, 0.210, and 0.221 for 27-29 weeks, 30-32 weeks, 33-35 weeks, 36-38 weeks, and 39-41 weeks respectively. There was no significant association between AFI and EFW for all subdivisions of gestation age, except in the 30-32 weeks group (P < 0.05; r = 0.472). Overall, there was no statistically significant relationship between AFI and EFW (P > 0.05; r = 0.241). Figure 6 shows the scatter plot diagram for all pairs of AFI and EFW, with r value of 0.241.
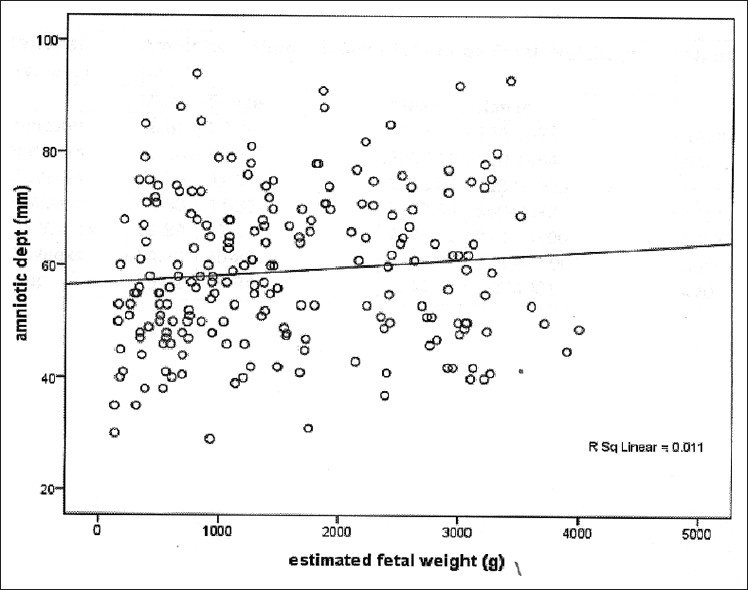
- Scatter diagram of the relationship between amniotic fluid index and estimated fetal weight.
DISCUSSION
Amniotic fluid disorders, oligo-hydramnios, and poly-hydramnios have been associated with intrauterine growth restriction and abnormal fetal growth, but this relationship across the entire range of FWs is unclear.[3] However, when used alone, amniotic fluid measurement has been found to perform poorly in predicting fetal distress, fetal growth restriction or low Apgar scores, among others. It also has a wide range of reference values.[6] Polyhydramnios and oligohydramnios could overestimate or underestimate sonographic FW assessment.[1] While there are reports of AFI measurements and ultrasound EFWs, as separate parameters, both in the Nigerian and international literature,[8–10] there are few reports that assessed the possible relationship between AFI and estimated weight, for both normal (non-diabetic) and diabetic pregnancies.[13611]
This study found a decrease in mean AFI values from 172.1 mm in early third trimester (27-29 weeks), to a value of 144.0 mm at 36-38 weeks, before a sharp drop to 125.0 mm at 39-40 weeks, as observed in previous studies.[811] As expected increase in FW was noticed throughout pregnancy, but there was no significant association between AFI and EFW when all the AFI and EFW pairs were considered (P > 0.05; r = 0.241). Only the AFI and EFW pair for gestation age 30-32 weeks showed any significant relationship; (P < 0.05). This lack of significant relationship between AFI and EFW across all gestational age strata is supported by the works of Perni et al., and Owen et al.[36] Possible reasons adduced for this are that swallowing and urinating mechanisms, rather than fetal size, are more involved in regulation of amniotic fluid volume. The implication of this is that fetal size may not need to be considered in variations of amniotic fluid volume across the gestational ages.
It is interesting to note that Kofinas and Kofinas[11] in 2012, found a significant relationship between AFI and EFW for both diabetic and non-diabetic pregnancies. While no explanation was offered for the former, it was postulated that fetuses of diabetic pregnancies spend more time breathing than swallowing; since swallowing and breathing are mutually exclusive, the fetuses do not swallow as much amniotic fluid as expected; thus in diabetic pregnancies, it may be necessary to consider fetal size when interpreting amniotic fluid variations across gestational ages.
This present report on relationship between amniotic fluid and estimated fetal weight is probably the first among pregnant women in Nigeria and therefore, raises the need for more studies on the subject, especially with larger sample sizes. It has nonetheless supported the majority of the views of similar works in the foreign literature that reported the non-dependence of amniotic fluid measurements on ultrasound estimated fetal size.
CONCLUSION
This study has produced a range of values of AFI and EFW among Nigerian Africans. However, no significant relationship exists between these parameters. The probable implication of this is neither parameter merits consideration when variations in the other are considered.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/2/106614
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- The effect of amniotic fluid index on the accuracy of sonographic estimated fetal weight. J Diagnostic Med Sonography. 2005;21:329-35.
- [Google Scholar]
- Correlation of sonographically estimated birth weight and actual birth weight among pregnant women at the University of Benin Teaching Hospital. National Postgraduate Medical College of Nigeria (FMCR) Dissertation 2011
- [Google Scholar]
- Association of amniotic fluid index with estimated fetal weight. J Ultrasound Med. 2004;23:1449-52.
- [Google Scholar]
- Ultrasound assessment of renal size in healthy term neonates: A report from Benin City, Nigeria. Saudi J Kidney Dis Transpl. 2007;18:277-81.
- [Google Scholar]
- Is there a relationship between fetal weight and amniotic fluid index? Ultrasound Obstet Gynecol. 2002;20:61-3.
- [Google Scholar]
- Amniotic fluid volume assessment with the four-quadrant technique at 36-42 weeks’ gestation. J Reprod Med. 1987;32:540-2.
- [Google Scholar]
- Sonographic assessment of normal amniotic fluid volume in pregnant Nigerian women. Trop J Obstet Gynaecol. 2007;24:39-44.
- [Google Scholar]
- The amniotic fluid index in normal human pregnancy. Am J Obstet Gynecol. 1990;162:1168-73.
- [Google Scholar]
- Assessment of amniotic fluid index in normal pregnancy at a tertiary care hospital setting. J Ayub Med Coll Abbottabad. 2009;21:149-51.
- [Google Scholar]
- Differences in amniotic fluid patterns and fetal biometric parameters in third trimester pregnancies with and without diabetes. J Matern Fetal Neonatal Med. 2006;19:633-8.
- [Google Scholar]




