
Translate this page into:
Novel case of coronary artery ectasia and myocardial bridging in one segment detected by coronary computed tomography angiography


*Corresponding author: Gabriel Czepe, Department of Radiology, Medical University of Lublin, Lublin, Poland. gabrielczepe@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Czepe G, Przybylski P, Czekajska-Chehab E. Novel case of coronary artery ectasia and myocardial bridging in one segment detected by coronary computed tomography angiography. J Clin Imaging Sci. 2025;15:1. doi: 10.25259/JCIS_149_2024
Abstract
Coronary artery ectasia (CAE) is defined as a dilation exceeding 1.5 times the diameter of an adjacent normal artery, predominantly affecting males. Myocardial bridging (MB) is a condition in which the coronary artery runs intramurally within myocardial tissue. Coronary computed tomography angiography (CCTA) offers high-resolution imaging, facilitating accurate diagnosis of these conditions. This report presents the first documented case of a 78-year-old female with CAE and superficial MB coexisting in the same segment of the left anterior descending artery that was detected incidentally by CCTA.
Keywords
Coronary artery ectasia
Myocardial bridging
Computed tomography angiography

INTRODUCTION
Coronary artery ectasia (CAE) is characterized by a coronary artery diameter that exceeds 1.5 times the largest diameter of an adjacent normal artery.[1] CAE is a rare condition, with prevalence rates varying between 1.2% and 7.4% across different studies. It predominantly affects males, with a predominance of approximately 90%.[2] Myocardial bridging (MB) is an anatomical phenomenon where a segment of the epicardial coronary artery follows a path within the myocardium. In coronary computed tomography angiography (CCTA), the prevalence of MB exhibits a wide range, spanning from 3.5% to as high as 58%.[3] CCTA demonstrates the highest concordance with pathological studies, making it currently the most reliable method for detecting MB prevalence.[4] Patients with both MB and CAE may experience the symptoms associated with coronary artery disease.[5] Although coronary angiography remains the gold standard for evaluating CAE, CCTA has proven to be highly useful in assessing this condition. The high-resolution imaging provided by CCTA allows for detailed visualization and accurate assessment, enhancing the overall diagnostic process.[1,2] This work aims to present a unique case of ectasia and MB occurring within a single segment, a phenomenon not previously documented in the available literature using CCTA.
CASE REPORT
A 78-year-old female patient, with a history of poor tolerance for physical exertion and intermittent dyspnea without chest pain, diabetes, heart failure, and arterial hypertension, was referred from the cardiology outpatient clinic to the Department of Radiology for CCTA. CCTA data were acquired using a retrospective electrocardiography (ECG)-gated cardiac computed tomography (CT) scan with a 256-row scanner (Revolution, General Electric Healthcare, Milwaukee Wisconsin, USA). The scan parameters included a tube voltage of 120 kV, 734 mA, and collimation of 256 × 0.625 mm with a cardiac axial spot, and a gantry rotation time of 0.28 s with electrocardiography (ECG)-dependent tube current modulation. The patient received an injection of iodine contrast agent Iomeron 400 with a total volume of 90 mL, followed by a 50-mL injection of saline solution, administered through an antecubital vein. Contrast material administration was monitored using bolus tracking in the ascending aorta, with manual selection of the scan delay using the SmartPrep technique. Image reconstruction comprised 10 series with a 10% R-R interval (5–95%). Data analysis was performed using dedicated workstation software (Advantage Workstation version 4.7, General Electric Healthcare, Milwaukee Wisconsin, USA). The examination revealed no atherosclerotic calcifications in the vessel walls. Minor mural changes were observed in both coronary arteries and their branches. The CCTA scan showed a superficial muscular bridge of the left anterior descending (LAD) artery in segment 7 (according to the Society of Cardiovascular CT) measuring 14 mm in length and 1.1 mm in thickness.[6] An irregular, gradual dilatation of the LAD over a length of 18.2 mm to a maximum diameter of 3.5 mm was observed. The diameter of the vessel before the ectatic segment was 2.1 mm and that after was 1.6 mm. The measured length of the LAD was 159 mm [Figure 1].
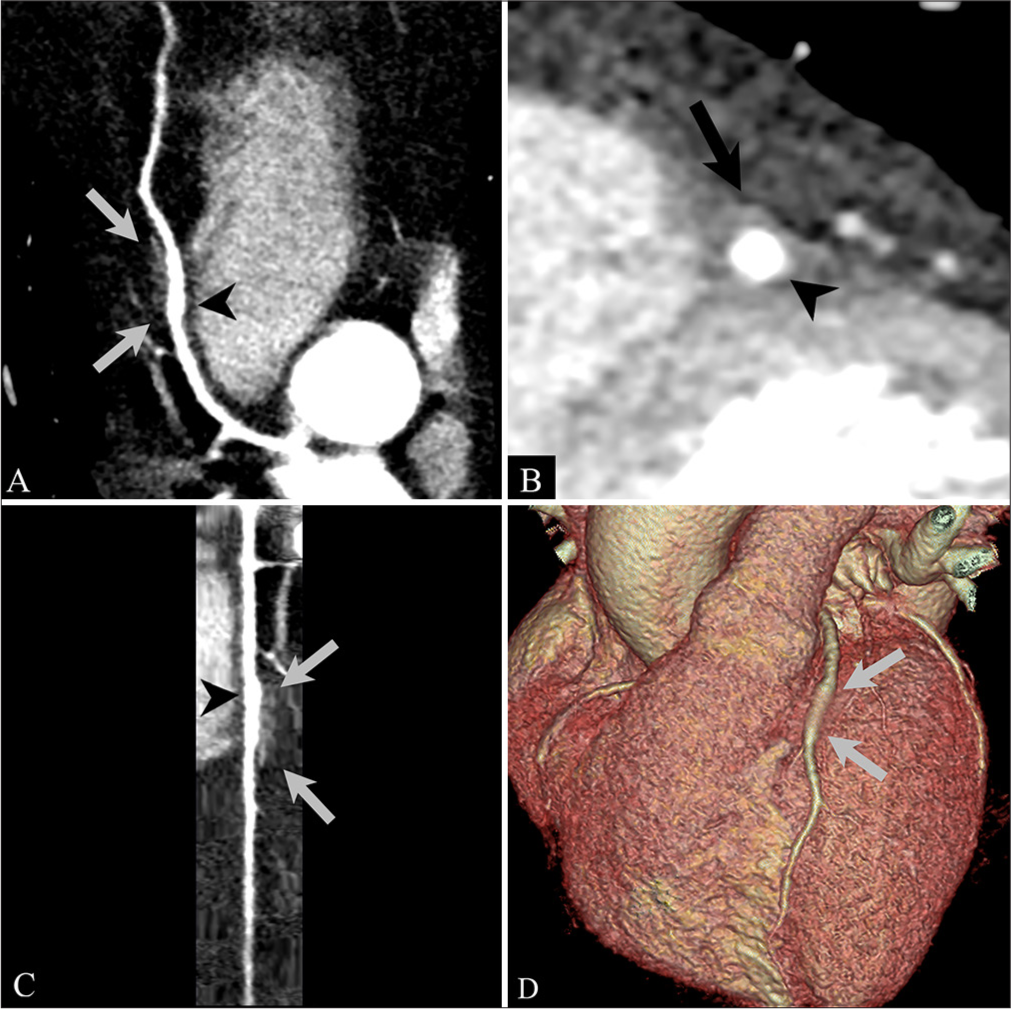
- (A-C) Curved planar reformat (CPR) images and (D) the three-dimensional volume-rendered (3D-VR) image. (A, C, D) The two gray arrows indicate the entrance and exit of the MB. (B) The black arrow points at the MB. (A-C) The black arrowhead points at ectasia.
Other significant findings were identified on CCTA: Slight hypokinesia of the apex and the anterior and mid-anteroseptal segments, accompanied by localized subendocardial perfusion defects. In addition, there were a few small fatty density foci in the wall of the right ventricle and the interventricular septum. Importantly, the patient did not have any other anatomical abnormalities.
DISCUSSION
There is no single, consistent definition distinguishing fusiform aneurysm from CAE. For instance, Markis et al. based on their work with coronary cineangiography, considered only saccular changes to be aneurysms.[7] There is currently no original work available that, based on CCTA, defines the differences between aneurysms and ectasias.
Markis et al. proposed a four-tier classification of CAE: Grade I – diffuse ectasia involving two or three vessels, Grade II – diffuse disease affecting one vessel with localized disease in another vessel, Grade III – diffuse ectasia of a single vessel only, and Grade IV – localized or segmental ectasia.[7]
At present, the pathogenesis of CAE remains incompletely understood, but there is some evidence indicating an atherosclerotic etiology as the most common cause in adults, where the most common cause in children and adolescents is Kawasaki disease.[1,4]
In the presented study, the patient had no significant atherosclerotic lesions (only minor mural changes), so other causes should be considered.
MB most commonly affects the LAD artery at a rate of 76.9%. The mid-segment of the LAD is the most frequent location of bridging, accounting for 46.7% of occurrences, followed by the distal LAD.[3] MB can present variations in depth, classified as superficial (>1 mm–2 mm), deep (≥2 mm), and very deep (≥5 mm).[3] Taking this into account, our case falls under Grade IV of the ectasia classification proposed by Markis et al. and it is also an example of superficial MB.[3,7]
There are no clear guidelines regarding the management of patients with CAE or MB. It depends on the underlying cause. According to the available literature, cases of MBs and CAE that produce clinical symptoms are initially treated conservatively, including risk factor modification, followed by pharmacological therapy. If such treatment proves unsuccessful, invasive procedures are considered.[1,8,9]
In the conducted CCTA, there were no signs of atherosclerotic calcifications in the walls of the coronary vessels, but even isolated CAE still presents a risk of myocardial ischemia and infarction.[8] In the case of MBs, they are mostly benign conditions; however, their significance is closely linked to other risk factors.[9] Due to the rarity of this phenomenon, the exact cause of the coexistence of these two conditions in the same segment of the coronary artery remains unknown. The only documented case we were able to find was detected during coronary angiography.[10]
CCTA provides detailed visualization without the need for invasive procedures, ensuring patient comfort while delivering accurate and reliable diagnostic results.[2]
Since no deterioration in the patient’s other known conditions, which could influence her symptoms, has been observed, it remains plausible that, despite their small dimensions, both the MB and CAE are contributing to the clinical presentation. The patient is currently under ongoing clinical observation at a cardiology outpatient clinic, where measures have been taken to modify risk factors and optimize treatment, including treatment of hypertension.
CONCLUSION
To the best of our knowledge, this is the first documented case of the coexistence of a MB and ectasia within the same coronary artery segment detected by CT and only the second case of this condition was reported overall. Due to the unique nature of these changes, the patient will be subject to continued observation to ascertain potential clinical implications. This ongoing monitoring aims to better understand the progression and possible consequences of the observed alterations, ensuring a comprehensive evaluation of the patient’s condition.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Myocardial bridging: Review on the role of coronary computed tomography angiography. J Clin Med. 2023;12:5949.
- [CrossRef] [PubMed] [Google Scholar]
- Coronary artery ectasia; Clinical updates and management options in acute presentation. Med Res Arch. 2017;5:5.
- [CrossRef] [Google Scholar]
- SCCT guidelines for the interpretation and reporting of coronary computed tomographic angiography. J Cardiovasc Comput Tomogr. 2009;3:122-36.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical significance of coronary arterial ectasia. Am J Cardiol. 1976;37:217-22.
- [CrossRef] [PubMed] [Google Scholar]
- Myocardial bridging: Diagnosis, functional assessment, and management: JACC state-of-the-art review. J Am Coll Cardiol. 2021;78:2196-212.
- [CrossRef] [PubMed] [Google Scholar]
- Coexistence of ectasia and myocardial bridge on the same coronary artery segment. Acta Med Anat. 2014;3:147-8.
- [CrossRef] [Google Scholar]




