
Translate this page into:
Littoral Cell Angioma of Spleen: An Uncommon Presentation of a Rare Neoplasm
Address for correspondence: Dr. Pramod Gupta, 2704, Oates Drive, Plano, TX 7509, USA. E-mail: pramodvagisha@hotmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Littoral cell angioma (LCA) is a rare primary splenic tumor that is difficult to differentiate preoperatively from other benign and malignant splenic lesions. Most of the cases present as multiple nodules in the spleen. We report a case of large solitary LCA of the spleen, an uncommon presentation. LCA should be considered in the differential diagnosis of multiple and solitary splenic lesions.
Keywords
Littoral cell angioma
neoplasm
spleen

INTRODUCTION

Littoral cell angioma (LCA) is a recently described rare primary vascular neoplasm, unique to the spleen. This neoplasm has characteristic morphological and immunophenotypic features that distinguish it from other vascular splenic tumors. Most of the cases described in the literature were LCAs composed of multiple nodules of variable sizes. We report a large solitary angioma in the spleen, an uncommon presentation of this rare neoplasm.
CASE REPORT
A 58-year-old female patient presented to her primary care physician with chronic non-specific bilateral lower rib pain. Her medical history included cholecystectomy for gall stones and gastroesophageal reflux disease. Her physical exam was normal at presentation. The chest radiographs showed a questionable opacity in the retrocardiac region near the diaphragm. Routine laboratory tests were normal including hemoglobin, hematocrit, white blood cell, and platelet count. A contrast-enhanced computed tomogram (CT) scan was performed during the portal venous phase, the retrocardiac opacity seen on the chest radiograph turned out to be hiatal hernia. The spleen was enlarged with a large 6.6 cm × 6.0 cm solitary mass [Figure 1]. There was diffuse, homogeneous enhancement on the lateral aspect of the mass and the medial aspect was hypoenhanced, probably due to a necrotic portion or a large nonenhanced vascular channel. To further characterize the mass, multiphasic magnetic resonance imaging (MRI) was performed. The MRI [Figure 2] showed the mass to be both T1 and T2 isointense with mild peripheral nodular and internal septal enhancement during the arterial phase with complete, diffuse, and mild enhancement of the mass during the portal venous phase, which remained enhanced until delayed images. The differential diagnoses considered were primary vascular neoplasms including atypical hemangioma (as mass was not T2 hyperintense), hamartoma, and potential angiosarcoma. The patient underwent laparoscopic splenectomy with morselization. Histological examination of the fragments of mass revealed anastomosing and congested sinusoidal channels with fibrous interstitial tissue and absence of normal red and white pulp. The lining cells were immunoreactive for CD 31, factor VIII, and CD 68, and were negative with stains for CD8 and CD34 (markers that are normally present on red pulp sinusoidal endothelium), consistent with diagnosis of LCA.
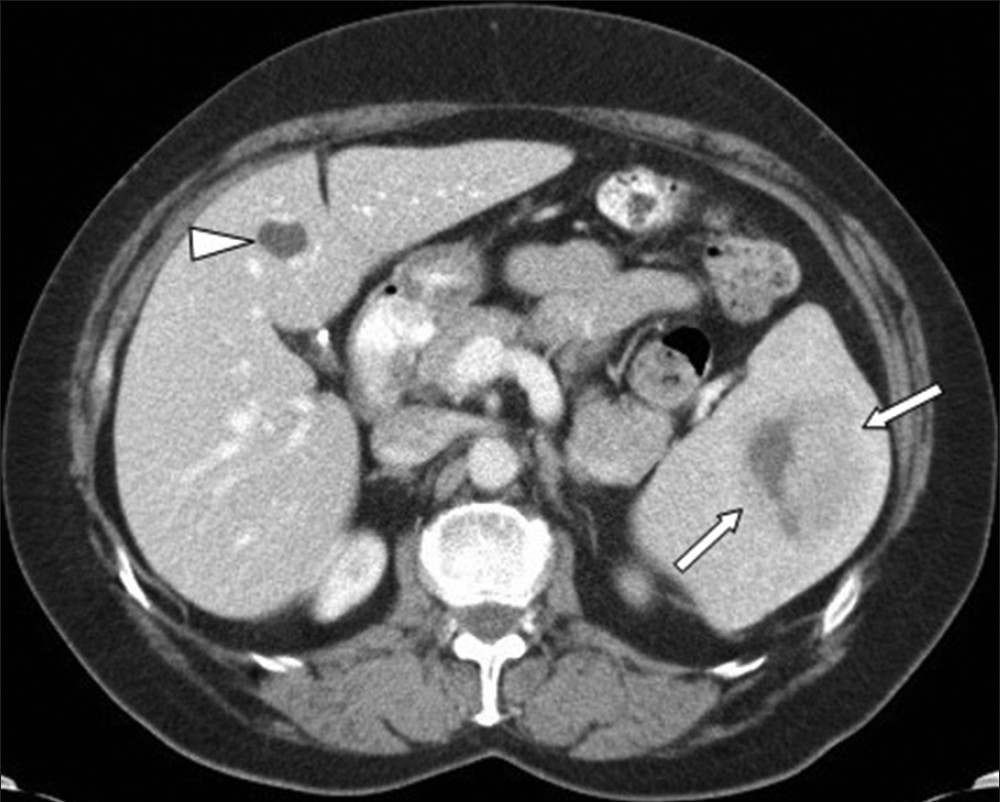
- Contrast-enhanced axial computed tomogram (CT) image obtained during portal venous phase shows a large mass (arrows) in the spleen, the mass is showing diffuse homogeneous enhancement on the lateral aspect and the medial aspect is hypoenhanced. A cyst in the liver is also demonstrated (arrowhead).
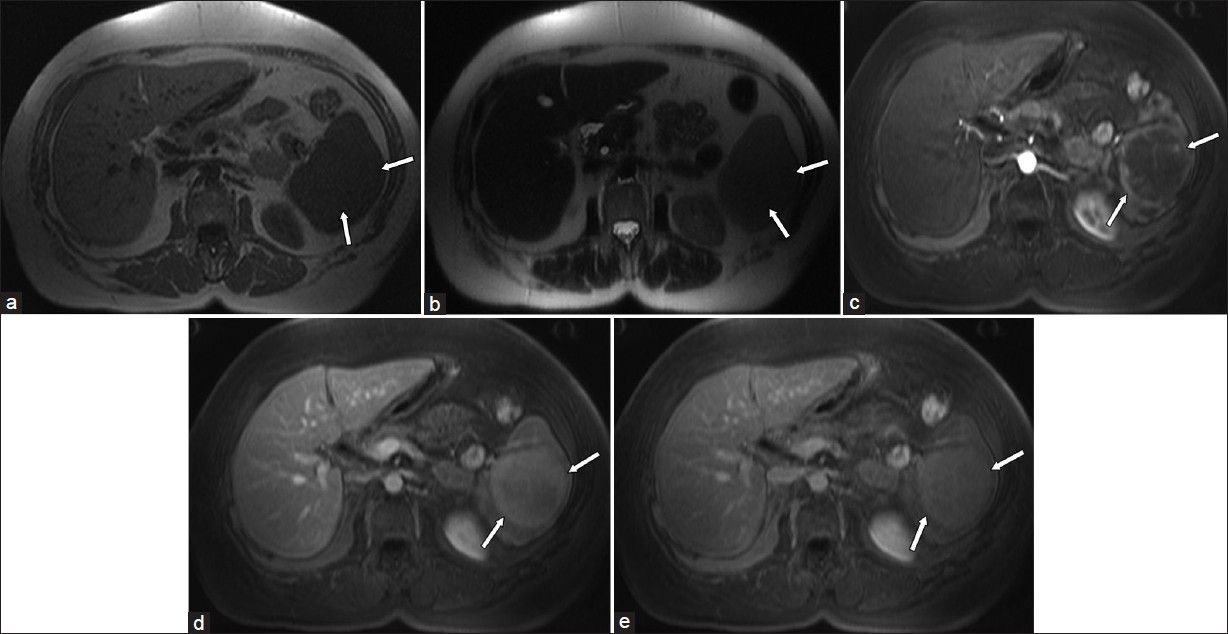
- Axial magnetic resonance imaging (MRI) images at the level of mid spleen show a large mass (arrows) which is isointense to the rest of splenic parenchyma before contrast injection on (a) T1-weighted and (b) T2-weighted images. (c) It shows peripheral nodular and internal septal enhancement during arterial phase on T1-weighted fat suppressed pulse sequence. (d) Diffuse enhancement during portal venous phase and (e) remains enhanced on delayed 3-min image.
The patient's postoperative course was uneventful. As 30% of LCA cases have been reported to be associated with other malignancies, she underwent further investigations including CT chest and colonoscopy, which were normal. Her clinical history has been uneventful over a 2-year follow-up period.
DISCUSSION
Primary vascular tumors of the spleen are uncommon. The differential diagnosis of splenic vascular tumor is broad and may represent benign (hemangioma, hamartoma, lymphangioma), indeterminate (LCA, hemangioendothelioma, hemangiopericytoma), or malignant neoplasms (angiosarcoma).[12] LCA is a rare and recently described vascular tumor of the spleen, first described by Falk et al., in 1991.[3] Since the initial description, there have been scattered case reports and a few case series of LCA.
Most of the cases of LCA described in the literature have been composed of multiple nodules of varying sizes in the spleen; solitary presentation is very rare. Out of not more than 75 cases reported in English literature so far, only five cases were of a solitary mass.[4–6]
LCA is considered a benign neoplasm arising from the littoral cells lining the sinuses of the red pulp in normal splenic tissue. Littoral cells possess morphologic and immunophenotypic features that reflect a dual endothelial and histiocytic potential of splenic sinus lining which are diagnostic traits for LCA. Morphological diagnosis is based on the presence of anastomosing vascular channels lined by tall endothelial cells, focal papillary fronds, and normal splenic sinuses at the periphery of the lesion. Immunohistochemically, in contrast to normal sinus endothelium, which only expresses factor VIII antigen and CD 8 positivity, LCA neoplastic cells exhibit positive staining for both endothelial (CD 31 and factor VIII) and histiocytic (CD 68 and lysozyme) antigens, and the complement receptors (CD 21 and CD 163). LCA cells are negative for CD 8, CD 34, and S-100 protein antigens.[346]
LCA has no particular gender or age predilection, although the median age in Falk et al.'s original study was 49 years.[3] The clinical presentation of LCA ranges from completely asymptomatic and discovered incidentally, such as in our case, to a constellation of signs and symptoms such as abdominal pain, vague constitutional symptoms, splenomegaly, and hypersplenism.[4]
Although first described as benign, a strong association has been shown between this neoplasm and a group of immunologic and oncologic entities. In approximately 36% of cases, LCA was accompanied by immunodysregulation, which included Crohn's disease, metabolic disorders, and congenital abnormalities.[7] In approximately 30% of the cases, LCA was associated with various malignancies including colorectal, renal, hepatocellular, pancreatic, lung, lymphoma, myelodysplastic syndrome, and aplastic anemia.[8] LCA has also been shown to exhibit malignant potential, although this is extremely rare. The two subtypes of LCA with malignant potential are described as “littoral cell angiosarcoma” and “littoral cell hemangioendothelioma.”[9] These LCA variants may present with distant metastasis several months after splenectomy. Histological evaluation reveals features consistent with LCA histopathology, as well as abnormal architecture, nuclear atypia, and necrosis.
The pathogenesis of LCA remains unclear, but given its association with autoimmune disorders such as Crohn's disease, an immune system dysfunction has been postulated as a possible important pathologic mechanism. Indeed, immune system dysfunction may explain the association of LCA with other cancer types. These observations have prompted recommendations to closely evaluate and provide surveillance to patients with LCA for the development of other malignancies.[4]
Radiologically, LCA may be evaluated by several imaging modalities such as ultrasound (US), CT, MRI, or nuclear medicine studies (Tc-99m-labeled RBC scintigraphy). The sonographic appearance of LCA is variable and includes reports of mottled echotexture without discrete lesions, as well as findings of isoechoic, hypoechoic, and hyperechoic lesions.[24610] Color flow Doppler imaging may reveal the presence of central and peripheral vascularity that helps distinguish between LCA and cavernous hemangioma of spleen.[10] On noncontrast CT, LCA appears as hypoattenuating masses; given the vascular nature of these neoplasms, they tend to enhance homogeneously with contrast, particularly on delayed images. CT findings of surrounding capsule and internal calcification have not been described.[24–6] On MRI, a minority of cases may be hypointense on both T1-weighted and T2-weighted scans because of the hemosiderin content of the tumor. However, no significant siderosis is seen in more than 50% of the cases and lesions tend to be hyperintense on the T2-weighted images.[4] Nuclear medicine studies with Tc-99m-labeled RBC scintigraphy can be useful to differentiate splenic lesions from splenic hemangiomas. However, the radiologic features of LCA are rarely diagnostic as many other splenic neoplasms such as hamartomas, hemangiomas, lymphomas, metastatic diseases, and infectious diseases exhibit similar imaging characteristics.[15] The definitive diagnosis is made on histology and confirmed with immunohistochemistry.
Symptomatic LCA is often relieved by splenectomy, and given the association of LCA with other malignancies and reported cases of malignant transformation, splenectomy is both diagnostic and therapeutic.[6]
CONCLUSION
In conclusion, LCA is a recently described rare primary benign vascular neoplasm of the spleen that may be associated with other malignancies and may itself also have malignant potential. A majority of LCAs are multinodular, although some may present as solitary lesion, as in our case. LCA should be considered in the differential diagnosis of multiple or solitary splenic lesions.
ACKNOWLEDGMENT
The authors gratefully acknowledge the assistance of Francisco Garcia-Morales, MD, in the preparation of this manuscript.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/69/104302
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- From the archives of the AFIP: Primary vascular neoplasms of the spleen: Radiologic-pathologic correlation. Radiographics. 2004;24:1137-63.
- [Google Scholar]
- Littoral cell angioma of the spleen: Imaging features. AJR Am J Roentgenol. 2000;174:467-9.
- [Google Scholar]
- Littoral cell angioma. A novel splenic vascular lesion demonstrating histiocytic differentiation. Am J Surg Pathol. 1991;15:1023-33.
- [Google Scholar]
- Littoral cell angioma, a rare cause of long standing anaemia: A case report. Cases J. 2009;2:9115.
- [Google Scholar]
- Littoral cell angioma of the spleen in a patient with Gaucher disease. Am J Hematol. 2001;68:61-2.
- [Google Scholar]
- Littoral cell angioma of the spleen: An additional report of four cases with emphasis on the association with visceral organ cancers. Tumori. 1998;84:595-9.
- [Google Scholar]
- Littoral cell angiosarcoma: A truly malignant tumor. Am J Surg Pathol. 2004;28:1255.
- [Google Scholar]
- Littoral cell angioma: Sonographic and color Doppler features. J Ultrasound Med. 2007;26:539-42.
- [Google Scholar]




