
Translate this page into:
Incidentally Detected Mediastinal Vascular Anatomical Variants on PET-CT: A Pictorial Essay
Address for correspondence: Dr. Kathyayini Gopalkishna Murthy Paidipati, Department of Radiology, American Oncology Institute and Citizens Hospitals, Nallagandla, Hyderabad - 500 019, Andhra Pradesh, India. E-mail: kathybmc@yahoo.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Positron emission tomography with computed tomography (PET–CT) is an integral part of oncology practice in the current-day scenario. The hybrid anatomical and metabolic imaging information in this imaging modality provides access to a wealth of incidental findings which can have implications in the management of the patient, especially when surgical options are being considered. In this pictorial essay, we present incidentally detected mediastinal vascular anomalies on PET–CT, along with a review of associated literature.
Keywords
Incidental
mediastinum
positron emission tomography–computed tomography
vascular anomalies

INTRODUCTION

Positron emission tomography (PET) imaging has become an indispensable modality in current oncology practice. From the initial days of stand-alone PET imaging, this modality has now transformed into a hybrid or fusion imaging modality where anatomical information from computed tomography (CT) or from magnetic resonance imaging (MRI) is fused with the metabolic data obtained from tracers used. This helps in better understanding of the underlying pathology, thereby increasing the overall specificity.
The integrated anatomical information in the fused imaging provides additional data to the interpreting physician. This includes incidental findings which might not be directly related to the malignancy being evaluated but might assume significance in patient management, especially when surgical options are being considered. The recognition of such changes is essential for the physician. Through this compilation of cases, we attempt to describe both the normal vascular anatomy of the mediastinum on CT and pictorial presentation of incidentally encountered mediastinal vascular anatomical variants in patients undergoing PET–CT.
With the widespread use of PET–CT in the evaluation of various malignancies and non-malignant pathologies and the use of intravenous contrast in these studies, the understanding of the different vascular anatomic variants has become important for interpreting physicians.
A thorough knowledge of mediastinal vascular anatomy is essential in identifying various vascular anomalies. At the time of interpretation, it is not only necessary to consider the various anatomic variants that may occur but also to have knowledge of their different classifications, associated symptoms, and related anomalies [Table 1]. Ignorance of these vascular variants may lead to unnecessary examinations and may even have medico-legal implications.
The minor disadvantage with our series is that the imaging was done as a standard in the portal venous phase with a delay of 40–50 s, which may not be ideal to demonstrate most of the thoracic vessel abnormalities.
AORTIC ARCH ANOMALIES
Right aortic arch
This is a congenital malformation occurring during embryologic development as a consequence of a complete obliteration of the left fourth aortic arch and the left dorsal aorta.[12]
Right aortic arch (RAA) [Figure 1] is a rare and asymptomatic entity that is usually diagnosed incidentally.

- 60-year-old female with malignant melanoma. Axial non-contrast CT image shows right-sided aortic arch with aberrant origin of left subclavian artery (arrow).
RAA has been classified into three major subgroups:[3]
-
RAA with an aberrant left subclavian artery
-
RAA with mirror-image branching of the major arteries
-
RAA with the left subclavian artery isolated from the arch.
The RAA with aberrant left subclavian artery is the most common subtype and usually exists as an isolated anomaly.[4] It results from interruption of the left arch between the left common carotid and the left subclavian arteries in the hypothetical double aortic arch. In this subgroup, four vessels arise from the right arch in the following order: Left common carotid artery, right common carotid artery, a right subclavian artery, and an aberrant left subclavian artery. The proximal portion of the embryological left arch forms the left common carotid artery and the distal portion of the left arch may persist as the diverticulum of “Komerell”.[5]
The left subclavian artery arises from this aortic diverticulum at the junction of the arch and the descending thoracic aorta. This can be a cause of dysphagia in adults.
Double aortic arch
In a double aortic arch, the ascending aorta divides into two separate arches. The left or anterior arch has a course similar to that of the normal left aortic arch (LAA), and the right or posterior arch has a course to the left behind the esophagus and joins the left arch.[6] The descending aorta is usually on the left side. The subclavian and carotid arteries arise from their respective arches.
A double aortic arch completely encircles the trachea and esophagus by connecting segments of the arch and its branches. Thus, it is an example of a vascular ring and can cause dysphagia (dysphagia lusoria) or dyspnea and stridor.
Aberrant right subclavian artery
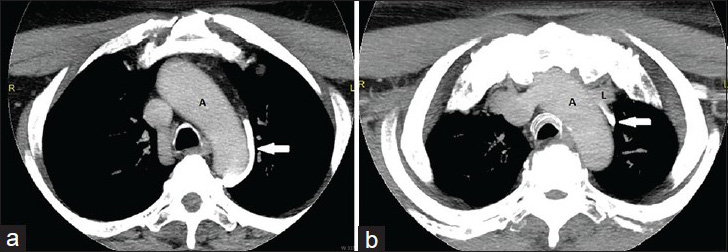
Aberrant right subclavian artery is the most common arch anomaly with an incidence of 0.5–2%.[3] It is a distal branch arising from an otherwise normal aortic arch. It courses behind the trachea and esophagus, crossing the mediastinum obliquely from left to right [Figures 2 and 3]. When ectatic, it can be a cause of dysphagia (dysphagia lusoria).

- 45-year-old male with carcinoma left lung. Axial contrast-enhanced CT (CECT) image shows aberrant right subclavian artery (arrow) coursing posterior to the trachea and esophagus. Also note changes of left pneumonectomy.

- 19-year-old female with adrenal neuroblastoma. Axial contrast-enhanced CT (CECT) image displays aberrant right subclavian artery (arrow) arising distal to the left subclavian artery and coursing posterior to the esophagus (E). T = Trachea
Common origin of bilateral carotid arteries
This is the most common variant of aortic arch branching. Here, the left common carotid artery has a common origin with the innominate artery.[7] Rather than arising directly from the aortic arch as a separate branch, the left common carotid artery origin is moved to the right and merges with the origin of the innominate artery [Figure 4]. The most common aortic arch branching pattern found in humans has separate origins for the innominate, left common carotid, and left subclavian arteries.
- 68-year-old paient with gallbladder carcinoma. Oblique multiplanar reconstruction (MPR) image demonstrates common origin (arrow) of bilateral common carotid arteries (CCAs). R = Right CCA, L = Left CCA
Aortic coarctation
This anomaly is characterized by narrowing at the junction of the distal arch of aorta and descending aorta. It can be associated with bicuspid aortic valve (75%), cerebral aneurysms (5–10%), and Turner syndrome (20% have coarctation).[8]
PULMONARY ARTERY ANOMALIES
Pulmonary artery anomalies are of three types: Pulmonary agenesis, pulmonary sling, and patent ductus arteriosus.
In pulmonary agenesis, there is unilateral absence of the main pulmonary artery with either complete or near-complete absence of lung parenchyma. This deficiency is overcome by compensatory hyperinflation of the contralateral lung.[8]
The term “pulmonary sling” is used when the left pulmonary artery take an abnormal origin from the right pulmonary artery and courses between the trachea and esophagus, thereby causing compression of the right main bronchus.
The ductus arteriosus shunts blood from the right ventricle to the aorta during intra-uterine life and usually closes after birth. Its persistence after 2 weeks results in a patent ductus arteriosus, which can lead to pulmonary arterial hypertension, if left uncorrected.
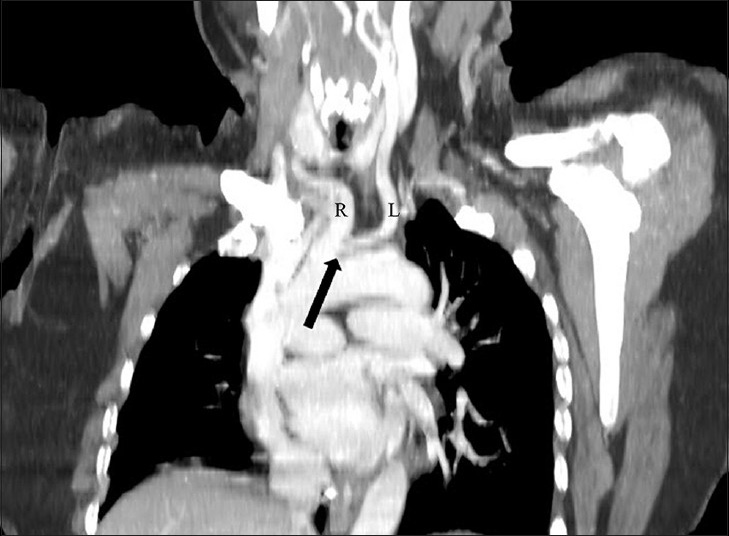
PULMONARY VENOUS ANOMALIES
Partial anomalous pulmonary venous connection
Partial anomalous pulmonary venous connection (PAPVC) is a congenital anomaly of pulmonary veins that drain into the systemic veins. In this anomaly, the blood from anomalous pulmonary vein drains into the systemic circulation, creating a right to left shunt. The anomalous veins drain into the following structures:[8]
-
Right upper lobe: Usually drains into the superior vena cava (SVC) and is associated with sinus venosus type of ASD atrial septal defect
-
Right lower lobe: Usually drains into the inferior vena cava (IVC), sometimes into the portal or hepatic vein; this can be an isolated finding or may be combined with pulmonary hypoplasia (Scimitar syndrome)
-
Left upper lobe: Drains into the brachiocephalic vein (isolated finding) [Figure 5]
-
Left lower lobe: This is a rare entity.
- 59-year-old female with endometrial carcinoma. (a) Oblique multiplanar reconstruction (MPR) image and (b) volume-rendered (VR) image demonstrate the left upper lobe pulmonary vein (arrow) draining into the left brachiocephalic vein.
Scimitar syndrome
Also known as pulmonary veno-lobar syndrome, Scimitar syndrome is characterized by hypoplastic right pulmonary artery and right lung, anomalous systemic arterial supply to the right lung, and an anomalous right pulmonary vein which drains into the inferior vena cava. This abnormal vein has been described as a “Scimitar” owing to is resemblance to Middle Eastern sword.[9]
SYSTEMIC VENOUS ANOMALIES
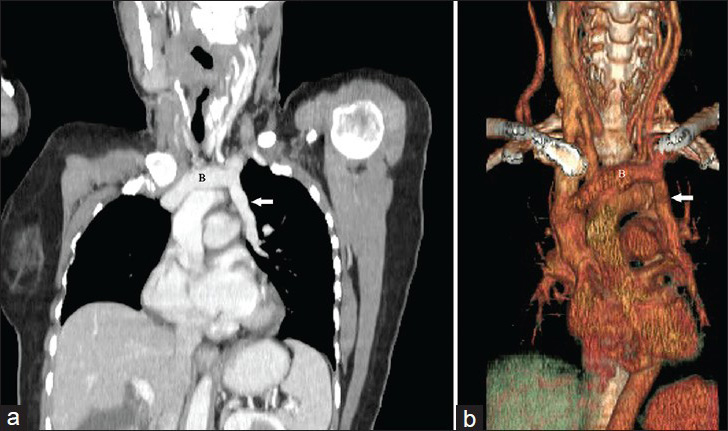
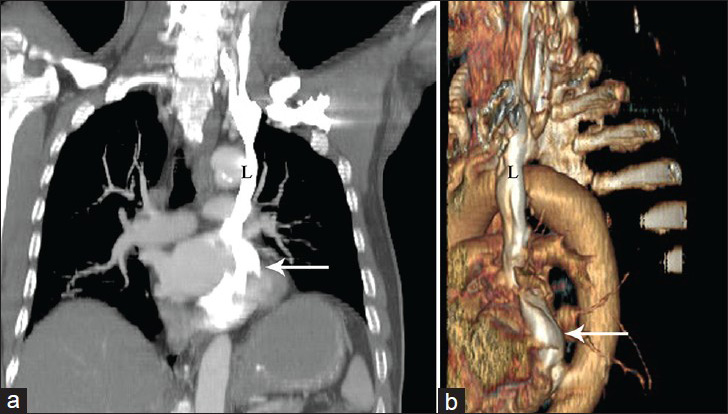
Persistent left SVC
Persistent left SVC (PLSVC) [Figures 6 and 7] is the most common congenital thoracic venous anomaly with a prevalence of 0.3–0.5% in the general population.[10]
- 66-year-old male with cholangiocarcinoma. (a) Oblique coronal maximum intensity projection (MIP) image and (b) volume-rendered (VR) and VR image demonstrate a persistent left superior vena cava (L) draining into the coronary sinus (arrow).
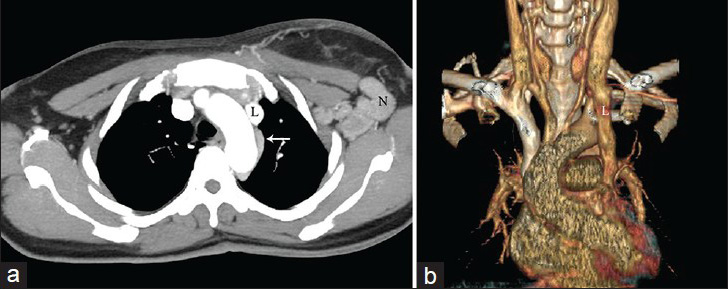
- 47-year-old female with carcinoma breast. (a) Axial maximum intensity projection (MIP) and (b) volume-rendered (VR) images demonstrate persistent left superior vena cava (SVC) (L). On the axial image, a left hemi-azygous vein (arrow) is noted draining into the left SVC. Also seen are enlarged left axillary lymph nodes (N).
The embryonic venous system in the thorax comprises a pair of superior cardinal veins (which drain the cranial portion of the embryo) and a pair of inferior cardinal veins (which drain the caudal portion of the embryo). Both pairs of veins join to form right and left common cardinal veins before entering the embryological heart. During the 8th week of gestation, an anastomosis forms between the right and left superior cardinal veins, resulting in the formation of innominate (or brachiocephalic) vein. Normally, the caudal portion of the left superior cardinal vein caudal to the innominate vein regresses to become the “ligament of Marshall”. If this fails to occur, a PLSVC is formed which empties into the coronary sinus. In such a situation, the bridging innominate vein may or may not degenerate.[11]
The most common subtype of PLSVC results in the presence of both left and right SVCs. Very rarely, however, the caudal portion of the right superior cardinal vein may regress leading to PLSVC with absence of right SVC.
A large majority of patients with PLSVC can have a variety of associated cardiac anomalies,[1213] such as atrial septal defect, bicuspid aortic valve, coarctation of aorta, coronary sinus ostial atresia, and cor triatriatum. Associated anomalies are more common with concomitant absence of right SVC. PLSVC has also been linked with anatomical and architectural abnormalities of the sinus node and conduction tissues.[14]
PLSVC has important implications when the left subclavian vein is used for access to the right side of the heart or pulmonary vasculature.[11] Its presence can make some procedures like Swan-Ganz catheter placement, permanent pacemaker and implantable cardioverter defibrillator (ICD) placement difficult.
PAPVC versus PLSVC
It is essential to differentiate PAPVC of the left upper lobe from PLSVC, as both entities can appear similar on CT. In both these anomalies, an anomalous vertically oriented structure is seen to the left of the aortic arch. This can be done by observing the drainage pattern of the anomalous vein as well.[15] In PAPVC, the anomalous vein drains the blood from the left upper lobe into the left innominate vein (which can appear enlarged at times). On the other hand, in PLSVC, the duplicated left SVC drains via the coronary sinus (which can appear enlarged) into the right atrium. Usually at the level of the left main bronchus, only the left superior pulmonary vein is seen anteriorly. However, in PSLVC, two vascular structures, namely, the normal left superior pulmonary vein and the left SVC are appreciated ventral to the left main bronchus.[16] This differentiation is clinically relevant as a PAPVC can become symptomatic if the right lung is diseased or in cases of right pneumonectomy.[17] Another important entity to be considered in the differentials is the “levoatriocardinal vein”, which was first described by Edwards and DuShane as a vein connecting the right superior vena cava and the left atrium.[18] This vascular anomaly is usually associated with left heart hypoplasia. Identifying the origin of this anomalous vein can differentiate it from PAPVC.
Left superior intercostal vein
The left superior intercostal vein drains blood from left second to fourth intercostal veins, passes lateral to the aortic arch, and then empties into the left brachiocephalic vein [Figure 8]. Its appearance on chest radiographs has been described as an “aortic nipple”. Its normal diameter on erect radiographs and supine radiographs is 4.5 mm and 5.5–6.5 mm, respectively. Dilatation of the superior intercostal vein is observed in SVC or IVC obstruction, congestive cardiac failure, portal hypertension, Budd–Chiari syndrome, and hypoplasia of the left brachiocephalic vein.[19]
- 45-year-old male patient with carcinoma tongue. (a and b) Axial contrast-enhanced CT (CECT) maximum intensity projection (MIP) images demonstrate the left superior intercostal vein (arrow) coursing along the arch of aorta (A) to drain into the left brachiocephalic vein (L).
Azygous continuation of IVC
Here, the IVC is interrupted above the level of the renal veins and continues as the azygous vein. This anomaly is associated with congenial heart disease and can be a part of polysplenia syndrome.
MISCELLANEOUS
Azygous lobe
The azygous lobe is a normal variant that is found in about 0.4% of chest radiographs.[20] It occurs when the right posterior cardinal vein, one of the precursors of the azygous vein, fails to migrate over the apex of the lung and penetrates it instead, carrying along pleural layers that entrap a portion of the right upper lobe. Two folds of parietal and two folds of visceral pleura form a mesentery-like structure, containing in its lowermost portion the azygous arch [Figure 9]. The enclosed lung (azygous lobe) is not an independent segment and its bronchial and arterial supplies arise from the apical or posterior segments of the right upper lobe.
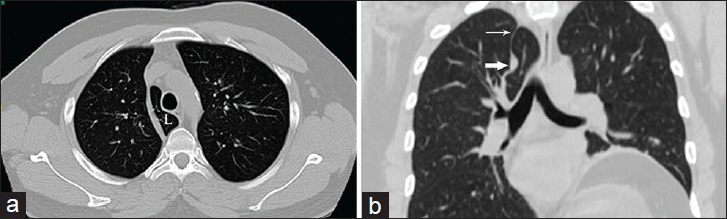
- 40-year-old male patient with laryngeal carcinoma. (a) Axial non-contrast CT (NCCT) lung window image demonstrates the azygous lobe (L). (b) Coronal NCCT lung window image displays the entrapped vein in cross section (bold arrow with pleural layers forming a sling (thin arrow).
Bronchial arteries and aorto-pulmonary collaterals
The lungs have dual vascular supply from pulmonary arteries and bronchial arteries. The former serve the purpose of gas exchange, while the latter provide nutrition.[21] The bronchial arteries usually arise from the descending thoracic aorta at the T5 and T6 vertebral levels and are described as orthotopic. They are referred to as ectopic when they arise at a different level of the descending aorta or from its branches. Irrespective of their origin, the bronchial arteries enter the lung parenchyma through the hilum and follow the course of bronchi. On CT, their normal diameter in adults is less than 1.5 mm at their origin and a diameter of 2 mm or more is considered abnormal.[2223] Enlarged bronchial arteries are usually a consequence of pulmonary vascular disease (like chronic thromboembolism or vasculitis), chronic inflammatory lung disease, and neoplastic diseases. The most common locations of enlarged bronchial arteries are retroesophageal, retrotracheal, and retrobronchial areas, as well as the posterior wall of the main bronchus and the aorticopulmonary window.[23]
On the other hand, aorto-pulmonary collateral blood vessels (APCs) arise from the systemic arteries and supply blood to pulmonary circulation. They usually arise from the descending aorta, subclavian artery branches, and bronchial and intercostal arteries. However, unlike bronchial arteries, they supply blood to terminal respiratory units and may have a course away from the bronchial tree. They are most often associated with cyanotic congenital heart diseases, particularly tetralogy of Fallot with pulmonary valve atresia where APCs compensate for the decreased pulmonary vascular supply.[24] They also accompany single-ventricle heart disease.
CONCLUSION
Vascular anatomical variants are incidentally found with relative frequency on imaging studies including PET–CT. Knowledge of mediastinal vascular anomalies may lead to search for other associated anomalies and has an impact on the surgical management of patients. Interpreting these anomalies is, therefore, of significance for the imaging physicians.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2015/5/1/19/154353
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- A right-sided aortic arch and aberrant left subclavian artery with proximal segment hypoplasia. Interact Cardiovasc Thorac Surg. 2012;14:370-1.
- [Google Scholar]
- An Atlas of Vascular Rings and Related Malformations of the Aortic Arch System. Springfield, Illinois: Charles C Thomas Publisher; 1964. p. :8-13. 124-31
- [Google Scholar]
- Right aortic arch: Plain film diagnosis and significance. Am J Roentgenol Radium Ther Nucl Med. 1966;97:377-89.
- [Google Scholar]
- Verlagerung des Ösophagus durch eine abnorm verlaufende Arteria subclavia dextra (Arteria lusoria) Fortschr Geb Roentgenstrahlen. 1936;54:590-5.
- [Google Scholar]
- Congenital anomalies of the aortic arch: Evaluation with the use of multidetector computed tomography. Korean J Radiol. 2009;10:176-84.
- [Google Scholar]
- Bovine Aortic Arch Variant in Humans: Clarification of a Common Misnomer. In: AJNR Am J Neuroradiol. Vol 27. 2006. p. :1541-2.
- [Google Scholar]
- Vascular Anomalies of Aorta, Pulmonary and Systemic Vessels. St. Louis, USA, Leiderdorp: The Radiology Assistant (Cardiovascular). Mallinckrodt Institute of Radiology, Washington University School of Medicine, Rijnland Hospital; 2007.
- [Google Scholar]
- Disease of Heart and Circulation. (2nd ed). Philadelphia: JB Lippincott; 1956. p. :457-8.
- [Google Scholar]
- Persistent left superior vena cava: A case report and review of literature. Cardiovasc Ultrasound. 2008;6:50.
- [Google Scholar]
- Persistent left superior vena cava: Case report and literature review. Respir Care. 2000;45:411-6.
- [Google Scholar]
- Persistent left superior vena cava; survey of world literature and report of thirty additional cases. Angiology. 1954;5:90-132.
- [Google Scholar]
- XVIII. Persistent fetal dispersion of the atrioventricular node and His bundle within the central fibrous body. Circulation. 1976;53:1026-34.
- [Google Scholar]
- Partial anomalous pulmonary venous drainage of the left upper lobe vs duplication of the superior vena cava: Distinction based on CT findings. AJR Am J Roentgenol. 1993;160:375-9.
- [Google Scholar]
- CT appearance of persistent left superior vena cava, anomalous right superior pulmonary venous return into the right-sided superior vena cava and a sinus venosus-type atrial septal defect. Br J Radiol. 2009;82:e235-9.
- [Google Scholar]
- An anatomic survey of anomalous pulmonary veins: Their clinical significance. J Thorac Surg. 1952;23:433-44.
- [Google Scholar]
- Thoracic venous anomalies. I. Vascular connection between the left atrium and the left innominate vein (levoatriocardinal vein) associated with mitral atresia and premature closure of the foramen ovale (Case 1). II. Pulmonary veins draining wholly to the ductus arteriosus (Case 2) Arch Pathol. 1950;49:517-37.
- [Google Scholar]
- The normal and abnormal left superior intercostal vein. AJR Am J Roentgenol. 1978;131:599-602.
- [Google Scholar]
- The azygous arch: Normal and pathologic CT appearance. AJR Am J Roentgenol. 1982;139:477-83.
- [Google Scholar]
- Anatomy of the normal bronchial circulatory system in human and animals. In: Butler J, ed. The Bronchial Circulation. New York, NY: Marcel Dekker; 1992. p. :45-77.
- [Google Scholar]
- Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: A comprehensive review. Radiographics. 2002;22:1395-409.
- [Google Scholar]
- Prevalence and risk factors for aortopulmonary collateral vessels after Fontan and bidirectional Glenn procedures. J Am Coll Cardiol. 1993;22:207-15.
- [Google Scholar]




