
Translate this page into:
Gastroepiploic artery embolization for splenic trauma in a liver transplant recipient

*Corresponding author: Rooshi Parikh, School of Medicine, City University of New York, New York, United States. rparikh000@citymail.cuny.edu
-
Received: ,
Accepted: ,
How to cite this article: Parikh R, Epstein SB. Gastroepiploic artery embolization for splenic trauma in a liver transplant recipient. J Clin Imaging Sci. 2025;15:18. doi: 10.25259/JCIS_3_2025
Abstract
The spleen is a highly vascular organ susceptible to injury in blunt abdominal trauma, often leading to massive blood loss. Splenic artery embolization (SAE) has been shown to be a safe and effective nonoperative approach in cases of hemodynamically stable patients with blunt splenic trauma. SAE can be performed proximally or distally, with both approaches demonstrating similar clinical efficacy. This case report describes emergent splenic embolization for acute abdominal trauma in a liver transplant recipient. However, due to the presence of prior splenic artery ligation, a uniquely alternative route through the gastroepiploic artery was used to gain access to the spleen for embolization.
Keywords
Blunt abdominal trauma
gastroepiploic artery
liver transplant
splenic artery embolization

INTRODUCTION
Blunt abdominal trauma can result in clinically significant visceral organ injuries of which the spleen is most commonly affected. Traditional management options for splenic trauma include observation, splenectomy, and splenic artery embolization (SAE). Nonoperative management is preferred for hemodynamically stable patients while splenectomy may be indicated in hemodynamically unstable patients.[1-4] SAE is an alternative nonoperative modality. SAE can be performed proximally or distally, with proximal SAE offering lower rates of splenic infarction and shorter procedure times but complicating future coaxial interventions, while distal SAE improves splenic salvage in cases of focal injury but increases infarction risk.[2-5]
In liver transplant patients, managing splenic injury can be more complex due to altered vascular anatomy. Splenic artery steal syndrome (SASS) is a rare but severe complication seen after liver transplantation where shunting of blood from the hepatic artery to the splenic artery leads to hepatic hypoperfusion and potential graft dysfunction. Splenic artery ligation is sometimes performed prophylactically to prevent SASS, but this can complicate future interventions, as seen in this case.[6,7]
This case report describes emergent splenic embolization through gastroepiploic artery (GEA) in a liver transplant recipient with previous splenic artery ligation following acute trauma.
CASE REPORT
A 30-year-old male with history of an orthotopic liver transplant and a combined kidney and second liver transplant presented to the emergency department following a motorcycle accident. On initial assessment, he was alert and oriented, complaining of right shoulder and left chest pain. His blood pressure (BP) dropped to 84/47 mmHg, and heart rate (HR) rose to 114 beat/min.
A focused assessment with sonography in trauma (FAST) scan revealed free fluid. After receiving blood products, BP stabilized at 123/83 mmHg, although HR remained between 110 and 119 beat/min. He was taken for computed tomography (CT) scan which demonstrated a Grade 5 splenic laceration with hemoperitoneum [Figure 1], multiple left rib fractures, and left scapular fractures. Despite previous splenic artery ligation, the entire artery was patent, evidenced by contrast opacification. In addition, a largely hypertrophied GEA was noted [Figure 2]. Interventional radiology was consulted for emergent embolization.
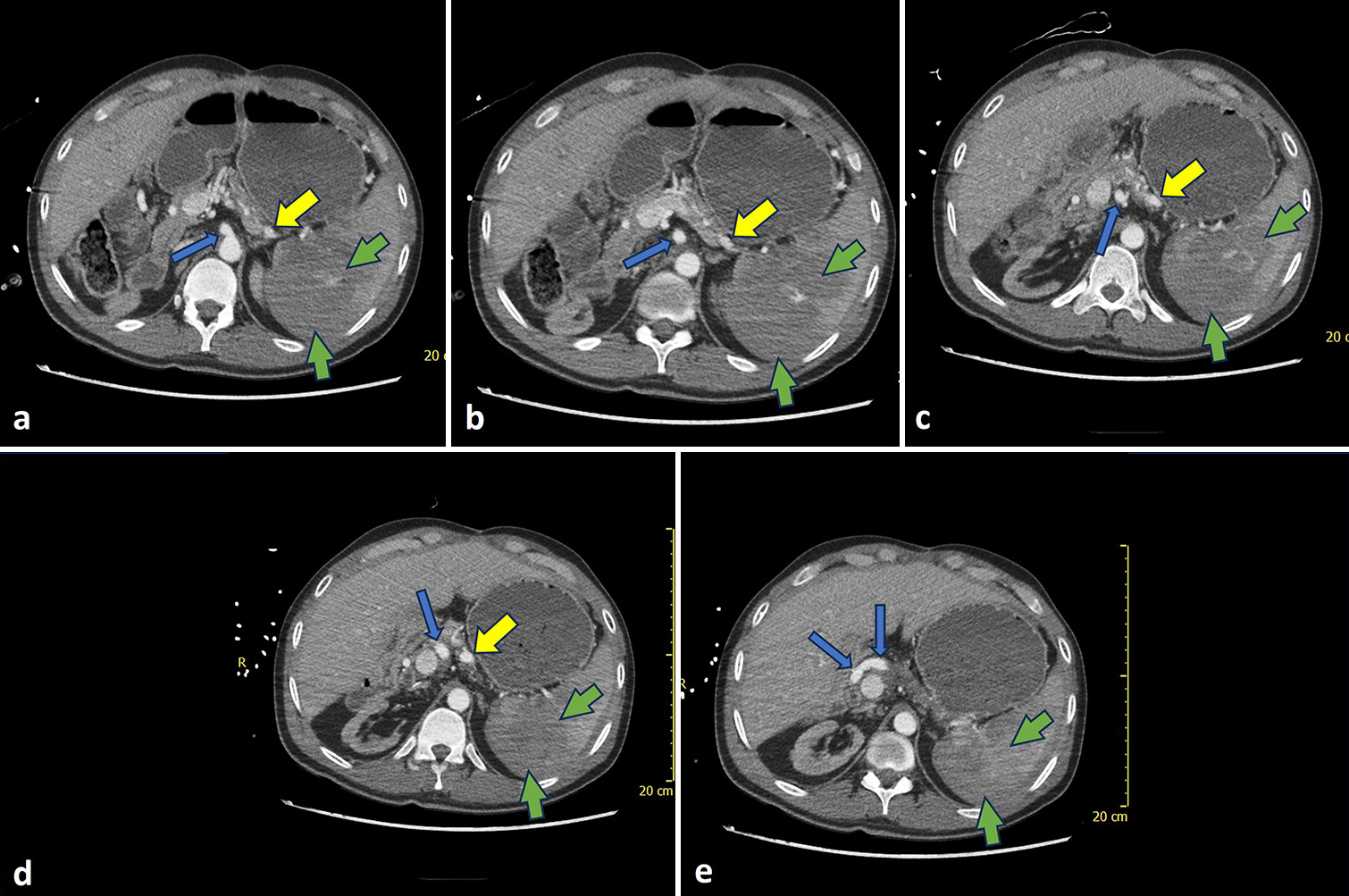
- A 30-year-old male presented with chest and shoulder pain after motorcycle accident. (a-e) Axial CT slices demonstrate Grade V subcapsular splenic lacerations (green arrows) following blunt trauma with common hepatic artery (blue arrows) originating from celiac axis while splenic artery (yellow arrows) has been proximally ligated but still patent.
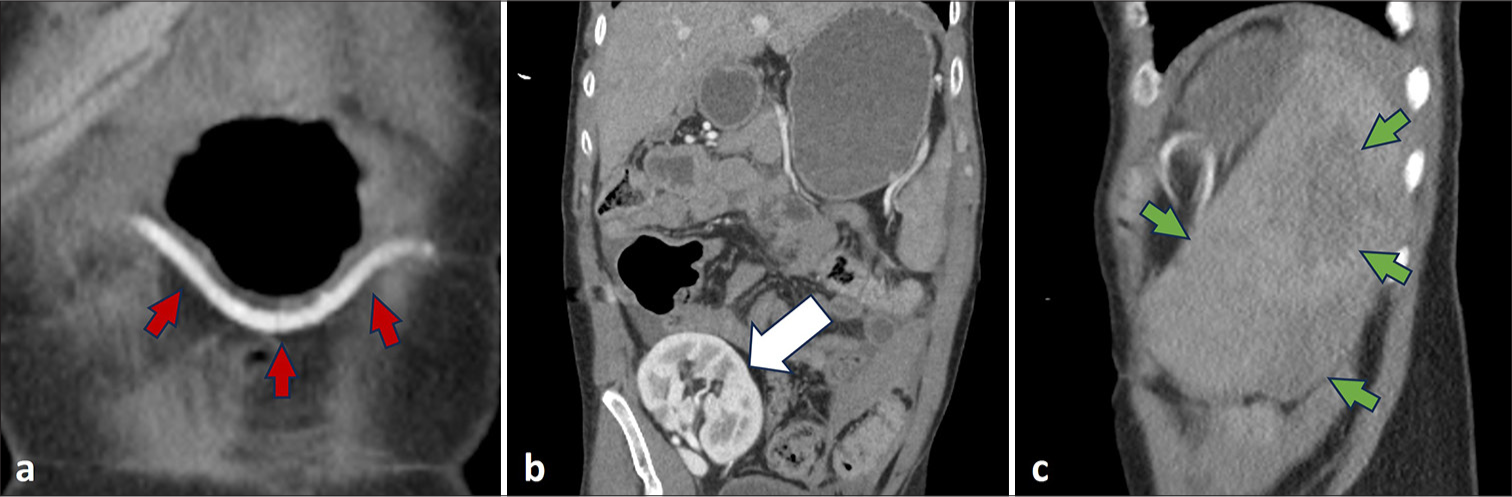
- A 30-year-old male presented with chest and shoulder pain after motorcycle accident. (a) Hypertrophied gastroepiploic artery (red arrows) anastomosing with distal splenic artery at splenic hilus seen on coronal CT slice. (b) Transplanted kidney (white arrow) seen on coronal CT slice. (c) Grade V subcapsular splenic lacerations (green arrows) seen on sagittal CT slice.
The celiac trunk was accessed using a 65 cm 5F SOS catheter (AngioDynamics, Latham, New York) through a right femoral artery puncture. Arteriography demonstrated a dilated and tortuous gastroepiploic artery (GEA) originating as usual from common hepatic and gastroduodenal arterial segments. Without an inner wire, the catheter was gently retracted and twisted so that its loop was less acutely angulated. Simultaneously, its tip was advanced into a common hepatic branch near the origin of the gastroduodenal artery (GDA). A stiff angled glide wire (Terumo, Somerset, New Jersey) was advanced through the GDA, right and subsequently left GEA segments. The SOS catheter was readily advanced over the wire and then exchanged for a more simple angle tipped 100 cm 5F hydrophilic catheter. The stiff angled glide wire was replaced with a non-stiff glide wire.
The left GEA was markedly redundant and tortuous, especially near the splenic hilus [Figure 3]. Distal embolization close to the splenic hilus was preferred to avoid embolization of gastric and pancreatic segments arising proximally from the GEA. The 100 cm catheter could not reach close enough to the splenic hilus; therefore, the glide wire was removed and a 130 cm 2.8F Progreat microcatheter (Terumo, Somerset, New Jersey) assembly was advanced through the 5F catheter until maximal length of the inner coaxial system achieved satisfactory proximity to the splenic hilus. Angiography demonstrated extravasation. The microwire was removed and a gelatin foam slurry including diluted contrast was injected for embolization. Post-embolization arteriography confirmed successful pruning and no extravasation [Figure 4]. The coaxial apparatus was removed, and hemostasis was achieved through manual compression.
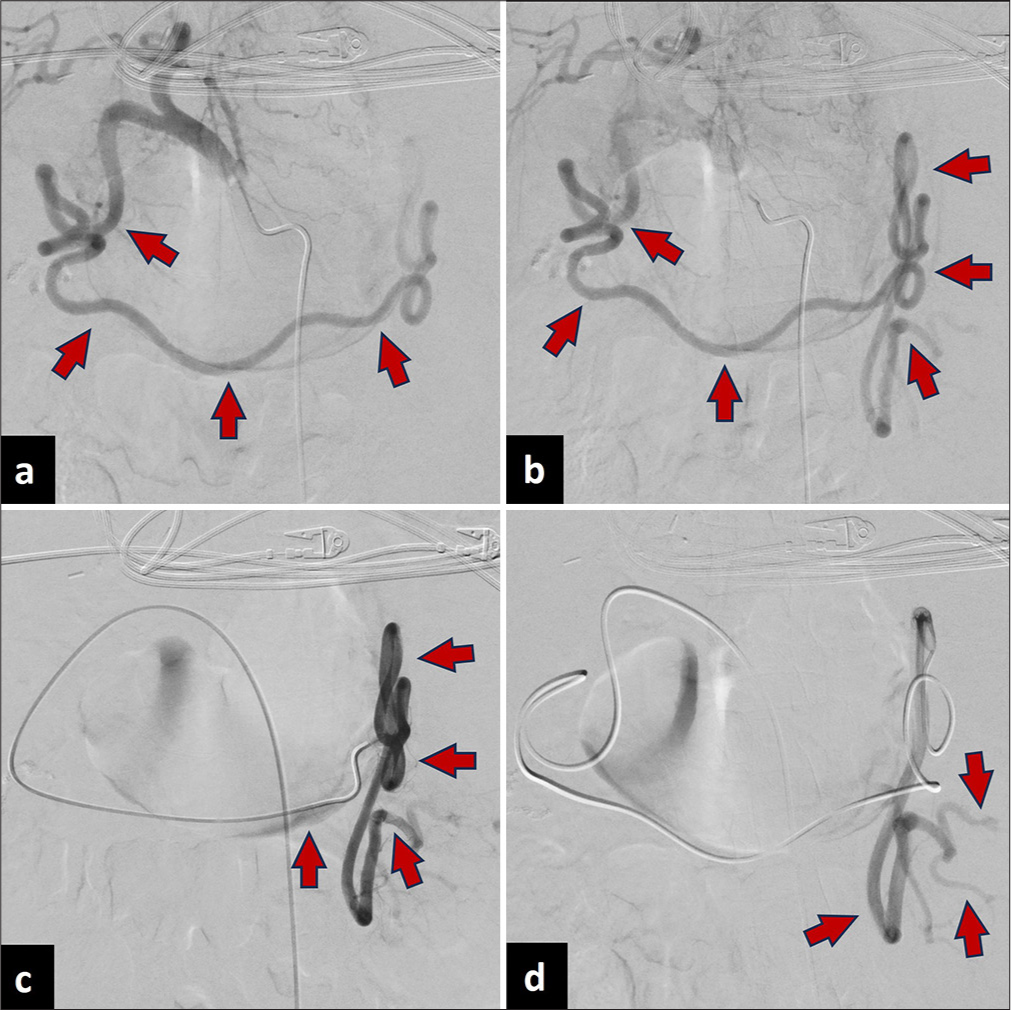
- A 30-year-old male presented with chest and shoulder pain after motorcycle accident. (a-d) Arteriography demonstrates dilated and tortuous GEA reaching until the splenic hilus (red arrows).
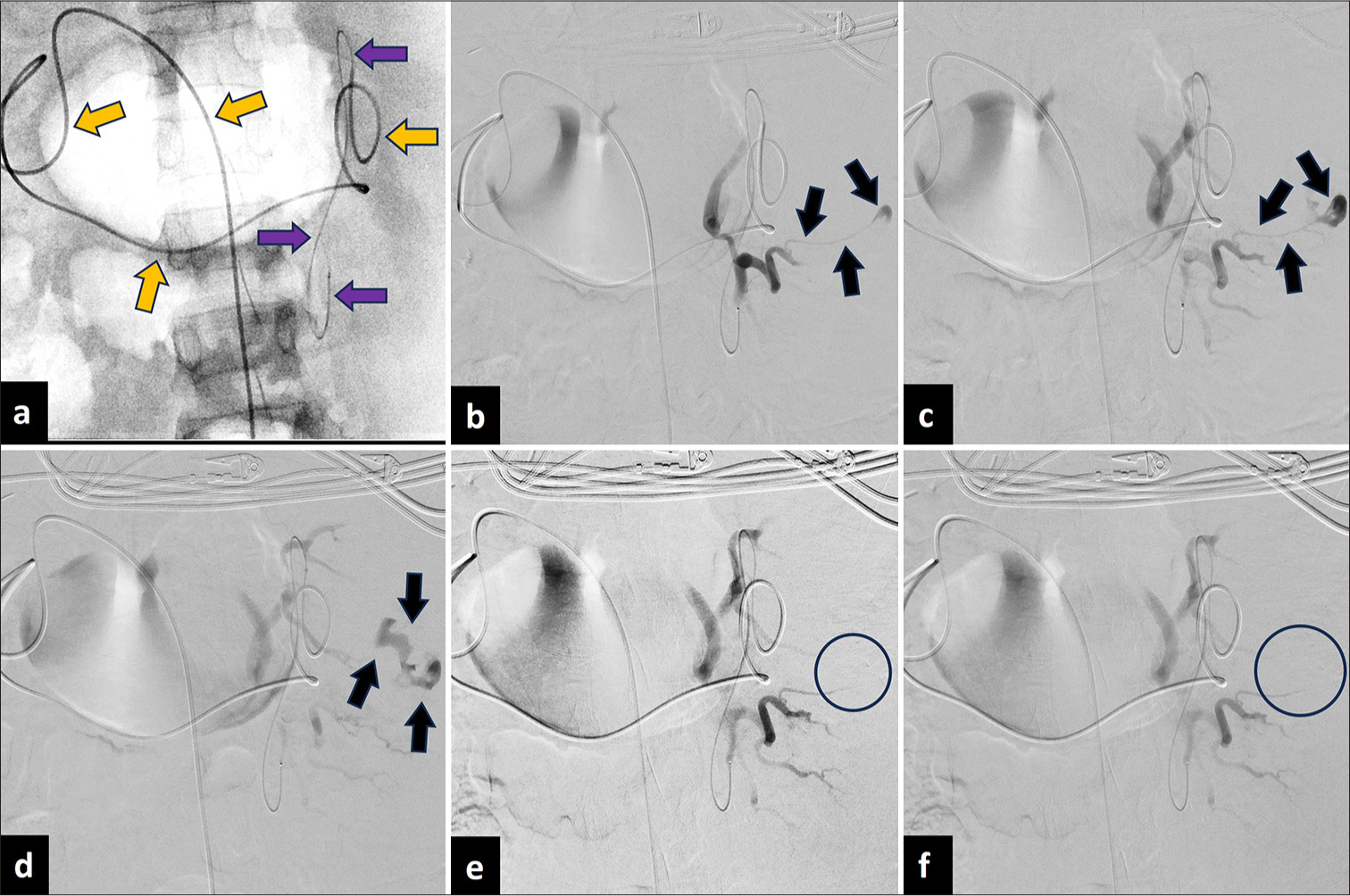
- A 30-year-old male presented with chest and shoulder pain after motorcycle accident. (a) Embolization using coaxial catheter (orange arrows)/microcatheter (purple arrows) system purposefully advanced close to splenic hilus to avoid needless embolization of gastric and superior pancreaticoduodenal segments arising from right GEA. (b-d) Contrast extravasation pre-embolization (black arrows), (e-f) no longer seen post-embolization (black circles).
The patient’s BP was 134/88 mmHg, and HR was 109 bpm during manual compression. He was transferred to the surgical intensive care unit (ICU) and later to a non-ICU bed before being discharged to his transplant center a week later.
DISCUSSION
Initial radiologic examination for blunt splenic trauma is a focused assessment with sonography in trauma (FAST) examination. Following a positive FAST, computed tomography (CT) with intravenous contrast is indicated. The American Academy of Surgery and Trauma splenic injury scale is used to grade the degree of splenic injury from I to V, with a high-grade injury characterized as greater than Grade III.[1-4] Hemodynamically stable patients with any grade of splenic injury are candidates for SAE. The goal of SAE is to reduce a high flow arterial flow to the site of injury. Proximal embolization achieves this by occluding the main splenic artery, whereas distal embolization selectively targets branch vessels.[4] Embolization can be performed using vascular plugs, coils/microcoils, gelatin foam, particles, or glue.[2-5]
SAE typically involves femoral artery puncture, celiac trunk selection, and splenic artery catheterization. However, in this case, given the prior splenic artery ligation, conventional embolization through the splenic artery was not feasible. Alternative approaches, such as surgical splenectomy or embolization through collateral pathways, were considered. However, splenectomy was avoided due to the risks of overwhelming post-splenectomy infection, particularly in an immunosuppressed transplant patient. The hypertrophied GEA was identified as a viable access route, providing a direct path to the spleen while preserving hepatic perfusion. This approach was deemed the safest and most effective method to control hemorrhage while minimizing potential complications.
Bashir et al. reported a case in which partial SAE was performed through right GEA in a patient post-liver transplantation with prophylactic splenic artery ligation. There were no reported complications immediately post-procedure and at 5 months follow-up.[8] Xu et al. reported a similar case in which partial SAE was performed following selections of GEA and dorsal pancreatic arteries in a patient post splenic artery ligation but without liver transplantation. Reported post-procedure complications included moderate fever and left upper abdominal pain which lasted for 15 days.[9] In both reports, embolization was performed using polyvinyl alcohol particles and the intervention was performed for the treatment of hypersplenism. Unlike these prior cases, our case involved emergent embolization with a gelatin foam slurry due to trauma rather than elective intervention for hypersplenism. In addition, no similar post-procedural complications in addition to gastric ischemia or pancreatic infarction were observed, reinforcing the feasibility of this approach in emergency settings. Loss to follow-up after the patient was transferred to his transplant facility was a limitation. In the case of acute trauma, it is important to review relevant anatomy on prior imaging to accurately perform a well-informed swift intervention.
CONCLUSION
This case describes emergent splenic embolization through a hypertrophied and tortuous GEA following blunt abdominal trauma in a liver transplant recipient with prior splenic artery ligation. By demonstrating the viability of this alternative embolization route, this case provides insight into managing complex vascular anatomy in trauma settings. When routine procedures are complicated by altered vascular anatomy, careful imaging review is essential to guide successful intervention.
Ethical approval
This is a single case report hence the Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The management of splenic injuries. Interv Radiol (Higashimatsuyama). 2023;9:149-55.
- [CrossRef] [PubMed] [Google Scholar]
- Splenic artery embolization for patients with high-grade splenic trauma: Indications, techniques, and clinical outcomes. Semin Intervent Radiol. 2021;38:105-12.
- [CrossRef] [PubMed] [Google Scholar]
- The impacts of different embolization techniques on splenic artery embolization for blunt splenic injury: A systematic review and meta-analysis. Mil Med Res. 2017;4:17.
- [CrossRef] [PubMed] [Google Scholar]
- Splenic trauma: Endovascular treatment approach. Ann Transl Med. 2021;9:1194.
- [CrossRef] [PubMed] [Google Scholar]
- Review of proximal splenic artery embolization in blunt abdominal trauma. CVIR Endovasc. 2019;2:11.
- [CrossRef] [PubMed] [Google Scholar]
- New strategies for prevention and treatment of splenic artery steal syndrome after liver transplantation. World J Gastroenterol. 2014;20:15367-73.
- [CrossRef] [PubMed] [Google Scholar]
- Splenic artery steal syndrome after liver transplantation-prophylaxis or treatment?: A case report and literature review. Ann Hepatobiliary Pancreat Surg. 2022;26:386-94.
- [CrossRef] [PubMed] [Google Scholar]
- Successful embolization of spleen through gastroepiploic artery in a liver transplant recipient with splenic artery ligation. J Clin Exp Hepatol. 2022;12:645-8.
- [CrossRef] [PubMed] [Google Scholar]
- Partial embolization as re-treatment of hypersplenism after unsuccessful splenic artery ligation. World J Gastroenterol. 2015;21:1365-70.
- [CrossRef] [PubMed] [Google Scholar]




