
Translate this page into:
Concepts for Liver Segment Classification: Neither Old Ones nor New Ones, but a Comprehensive One
Address for correspondence: Prof. Jean H. D. Fasel, Department of Cellular Physiology and Metabolism, University Medical Center, Rue M. Servet 1, CH - 1211 Geneva 4, Switzerland. E-mail: jean.fasel@unige.ch
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Concepts dealing with the subdivision of the human liver into independent vascular and biliary territories are applied routinely in radiological, surgical, and gastroenterological practice. Despite Couinaud's widely used eight-segments scheme, opinions on the issue differ considerably between authors. The aim of this article is to illustrate the scientific basis for understanding and harmonizing inconsistencies between seemingly contradictory observations. Possible clinical implications are addressed.
Keywords
Anatomy
liver
radiology
segments
surgery

INTRODUCTION

At first glance, the issue of vascular and biliary segments within the human liver seems definitively settled. This view is certainly related to the fact that a simple pragmatic concept of liver segmentation, namely the eight-segments scheme credited to Couinaud, has gained worldwide acceptance.[1] Despite the overwhelming utility of this classification, a review of the classic (some would say the old) literature - as well as an increasing number of inconsistencies observed during medical imaging studies and surgical operations - shows that, in fact, there is a notable confusion regarding liver compartmentalization. Symptomatically, recent publications propose new concepts of liver segmentation,[2] or even a new liver anatomy.[3] Belghiti even suggests that liver anatomy can actually change.[4] The importance of assessing liver anatomy by segmentation in radiology, gastroenterology, and surgery has recently been again pointed out. Bismuth states that “advances in surgical and radiologic techniques in recent years, including reduced-size liver for pediatric and adult transplants, split liver, and living donor in liver transplantation, make the reexamination and further the international consensus on hepatic anatomy and terminology of hepatectomies a current priority”.[5]
A rationale for explaining contradictory concepts has recently been proposed.[6] The present article aims to (i) illustrate the scientific basis for the inconsistencies between the supposedly old and new subdivisions by going beyond simple anatomical variability, and thus (ii) help radiologists and surgeons gain a better understanding of the limitations of the eight-segments scheme.[7891011121314]
This paper therefore reproduces some of the main differing opinions concerning liver segmentation on an invariable portal venous branching pattern. Accordingly, a single specimen was chosen from the University of Geneva Institute of Anatomy's collection of corrosion casts and investigated using high resolution computed tomography (CT). The portal vein branching pattern was reconstructed using the Liver Analyzer software (Fraunhofer MEVIS, Bremen) [Figure 1]. In other words, all illustrations in this review come from the same liver. This approach excludes anatomical variations of the portal vein branching pattern as an explanation for contradictory results.
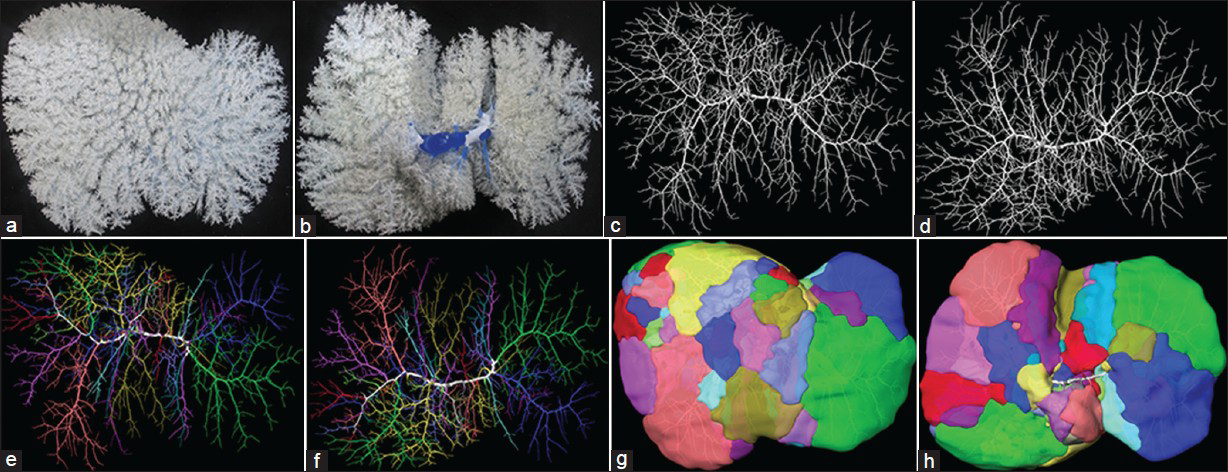
- Portal venous territories in a human liver. All figures are from the same liver, thus excluding any anatomical variation in the branching pattern. (a) Front view and (b) the posterior (also called inferior) view of the native portal venous corrosion cast; (c) Front view and (d) the posterior view of the portal venous branching pattern as reconstructed from CT images. The liver investigated had 24 second-order branches; (e) Front view and (f) the posterior view reveal the portal venous branching pattern with all second-order branches of the liver and the major third-order branches to the right hemiliver marked by different colors; (g) Front view and (h) the posterior view of the corresponding second and third-order territories.
LEVELS OF SEGMENTATION
There is general agreement about the existence of individual territories within the human liver, each with its own vascular and biliary system. However, the number, size, shape, and denomination of these areas have been, and are once more beginning to be, a controversial issue.
Hemilivers
All studies based on the Glissonian system (meaning the portal, arterial and biliary branching system rather than the hepatovenous pattern) agree upon the existence of 2 territories within the human liver (provided by the portal vein bifurcating). Rex,[15] Cantlie[16] and McIndoe and Counseller[17] were among the first to report on this issue. Since then, however, a variety of terms have been used for these two territories (hemilivers, hemihepates, hepates, livers, lobes, main parts, parts, sides, territories, etc.). This paper applies the term hemilivers (Greek: hemihepates) - A right hemiliver (RHL) and a left hemiliver (LHL) can thus be distinguished.
Sectors
When taking into account what are customarily called the main ramifications of the triad (in particular those of the portal vein), most investigators further subdivide the 2 hemilivers into 2 further parts each, leading to a quadripartition of the liver [Figure 2]. Again, many different terms have been used for these territories (lobes, portions, sections, sectors, segments etc). The present article uses the term sector, and Goldsmith and Woodburne's denominations of right posterior, right anterior, left medial, and left lateral sectors (RPS, RAS, LMS, LLS).[18]
![The concept of 4 sectors. (a) Original illustration by Rex.[15] (b) As applied to the corrosion cast.](/content/12/2013/3/1/img/JCIS-3-48-g003.png)
- The concept of 4 sectors. (a) Original illustration by Rex.[15] (b) As applied to the corrosion cast.
However, at this level of liver partition already, some authors disagree with the mainstream four-sector concept. Hjortsö[19] considered the RHL to included 3 (not 2) sectors; he called these territories ventrocranial, intermediate, and dorsocaudal segments [Figure 3a]. Kogure et al.,[20] and Cho et al.,[2122] have recently proposed this classification again.
![The concept of 5 or 6 sectors, as a result of partition of the right hemiliver into 3 (and not 2) sectors (called segments by Hjortsö). (a) Original figure.[19] (b) Reproduction on the same corrosion cast as in Figure 2b. This means that the seemingly contradiction between Figures 2b and 3b cannot be explained by anatomical variation.](/content/12/2013/3/1/img/JCIS-3-48-g004.png)
- The concept of 5 or 6 sectors, as a result of partition of the right hemiliver into 3 (and not 2) sectors (called segments by Hjortsö). (a) Original figure.[19] (b) Reproduction on the same corrosion cast as in Figure 2b. This means that the seemingly contradiction between Figures 2b and 3b cannot be explained by anatomical variation.
Of course, such a tripartition of the RHL can be the result of an anatomical variation, a trifurcation of the right portal vein (RPV). However, it can also well be obtained in the usual case of a RPV bifurcation, that is by considering that the branches to the RAS vascularize 2 sectors (and not 1), as illustrated in [Figures 1 and 3].
Ryu and Cho[3] published a reclassification considering both the RHL and LHL to be subdivided into 3 sectors (they called segments), not including the caudate lobe. The liver as a whole may then be considered as presenting 7 portal venous territories (neither 4 sectors, nor 8 segments). In contrast, Takasaki[2] discerned 3 sectors for the liver as a whole (which he named right segment, middle segment, and left segment) [Figure 4].
![Takasaki's concept of 3 sectors (he calls segments).[2] (a) Original figure, (b) rendering on our liver cast.](/content/12/2013/3/1/img/JCIS-3-48-g005.png)
- Takasaki's concept of 3 sectors (he calls segments).[2] (a) Original figure, (b) rendering on our liver cast.
However, even amongst authors who agree on the existence of 4 sectors, opinions differ about their boundaries. For instance, Couinaud,[1] Bismuth[23] and others consider the portal venous segment II (without segment III) to correspond to a sector. Thus, in fact, they disagree with the view that the LLS is limited by the umbilical fissure (fissure for the ligamentum teres and venosum), as is generally assumed.
Segments
There is definite disagreement on the next level of liver compartmentalization - the further subdivision of the sectors. Not only does the terminology again differ (areas, sections, segments, subsegments, etc.), but the divergence of opinion is deeper:
-
To begin with, some authors did not consider there to be any further subdivision of the sectors. Most American radiologists, for instance, referred to nothing more than the four sectors until the intervention of Dodd in 1993.[24]
-
Other investigators restricted subdivisions to just some of the sectors. Hjortsö,[19] for instance, only considered there to be a bipartition in the LLS. Gans[25] considered only a transverse fissure to the RPS. Kekis and Kekis[26] considered there to be superior and inferior parts to the LLS and the RPS, but not to the RAS and LMS. In 1957, Couinaud,[1] did not mention a subdivision of either segment IV or the caudate lobe [Figure 5]. He later refuted the existence of any transverse scissure, which had been erroneously attributed to him by some authors.[27] Bismuth[23] did not subdivide the LMS either.
![Couinaud's compartmentation:[1] 4 sectors, 8 segments (I-VIII, including the caudate lobe). (a) Original illustration, (b) reconstruction on our corrosion cast.](/content/12/2013/3/1/img/JCIS-3-48-g006.png) Figure 5
Figure 5- Couinaud's compartmentation:[1] 4 sectors, 8 segments (I-VIII, including the caudate lobe). (a) Original illustration, (b) reconstruction on our corrosion cast.
-
The most current widespread view, as mentioned, subdivides all sectors into a superior and an inferior area, yielding 8 territories. This number was first been proposed by Healey and Schroy[28] [Figure 6], then by Couinaud,[29] Healey,[30] and Bismuth.[23] Of the differing terminology for these areas, the most popular is that of segments. This term is thus used in the present paper.
![Healey and Schroy's concept:[28] 2 hemilivers, 4 sectors, 8 segments, but exclusive of the caudate lobe. a) Original illustration showing 4 sectors (a posterior, anterior, medial, and lateral one) in an anterior view, with a superior and inferior area for each, b) reconstruction on our corrosion cast.](/content/12/2013/3/1/img/JCIS-3-48-g007.png) Figure 6
Figure 6- Healey and Schroy's concept:[28] 2 hemilivers, 4 sectors, 8 segments, but exclusive of the caudate lobe. a) Original illustration showing 4 sectors (a posterior, anterior, medial, and lateral one) in an anterior view, with a superior and inferior area for each, b) reconstruction on our corrosion cast.
-
Finally, one group of authors advocate the existence of more than 8 segments. Couinaud himself introduced a ninth segment in 1998,[2731] though he later abandoned this proposition.[32] Gupta et al.,[33] also reported nine territories (which they called sub-segments). In fact, their compartmentalization bears similarities with Couinaud's, but from the beginning they added the caudate lobe and caudate process together as territory number nine. They also numbered the segments in another order, but it was that credited to Couinaud[1] which gained general acceptance. Gans[25] interpreted Healey and Schroy's[28] division encompassing even 10 segments. Platzer and Maurer[34] observed 2-5 segments (often 3) solely within the LLS [Figure 7]. Elias and Petty[35] took the view the main portal territories were constant, with 4 for the LLS (superior, intermediate, inferior, and omental one), 6 for the LMS (venous, quadrate, paracystic, left and right caudate, and the caudate process), and 3 for the RHL central, inferior, and lateral territory). This view would have one consider 13 segments in the human liver. However, they did admit to “a certain arbitrariness” in establishing these segments.
![Platzer and Maurer's concept:[34] 4 sectors, no segments in the right hemiliver, but 3 in both the left lateral sector and left medial sector, as an example. a) Original illustration, (b) reconstruction on our corrosion cast.](/content/12/2013/3/1/img/JCIS-3-48-g008.png) Figure 7
Figure 7- Platzer and Maurer's concept:[34] 4 sectors, no segments in the right hemiliver, but 3 in both the left lateral sector and left medial sector, as an example. a) Original illustration, (b) reconstruction on our corrosion cast.
Subsegments
If the concept of 8 segments is accepted, the next level down of liver territories should logically be called subsegments. Lee et al.,[36] for instance, supported the bipartition of not only segment IV (into subsegments IVa and IVb), but also segment VIII (into subsegments VIIId and VIIIv) [Figure 8]. This view is in accordance with that published by Cho et al.,[37] and resembles that presented by Trinh Van Minh and Galizia[38] who designated subsegments VIIIe, VIIIi in segment VIII. Takayasu et al.,[39] even divided the portal branches to segment VIII into 4 subsegmental groups (ventral, dorsalateral, dorsal and medial). Healey and Schroy,[28] who also proposed 8 segments, not including the caudate lobe, further subdivided the latter into 3 subsegments (calling them right portion, left portion, and caudate process). Platzer and Maurer[34] reported 1-4 territories within segment IVa. Elias and Sherrick[40] mention that smaller branches coming off the right and left portal vein can always be found by careful dissection, and - grouping some of them - even gave names to 13 of them. Rex[15] had acknowledged these smaller vessels in 1888 by designating the LMS and LLS as “rechtes und linkes Astwerk”, or “right and left entity made of a multitude of branches” [Figure 2]. Fasel[41] counted between 9 and 44 so-called second-order portal venous territories (with a mean of 20). Takasaki[2] subdivided his 3 sectors (which he called segments) into 6 to 8 areas each. Following this concept, the liver as a whole encompasses between 18 and 24 subsegments (which he designated as cone units) [Figure 9].
![According to Lee et al.,[36] Segment VIII is subdivided into 2 subsegments (d, v) for the sake of illustrating homology with Segment IV (a, b). (a) Original illustration, (b) concept applied to our liver cast.](/content/12/2013/3/1/img/JCIS-3-48-g009.png)
- According to Lee et al.,[36] Segment VIII is subdivided into 2 subsegments (d, v) for the sake of illustrating homology with Segment IV (a, b). (a) Original illustration, (b) concept applied to our liver cast.
![Takasaki implicite subdivided the liver into 18-24 subsegments (he named cone units).[2] (a) Original picture, illustrating two subsegments, taking 3rd order branches of the main portal branch to the right anterior sector as an example, (b) corresponding reconstruction on the corrosion cast.](/content/12/2013/3/1/img/JCIS-3-48-g010.png)
- Takasaki implicite subdivided the liver into 18-24 subsegments (he named cone units).[2] (a) Original picture, illustrating two subsegments, taking 3rd order branches of the main portal branch to the right anterior sector as an example, (b) corresponding reconstruction on the corrosion cast.
COMMON DENOMINATOR
Apart from anatomical variability, the common denominator for these seeming contradictions is simple: it is related to the fact that the Glissonian (and in particular the portal venous) branching pattern encompasses more rami than generally assumed in radiological and clinical practice. Consequently – and this is the key to understanding such disagreements – the question is how to group multiple branches in order to obtain a few number of territories for the sake of convenience.
Let us consider the most frequent anatomical situation where the PV bifurcates into a RPV and a LPV. All authors having carefully dissected post-mortem livers or looked at corrosion casts agree, without exception, that when taking into account all the branches (including the small ones) coming directly off the RPV and LPV, there are significantly more than 8. This fact, however, is only true when the RPV is defined as the vessel extending as far as a bifurcation into two main branches (to the RAS and RPS); and when the LPV is defined as extending as far as its dead-end in Rex's recessus. Using this premise the liver consists of 2 hemilivers at the first-order level (RPV/LPV), and of more than 8 territories at the next, second-order level. In the liver illustrated in this paper, for instance, there were 24 branches of this nature, and thus 24 second-order territories [Figure 1]. Today, because Couinaud's 8 territories are established worldwide and are called segments, there is a compelling argument for designating these second-order areas as subsegments. However, considering the arbitrary definition of segments mentioned above, we suggest the more neutral term of subunits, instead of subsegments. Using different combinations of these 24 branches and their respective subunits, any number of territories less than 24 can be obtained, going as low as 8 (or 9, 10, 13 etc).
In other words, it is the high number of branches coming directly off the right and left portal vein (as defined in the preceding paragraph) that explains the seemingly differing observations. These rami have been arbitrarily grouped by different investigators. In fact, it is not necessarily the reality which differs, but the interpretations intended to serve clinical applications.
OTHER FEATURES OF LIVER SEGMENTATION
Besides the number of territories, two other features should be briefly noted here; they concern the boundaries between these territories. Firstly, the location of boundaries may not be where they are expected. For instance, the boundary between the right and left hemiliver far from always corresponds to the line running from the gallbladder to the inferior vena cava line. Secondly, the shape of the boundaries does not always correspond to simple flat planes. They can display dentate outlines [Figure 10].

- Intraoperative situs documenting that the boundaries of the vascular territories are not always simple straight lines (corresponding to orthogonal flat planes), but may display wavy outlines. (Courtesy Prof. P. Majno, Department of Visceral Surgery, Geneva University Hospitals, Switzerland).
TERMINOLOGY
As mentioned, the nomenclatures concerning hepatic territories remain heterogeneous and confusing.[542434445] This paper confirms that this is not a surprise, especially considering the arbitrariness of segment definitions that has been carried out by amalgamating what are essentially independent branches and individual territories into major entities for the sake of obtaining simple classification schemes. Interestingly enough, the Terminology Committee of the International Hepato-Pancreato-Biliary Association[43] mentioned that its task was “to deal with terminology … not with anatomy per se”.
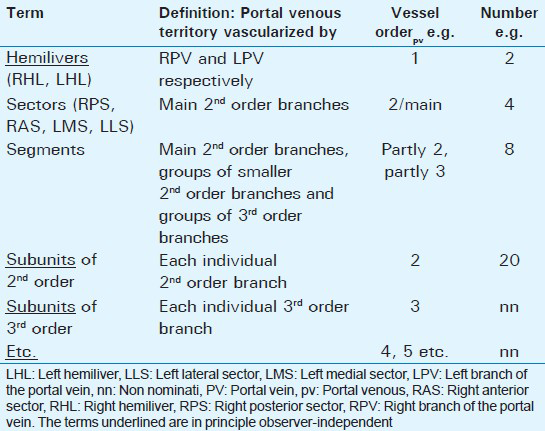
To the contrary, taking into account anatomy, we suggest the following terms for portal venous liver subdivisions. Those entities which are in principle observer-independent are underlined. A synoptic view of the proposal is given in Table 1.
-
Lobes: The lobes (right, left, quadrate, and caudate) are those liver parts that have been defined for centuries on the basis of external landmarks.
-
Hemilivers: These are the territories irrigated by the right and left branch of the portal vein. In general terms, they are the territories depending (in the regular case of portal venous bifurcation) on the two first-order branches of the portal vein and the corresponding arterial and biliary branches.
-
Sectors: The sectors correspond to territories defined by the so-called main second-order branches.
-
Segments: Segments are arbitrary entities, defined as territories that depend partly on major second-order branches (regularly for Couinaud's segment II, for instance), partly on gathered groups of smaller second-order branches (often for Couinaud's segments I, III and IV), and partly on groups of third-order branches (in particular for Couinaud's segments V to VIII).
-
Subunits2: Subunits2 are defined as territories vascularized by individual branches coming directly off the RPV and LPV. In general terms, every territory depending on an individual second-order Glissonian branch (including small ones) is a subunit2.
-
Subunits3: These are the territories depending on the individual third-order branches of the Glissonian triad. They were designated as cone units by Takasaki.[2].
-
Subunits4, 5 etc.
One of the main problems with such a terminology, however, consists in how to define hierarchical orders within branching patterns. At first glance, this definition may look very clear, but in fact it is anything but unambiguous, even at a purely mathematical level.[46]
CLINICAL APPLICATIONS
Clinical applications of this “subunits-concept” are likely to become more numerous due to the well-known trend toward ever more customized, personalized medicine, including minimally invasive procedures in radiology. As far as surgery is concerned, operating techniques aimed at or allowing the resection of such “subsegmental” territories have, in fact, been used for decades.[2474849] Proposals for smaller segment grafts have recently also been made.[50]
CONCLUSION
Although radiological observations deviating from the eight-segments scheme are promptly attributed to anatomical variability, this paper illustrates another common denominator that allows the reconciliation of seemingly contradictory concepts. The key point to understanding the disagreements is to be aware of the fact that there are not just 8 Glissonian (in particular portal venous) branches for 8 territories, but that the branching pattern encompasses more rami than generally assumed. It is this higher number of branches coming directly off the RPV and LPV – which different investigators have arbitrarily gathered together or which simply cannot be identified on patients using current imaging techniques - that yield seemingly differing observations. In fact, it is not the reality that necessarily differs, but the interpretations intended to serve clinical applications.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/48/120803
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Le foie. Etudes anatomiques et chirurgicales. In: The Liver. Anatomical and surgical investigations. Paris: Masson; 1957.
- [Google Scholar]
- Glissonean Pedicle Transection Method for Hepatic Resection. Tokyo, Berlin, Heidelberg, New York: Springer; 2007.
- [Google Scholar]
- Ryu M, Cho A, eds. New Liver Anatomy. Tokyo, Berlin, Heidelberg, New York: Springer; 2009.
- Revisiting liver anatomy and terminology of hepatectomies. Ann Surg. 2013;257:383-6.
- [Google Scholar]
- Liver segments: An anatomical rationale for explaining inconsistencies with Couinaud's eight-segment concept. Surg Radiol Anat. 2010;32:761-5.
- [Google Scholar]
- Segmental anatomy of the liver: Poor correlation with CT. Radiology. 1998;206:151-6.
- [Google Scholar]
- Limits of Couinaud's liver segment classification: A quantitative computer-based three-dimensional analysis. J Comput Assist Tomogr. 2002;26:962-7.
- [Google Scholar]
- Segmental anatomy of the liver under the right diaphragmatic dome: Evaluation with axial CT. Radiology. 1996;200:779-83.
- [Google Scholar]
- Segmental anatomy of the liver in computed tomography: Do we localize the lesion accurately? Rofo. 2000;172:147-52.
- [Google Scholar]
- Definition of a new correct functional anatomy. Available from: http://www.passport.liver.eu/News_files/Passport D1.3_1.pdf
- [Google Scholar]
- Limitations and pitfalls of Couinaud's segmentation of the liver in transaxial imaging. Eur Radiol. 2003;13:2472-82.
- [Google Scholar]
- Beiträge zur Morphologie der Säugetiere. Contributions to the Mammalian liver's morphology. 1888;14:517-617.
- [Google Scholar]
- On a new arrangement of the right and left lobes of the liver. J Anat Physiol. 1898;32:4-9.
- [Google Scholar]
- The surgical anatomy pertaining to liver resection. Surg Gynecol Obstet. 1957;105:310-8.
- [Google Scholar]
- The topography of the intrahepatic duct systems. Acta Anat (Basel). 1951;11:599-615.
- [Google Scholar]
- Reproposal for Hjortsjo's segmental anatomy on the anterior segment in human liver. Arch Surg. 2002;137:1118-24.
- [Google Scholar]
- Proposal for a reclassification of liver based anatomy on portal ramifications. Am J Surg. 2005;189:195-9.
- [Google Scholar]
- Relationship between right portal and biliary systems based on reclassification of the liver. Am J Surg. 2007;193:1-4.
- [Google Scholar]
- An American's guide to Couinaud's numbering system. AJR Am J Roentgenol. 1993;161:574-5.
- [Google Scholar]
- Introduction to Hepatic Surgery. Amsterdam, Houston, London, New York: Elsevier; 1955.
- [Google Scholar]
- Surgical anatomy of the liver. In: Karaliotas CC, Broelsch CE, Habib NA, eds. Liver and Biliary Tract Surgery. Wien, New York: Springer; 2006. p. :25-33.
- [Google Scholar]
- Anatomy of the biliary ducts within the human liver; analysis of the prevailing pattern of branchings and the major variations of the biliary ducts. AMA Arch Surg. 1953;66:599-616.
- [Google Scholar]
- Lobes and segments hépatiques. Hepatic lobes and segments. Presse Médicale. 1954;62:709-12.
- [Google Scholar]
- Clinical anatomic aspects of radical hepatic surgery. J Int Coll Surg. 1954;22:542-50.
- [Google Scholar]
- The dorsal sector of human liver: Embryological, anatomical and clinical relevance. Hepatogastroenterology. 2000;47:1726-31.
- [Google Scholar]
- The caudate lobe of the liver: Implications of embryology and anatomy for surgery. Surg Oncol Clin N Am. 2002;11:835-48.
- [Google Scholar]
- Gross anatomy of the blood vessels and ducts within the human liver. Am J Anat. 1952;90:59-111.
- [Google Scholar]
- Ramification of Glisson's sheath peripheral branches and clinical implications in the era of local ablation therapy. Surg Radiol Anat. 2010;32:911-7.
- [Google Scholar]
- Anatomy of the right anterosuperior area (segment 8) of the liver: Evaluation with helical CT during arterial portography. Radiology. 2000;214:491-5.
- [Google Scholar]
- Segmentation of the liver and anatomical variants of the portal system. Ann Chir. 1990;44:561-9.
- [Google Scholar]
- Intrahepatic portal vein branches studied by percutaneous transhepatic portography. Radiology. 1985;154:31-6.
- [Google Scholar]
- Portal venous territories within the human liver: An anatomical reappraisal. Anat Rec (Hoboken). 2008;291:636-42.
- [Google Scholar]
- Terminology of liver anatomy and liver resections: Coming to grips with hepatic Babel. J Am Coll Surg. 1997;184:413-34.
- [Google Scholar]
- Use and dissemination of the brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg. 2013;257:377-82.
- [Google Scholar]
- Could we or should we replace the conventional nomenclature of liver resections? Ann Surg. 2013;257:387-9.
- [Google Scholar]
- Diameter-defined Strahler system and connectivity matrix of the pulmonary arterial tree. J Appl Physiol. 1994;76:882-92.
- [Google Scholar]
- A new technique of hepatic segmentectomy by selective portal venous occlusion using a balloon catheter through a branch of the superior mesenteric vein. World J Surg. 2007;31:1240-2.
- [Google Scholar]
- Anatomical segmental and subsegmental resection of the liver for hepatocellular carcinoma: A new approach by means of ultrasound-guided vessel compression. Ann Surg. 2010;251:229-35.
- [Google Scholar]
- Parenchyma-wise technique for the harvest and implantation of hepatic segment 2-3 grafts: Anatomic basis and surgical steps. Clin Anat. 2011;24:748-56.
- [Google Scholar]




