
Translate this page into:
Atlanto-occipital assimilation: A pictorial review of a commonly missed pathology

*Corresponding author: Ho Nam Ho, Department of Radiology, Tseung Kwan O Hospital, Tseung Kwan O, Hong Kong. calvin168hk@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ho H, Chau H, Pan N, Lo B. Atlanto-occipital assimilation: A pictorial review of a commonly missed pathology. J Clin Imaging Sci. 2024;14:24. doi: 10.25259/JCIS_42_2024
Abstract
Atlanto-occipital assimilation is a congenital craniovertebral junction malformation where the partial or complete fusion of the atlas and occiput occurs. Atlanto-occipital assimilation can be associated with numerous complications, including basilar invagination, atlantoaxial subluxation, Chiari malformation, congenital vertebral bodies fusion, and cord compression. As a result, vigilant identification and accurate reporting of atlanto-occipital assimilation are essential. The purpose of this review article is to discuss the numerous complications and associations of atlanto-occipital assimilation, such that an accurate diagnosis could be made for this commonly missed pathology.
Keywords
Atlanto-occipital assimilation (AOA)
Craniocervical junction
Cord compression

INTRODUCTION
Atlanto-occipital assimilation is a congenital craniovertebral junction malformation where the partial or complete fusion of atlas and occiput occurs. The incidence of atlanto-occipital assimilation was estimated to be 0.14–0.75% among the general population, affecting males and females equally.[1,2] Although most patients with atlanto-occipital assimilation are asymptomatic, some could be complicated by cervical cord compression. As a result, vigilant identification and accurate reporting of atlanto-occipital assimilation are essential. Flexion and extension radiography, computed tomography (CT), and magnetic resonance imaging all play important roles in diagnosing and evaluating complications of atlanto-occipital assimilation.
This pictorial review illustrates interesting cases of atlanto-occipital assimilation from Princess Margaret Hospital in Hong Kong, collected over the past 8 years. Numerous complications and associations of atlanto-occipital assimilation (e.g., basilar invagination, atlantoaxial subluxation, Chiari malformation, congenital vertebral bodies fusion, and compressive myelopathy) would be discussed, supported by real cases.
CLASSIFICATION
Atlanto-occipital assimilation is classified into three types:
Anterior arch assimilation [Figure 1a]
Posterior arch assimilation [Figure 1b]
Assimilation of both anterior and posterior arches [Figure 1c].
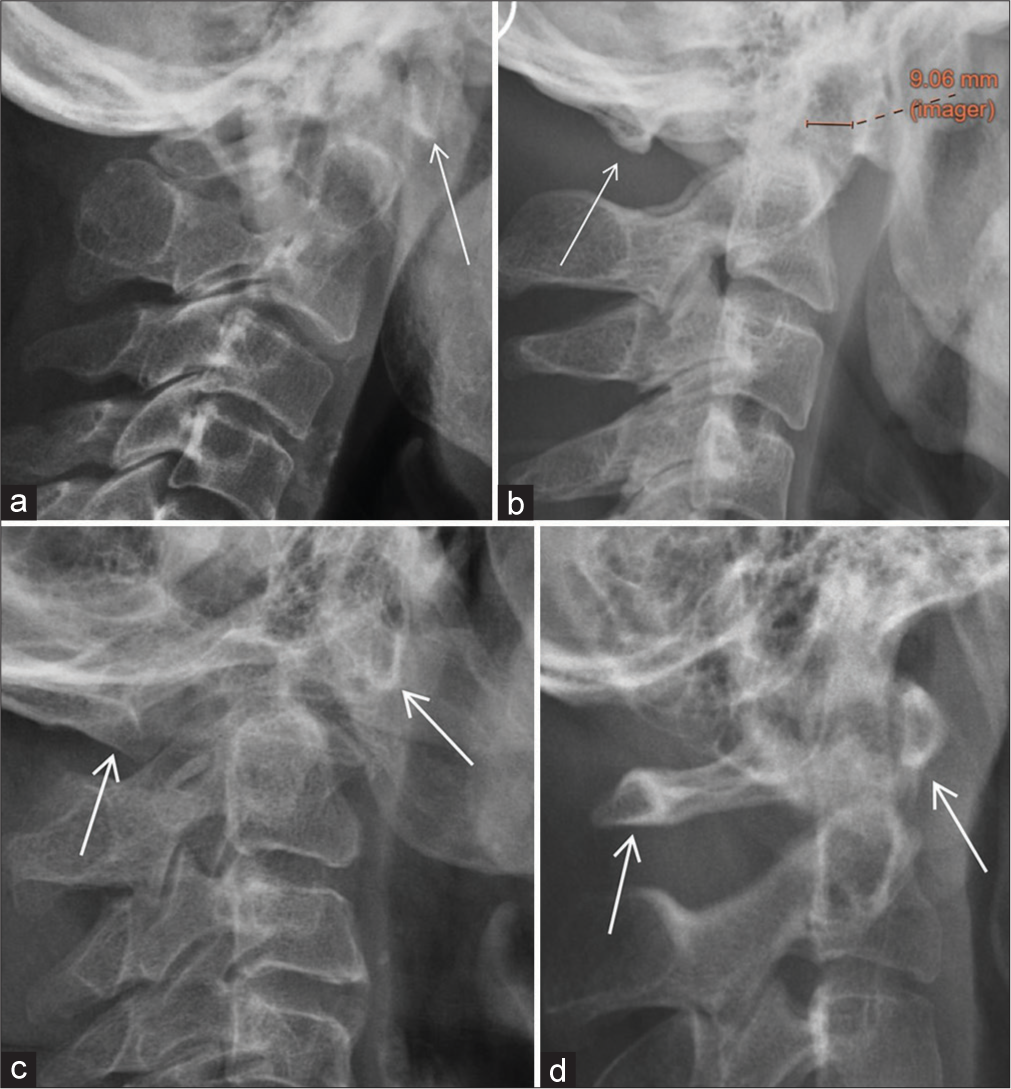
- (a) Plain radiograph of cervical spine showing anterior arch assimilation, as evidenced by the absence of anterior arch of (C1) atlas anterior to the dens. The anterior arch of C1 is fused to the clivus. (white arrow) Identification of anterior C1 arch assimilation would sometimes be difficult, due to overlapping structures (e.g., bilateral mandibles). The anterior arch of the C1 should be actively searched for when assessing lateral neck radiograph to avoid missing anterior arch of C1 assimilation. Notice that the posterior arch of C1 is still distinctly seen. (b) Plain radiographs of cervical spine showed posterior arch assimilation, as evidenced by fusion of the posterior arch of C1 to occiput. (white arrow) The anterior arch of C1 is still distinctly seen anterior to the dens. An associated increase in atlantodental interval is noted (orange measurement calipers), suggestive of atlantoaxial subluxation. (c) Plain radiographs of the cervical spine showing assimilation of both anterior and posterior arches of C1 (white arrows). (d) Plain radiograph of the cervical spine of a normal patient. Both the anterior and posterior arches of C1 could be distinctly seen. (white arrows).
A normal radiograph of the craniovertebral junction is included as a reference [Figure 1d].
This classification is based on the differences in embryological origins of the anterior arch and posterior arch of the atlas. The clinical implication for classifying atlanto-occipital assimilation into three main groups is that different types of atlanto-occipital assimilation are associated with different types of basilar invagination. This will be further elaborated later.
EMBRYOLOGY AND GENETICS
The craniovertebral junction is an embryologically unstable region and is subjected to numerous variations, with atlanto-occipital assimilation being one of the most common anomalies.[3] The embryological instability of the craniovertebral junction is considered analogous to the lumbosacral region, where lumbarization of S1 and sacralization of L5 are commonly seen.
According to Pang and Thompson, the hypochordal bow of proatlas forms the anterior atlantal arch and the lateral dense zone of the C1 sclerotome forms the posterior atlantal arch. Due to their differences in embryological origin, different types of atlanto-occipital assimilation could therefore be observed radiologically.[3]
It is postulated that mutations of the Hox gene homologues could be responsible for causing atlanto-occipital assimilation, as demonstrated in mouse models. Inappropriate repression of Pax-1 may be responsible for combined atlanto-occipital assimilation and Klippel-Feil syndrome.[3]
ASSOCIATIONS AND COMPLICATIONS
Atlanto-occipital assimilation is associated with numerous pathologies which should be actively searched for once it is identified. Associated complications should be mentioned in the radiology report since they are essential in guiding subsequent patient management.
Basilar invagination
Atlanto-occipital assimilation could be associated with both Type I and Type II basilar invagination.
Type I basilar invagination refers to the odontoid process directly invaginating inside the foramen magnum and is associated with craniocervical instability [Figure 2]. Type II basilar invagination is not associated with craniocervical instability and is characterized by a flattened basicranium.
- (a) Plain radiograph of cervical spine showing atlanto-occipital assimilation of both anterior and posterior arches. (white arrows) The odontoid is noted protruding through the foramen magnum, beyond the McRae line, suggestive of type 1 basilar invagination. The atlanto-dental interval is increased, suggestive of atlantoaxial subluxation. (b) Previous computed tomography (CT) brain of the same patient, showed associated compression on the cervicomedullary junction of the spinal cord. The craniovertebral junction should always be included in the review area while assessing a CT brain to avoid missing pathologies.
It is postulated that type I basilar invagination is more associated with anterior arch assimilation since the anterior arch of the atlas and the atlantoaxial ligament system share a common embryological origin. Type II basilar invagination, on the other hand, is more associated with posterior arch assimilation.[4]
Type I basilar invagination is more prone to direct brainstem compression due to odontoid process indentation. Type II basilar invagination can lead to a reduction in posterior cranial fossa volume and subsequent Chiari malformation.[5]
Anteroposterior atlantoaxial subluxation
The distance between the anterior arch of C1 and the dens in a fully flexed position should be <3 mm in adults and <5 mm in children.[6] The atlantoaxial subluxation can be occult in a standard lateral view of the cervical spine. Flexion and extension radiographs are helpful in detecting occult anteroposterior atlantoaxial subluxation [Figure 3].
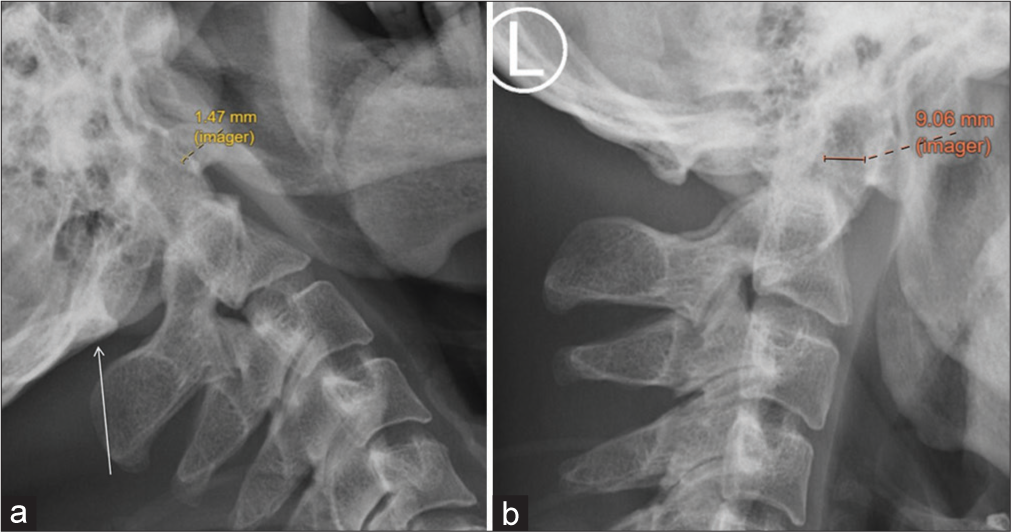
- (a) Extension radiograph of the cervical spine showing posterior arch assimilation (white arrow). The atlantodental interval is within normal limits under extension view, measuring 1.47 mm. (yellow measurement calipers). (b) Flexion cervical spine radiograph of the same patient showed an atlanto-dental interval with marked widening, measuring 9.06mm (orange measurement calipers), suggestive of atlantoaxial subluxation. Atlanto-axial subluxation may be missed if dynamic flexion and extension study is not performed.
Fusion of adjacent vertebral bodies
Atlanto-occipital assimilation could be associated with numerous types of fusion of vertebral bodies. By far, a fusion of C2/3 vertebral bodies would be the most common. Examples are illustrated in the following cases [Figures 4-6]. In patients with a congenital fusion of vertebral bodies or Klippel-Feil syndrome, the wasp-waist sign could be observed, meaning that the anteroposterior diameter of the affected discovertebral joint is smaller than the diameter of the superior and inferior limits of the vertebral bodies adjacent to uninvolved discs[7] [Figure 6].

- (a) Plain radiograph of the cervical spine showing anterior arch assimilation. Associated fusion of C2 and C3 vertebral bodies and posterior elements were noted. The atlantodental interval is within normal limits. No basilar invagination was seen. (b) Annotated computed tomography (CT) of the cervical spine, confirming the findings on plain radiograph. Notice the relatively ‘elongated’ appearance of the dens, supporting the diagnosis of C2/3 fusion. (c) Coronal reformatted CT of the cervical spine showing C2/3 fusion. The first rib-bearing thoracic vertebral body is labeled as T1. (d) T1W magnetic resonance imaging of the cervical spine, confirming previous findings. The cervical cord is not compressed.

- (a) Computed tomography (CT) of the cervical spine showing atlanto-occipital assimilation with anterior and posterior arches assimilation. Fusion between the dens, assimilated C1, and clivus was seen. C3 is being labeled as a reference. Marked narrowing of the spinal canal was noted. (b) Subsequently arranged sagittal T2-weighted magnetic resonance imaging confirming CT findings and showing cord compression.
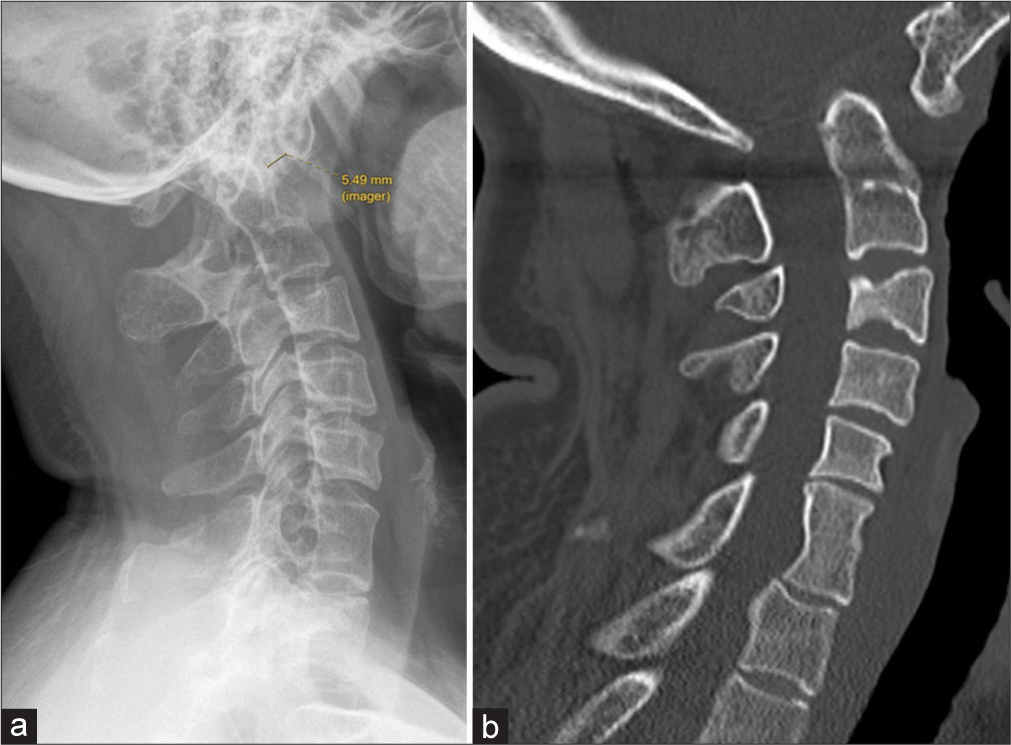
- (a) Lateral X-ray of cervical spine, showing atlanto-occipital assimilation with anterior arch assimilation. Fusion between the C6/7 vertebral bodies was noted. Associated atlantoaxial subluxation (atlantodental interval measuring 5.49 mm) and basilar invagination are also seen. (b) Sagittal computed tomography in bone window confirming the findings on plain radiograph. Note the wasp-waist appearance of the fused C6/7 vertebral bodies, suggesting a congenital fusion of the cervical spine rather than secondary causes (e.g., prior discitis and surgical fusion).
Chiari malformation
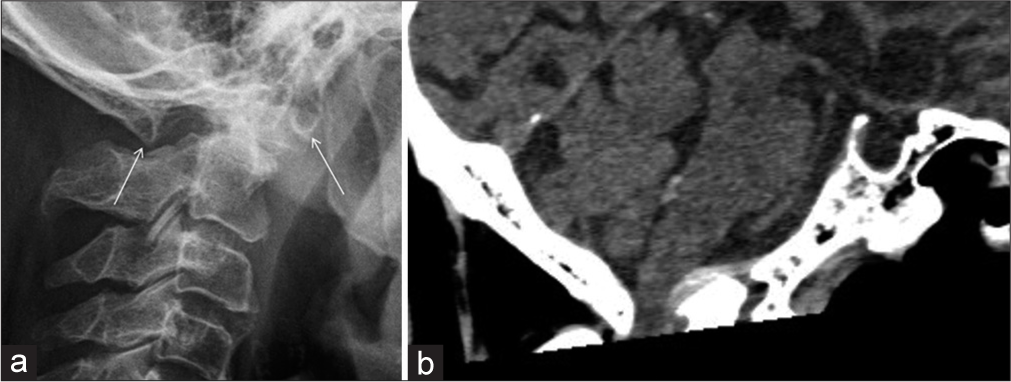
Atlanto-occipital assimilation can be associated with Chiari I malformation, which is characterized by the descent of the cerebellar tonsil through the foramen magnum into the upper cervical canal. The cerebellar tonsil would appear pointed, resembling a peg-like appearance [Figure 7]. Around 40% of the patients suffering from Chiari I malformation would develop cervical cord syrinx. This is particularly common when the patient is symptomatic.[8]
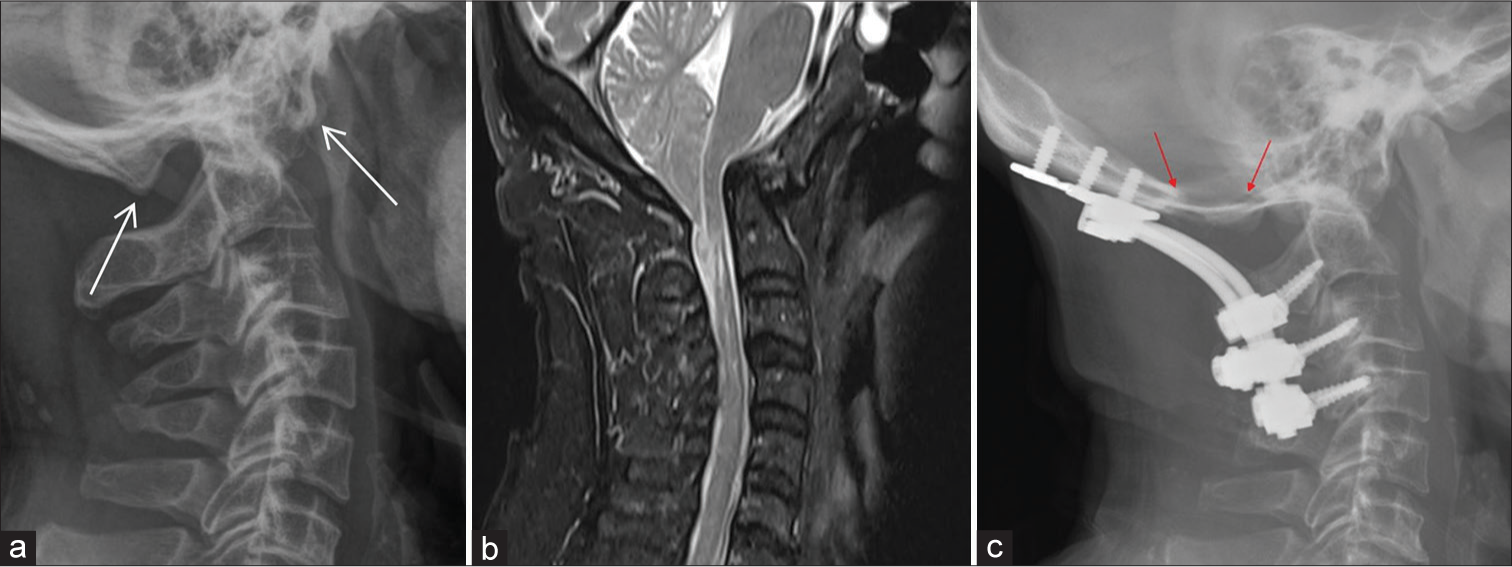
- (a) Plain radiograph of the cervical spine showing assimilation of anterior and posterior arches. (white arrows) Associated type 1 basilar invagination noted. (b) Sagittal T2-weighted magnetic resonance imaging of the same patient showing Chiari I malformation with descent of cerebellar tonsils beyond the foramen magnum. Note the peg-like configuration of the cerebellar tonsil. Associated compression on the cervicomedullary junction of the spinal cord was noted. There are also cord edema and syrinx formation. (c) Plain radiograph of the cervical spine of the same patient showing occipito-cervical fusion with metallic screws, plates, and rods. Occipitocervical fusion can provide atlantoaxial stability and is a procedure commonly performed for symptomatic atlanto-occipital assimilation. Also, notice the defect at the occipital bone (red arrows). The patient also had concomitant suboccipital craniectomy and expansile duroplasty for treatment of Chiari I malformation. The procedure is to create space for the herniated cerebellar tonsil since the pathogenesis of Chiari I malformation is believed to be due to a mismatch between the size and content of the posterior fossa (i.e., a congenitally small posterior fossa).
Chiari 1 malformation is postulated to be related to a mesodermal defect that causes a congenitally small posterior fossa, leading to overcrowding of its contents, subsequently resulting in tonsillar herniation.[9] As a result, surgical management by posterior fossa decompression (e.g., suboccipital craniectomy and expansile duroplasty) can be considered for patients with symptomatic Chiari I malformation. The aim of posterior fossa decompression is to expand the posterior fossa volume, thereby decompressing the cervicomedullary junction, re-establishing cerebrospinal fluid circulation, and reducing the size of the syrinx.[10,11]
Cervical compressive myelopathy
Although most cases of atlanto-occipital assimilation are asymptomatic, cervical cord compression can occur. Cervical cord compression is usually associated with basilar invagination, anteroposterior atlantoaxial subluxation, and Chiari malformation, as illustrated above [Figure 8].
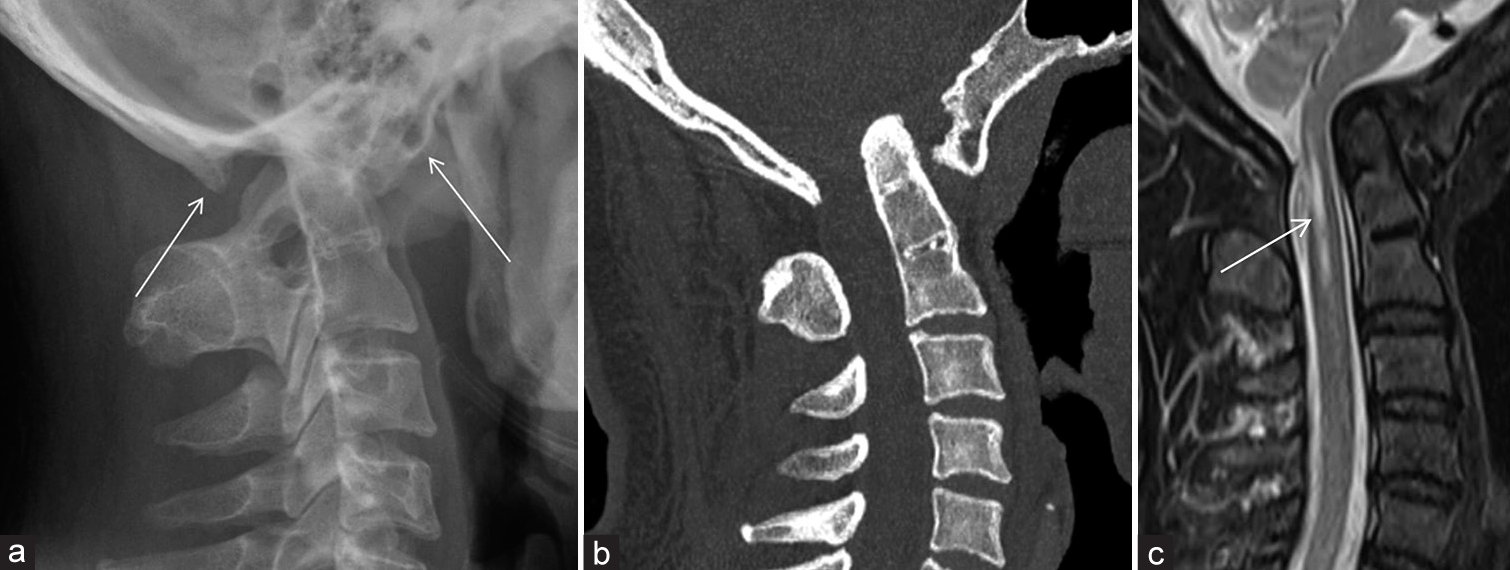
- (a) Lateral cervical spine radiograph showing assimilation of both the anterior arch and posterior arch of C1 (white arrows). Associated basilar invagination noted. Notice the relatively “elongated” appearance of the dens, raising suspicion for underlying C2/3 fusion. The cervical canal is markedly narrowed, worrisome of cord compression. (b) Sagittal computed tomography (CT) in bone window confirms the findings in the radiograph. Notice the fusion of C2 and C3 vertebral bodies and posterior elements. (c) Sagittal T2 weighted magnetic resonance imaging confirming findings in CT and plain radiograph. Compression on the cervicomedullary junction of the spinal cord was noted, with cord edema and syrinx formation seen (white arrow).
CONCLUSION
Atlanto-occipital assimilation is an entity that is easily missed in our daily reporting if not actively looked for. Aside from diagnosing it under dedicated imaging of the cervical spine, atlanto-occipital assimilation could also be incidentally diagnosed in the CT brain, where the atlanto-occipital joint may sometimes be partially included. Accurate reporting of atlanto-occipital assimilation is of clinical importance due to its association with atlantoaxial instability and cord compression. The following items are recommended to be mentioned while reporting cases of atlanto-occipital assimilation.
Type of atlanto-occipital assimilation (anterior arch assimilation/posterior arch assimilation/assimilation of both arches)
Presence of atlantoaxial instability (e.g., basilar invagination and anteroposterior atlantoaxial subluxation)
Presence of fusion of neighboring vertebral bodies (most commonly C2/3 congenital fusion)
Presence of complications (e.g., cord compression and Chiari malformation).
Acknowledgment
The authors would like to acknowledge Dr. Novena LS Cheng for offering refinement to the article.
Ethical approval
The Institutional Review Board permission was obtained for the study (Reference number: CIRB-2024-171-2).
Declaration of patient consent
Patient consent is not required as the patients’ identity is not disclosed nor compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Total occipitalization of the atlas. Anat Sci Int. 2006;81:173-80.
- [CrossRef] [PubMed] [Google Scholar]
- Complete atlantooccipital assimilation with basilar invagination and atlantoaxial subluxation treated non-surgically: A case report. Cureus. 2017;9:e1327.
- [CrossRef] [Google Scholar]
- Embryology and bony malformations of the craniovertebral junction. Childs Nerv Syst. 2011;27:523-64.
- [CrossRef] [PubMed] [Google Scholar]
- Atlas assimilation patterns in different types of adult craniocervical junction malformations. Spine (Phila Pa 1976). 2015;40:1763-8.
- [CrossRef] [PubMed] [Google Scholar]
- Angular craniometry in craniocervical junction malformation. Neurosurg Rev. 2013;36:603-10.
- [CrossRef] [PubMed] [Google Scholar]
- Atlantooccipital junction: Standards for measurement in normal children. AJNR Am J Neuroradiol. 1987;8:995-9.
- [Google Scholar]
- Klippel-Feil syndrome: Patterns of bony fusion and wasp-waist sign. Skeletal Radiol. 1993;22:519-23.
- [CrossRef] [Google Scholar]
- Chiari I malformations: Clinical and radiologic reappraisal. Radiology. 1992;183:347-53.
- [CrossRef] [PubMed] [Google Scholar]
- Neuroradiological diagnosis of Chiari malformations. Neurol Sci. 2011;32(Suppl 3):S283-6.
- [CrossRef] [PubMed] [Google Scholar]
- Accurate posterior fossa decompression technique for chiari malformation type I and a syringomyelia with navigation: A technical note. Int J Spine Surg. 2023;17:615-22.
- [CrossRef] [PubMed] [Google Scholar]
- A unifying hypothesis for hydrocephalus, Chiari malformation, syringomyelia, anencephaly and spina bifida. Cerebrospinal Fluid Res. 2008;5:7.
- [CrossRef] [PubMed] [Google Scholar]




