
Translate this page into:
Asymptomatic Thymic Cyst Appearing in the Neck on Valsalva: Unusual Presentation of a Rare Disease
Address for correspondence:Dr. PV Pradeep, Department of Endocrine Surgery, Narayana Medical College and Super Speciality Hospital, Chinthareddypalem, Nellore - 524 002, Andhra Pradesh, India pradeepputhenveetil@yahoo.co.in
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Thymic cysts are usually diagnosed accidentally during radiological evaluation of the chest for unrelated conditions. Symptoms appear late when the mass compresses on adjoining tissues. We report an unusual case of asymptomatic mediastinal thymic cyst which was seen in the neck whenever the patient was asked to perform Valsalva maneuver. This case is being reported for the unusual clinical presentation of a rare disease. The role of imaging in the diagnosis and common differential diagnoses are also discussed.
Keywords
Mediastinum
thymic cyst
valsalva maneuver

INTRODUCTION

Among the mediastinal cysts, thymic cysts have been reported to occur in about 3-28.6% of the cases.[1–3] These tumors are generally asymptomatic. They are usually diagnosed accidentally during radiological evaluation of the chest for unrelated conditions. Symptoms appear late when the mass produces compressive symptoms. The case reported here is unusual because the degree of superior herniation of the mediastinal thymic cyst was dramatic resulting in a palpable neck mass. Radiological workup was able to establish the nature of the mass for optimal surgical treatment planning.
CASE REPORT
Prior approval of the Ethical committee of the Narayana Hospital was obtained for publication of this case. A 13-year-old boy presented with an intermittent swelling in the lower neck. The neck swelling only appeared when the patient was asked to perform Valsalva maneuver [Figures 1a and b]. Mass was painful on Valsalva maneuver. The lower border of the mass was not palpable.
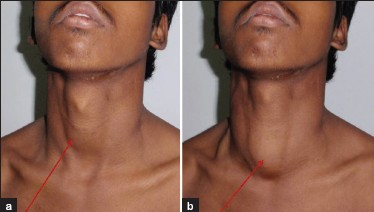
- (a) Photograph of the neck without Valsalva maneuver demonstrates
no neck mass. (b) Neck mass is observed when patient is asked to perform Valsalva maneuver
High-resolution sonography of the neck with the child performing Valsalva maneuver showed a well-circumscribed cystic mass with lobulated outlines, multiple small echogenic foci, and linear echogenic lines in the midline of the lower neck anterior to the cervical trachea [Figure 2]. The inferior portion of the mass could not be well delineated on sonography. MRI showed a cystic suprasternal mass continuous with the normal thymus in the anterior superior mediastinum [Figure 3]. The neck mass had a signal intensity that was hypointense on T1WI and hyperintense on T2WI images. The overall imaging appearances were of a thymic cyst with unusual superior herniation into the lower neck during Valsalva maneuver. Acetyl choline receptor antibody was negative. Intraoperatively a cystic lesion from the thymus extending to the lower neck was seen and excised [Figure 4]. Post-operative period was uneventful. Histopathology revealed the lesion to be a thymic cyst [Figure 5].

- Grayscale Ultrasound of neck in transverse view (a) without Valsalva maneuver and (b) with Valsalva maneuver demonstrates a cystic mass with internal low level echoes.
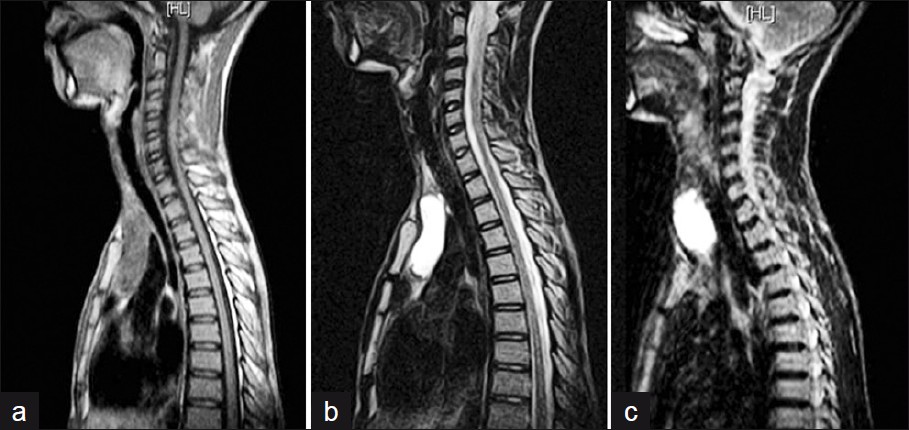
- MRI Saggital T1WI images show hypointense and T2WI hyperintense cystic lesion in the anterior mediastinum (a, b) without Valsalva maneuver and (c) with Vasalva maneuver.

- Intraoperative images (a) Partial sternotomy with excised thymus. (b) Complete specimen and the cut open cyst. (c) Closed cervical and sternotomy surgical incision.
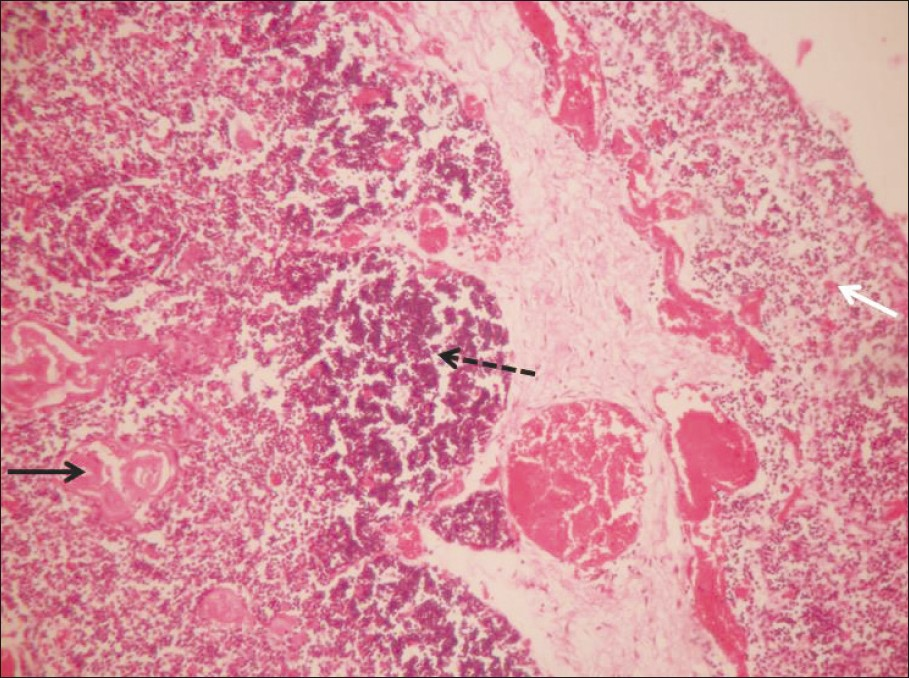
- Histopathology reveals the cyst wall with thymic tissue (white arrow), lymphoid aggregates (black arrow) and Hassals corpusceles (dashed arrow) (H and E, –100).
DISCUSSION
In the anterior mediastinum, tumors/ cysts of thymic origin, germ cell tumor, parathyroid adenoma, lymphoma, and intra thoracic goiters are prevalent.[1] The thymus develops from the third pharyngeal pouch together with the inferior parathyroid glands at the fifth week of gestation. The developing thymus maintains its close relation with the parietal pericardium and descends with the pericardium during 7-8 weeks of gestation to assume its characteristic location in the superior anterior mediastinum, anterior to the great vessels.[4] Thymic cysts may be congenital or acquired. Congenital thymic cysts (CTC) are remnants of the thyropharyngeal ducts and therefore can occur in the neck or mediastinum. CTC are usually < 6 cm, uniloculated or multiloculated and have thin walls; however, acquired cysts are multiloculated with variable cyst wall thickness and size ranging from 3 to 17cm.[5] In cases of thymic cyst with thymomas, the thymoma arises from the wall of the cyst. Radiologically thymic cysts manifest as well-circumscribed, uniloculated or multiloculated masses with septa and linear wall calcification.[1] The common symptoms mentioned for thymic cysts are chest pain, dyspnea, cough, and hoarseness of voice.[3] Hoarseness of voice and respiratory distress are rare presentation. Myasthenia gravis may be the presenting symptom in few cases. Malignant transformation has been reported in adults but not in children.
The differential diagnosis of midline anterior neck mass in children includes thyroglossal duct cyst, dermoid-epidermoid cyst, cystic hygroma, thyroid mass, and ectopic thymic mass.[6] The fact that the mass in this child occurred only during Valsalva maneuver virtually rules out all those possibilities. Laryngocele and phlebectasia may produce similar clinical presentation and can be easily differentiated from one another on imaging. Laryngocele, an abnormal dilatation of laryngeal saccule, can occur in children but is more common in adult men in the fifth decade. CT is the preferred imaging technique for evaluating laryngocele.[7] Phlebectasia is dilatation of an isolated vein which affects the internal jugular vein and the anterior jugular vein.[89]
Sonography supplemented by Doppler examination accurately identifies the dilated internal jugular vein on Valsalva maneuver with venous blood flow.[78] The diagnosis of superior herniation of thymic cyst in the neck in this child was made radiologically by virtue of its shape, location, continuity with the normal mediastinal thymus, absence of compression on adjacent structures on MRI, and characteristic sonographical appearances. Open procedure involving thoracotomy/ sternotomy and minimally invasive procedures like VATS/ mediastinoscopy are used for surgical removal.
In summary, symptomatic superior herniation of the mediastinal thymic cyst into the lower anterior neck during Valsalva maneuver is a rare condition. High-resolution sonography and MRI confirm the diagnosis. Surgeons and radiologists should be aware of this unusual clinical entity to enable further surgical management.
ACKNOWLEDGMENT
The authors acknowledge the contributions of Dr. Geetha S Nair, Postgraduate student, Department of Radio-diagnosis, and Dr. Shanthi Vissa Associate Professor, Department of Pathology, Narayana Medical College, in the preparation of the manuscript and data collection.
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/11/94026
REFERENCES
- Primary mediastinal tumors. Part 1. Tumors of the anterior mediastinum. Chest. 1997;112:511-22.
- [Google Scholar]
- Primary mediastinal cysts clinical evaluation and surgical results of 32 cases. Tex Heart Inst J. 2011;38:371-4.
- [Google Scholar]
- The pharyngeal apparatus. In: Moore KL, Persaud TVN, eds. The developing human: Clinically oriented embryology (7th ed). Saunders: Philadelphia PA; 2003. p. :202-40.
- [Google Scholar]
- Multilocular thymic cyst: An acquired reactive process. Am J Surg Pathol. 1991;15:388-98.
- [Google Scholar]
- Ectopic cervical thymic masses in infants: A case report and review of the literature. Int J Pediatr Otorhinolaryngol. 1998;43:77-84.
- [Google Scholar]
- Unilateral right-sided internal jugular phlebectasia in asthmatic children. J Paediatr Child Health. 2000;36:517-9.
- [Google Scholar]




