
Translate this page into:
Twin Reversed Arterial Perfusion Sequence: A Rare Entity
Address for correspondence: Dr. Sachin Khanduri, Department of Radiodiagnosis, Era's Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India. E-mail: drsaakshi02@gmail.com
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Twin reversed arterial perfusion (TRAP) sequence is an extremely rare complication of monochorionic multi-fetal pregnancy, occurring once in 35,000 births. This condition is characterized by a malformed fetus without a cardiac pump being perfused by a structurally normal (pump) twin via an artery-to-artery anastomosis in a reverse direction. We report a case of a primigravida, who came for routine antenatal checkup to our hospital at 31 weeks gestational age. Ultrasound imaging and magnetic resonance imaging revealed twin monochorionic intrauterine pregnancy with a viable, normal-appearing first twin and amorphous structured second twin connected by umbilical vessels. The patient was monitored with weekly ultrasonography, echocardiography, and Doppler ultrasound examination to ascertain the well-being of the pump twin. She delivered successfully at term a normal live baby and an acardius acephalus fetus. Plain X-ray of the acardius acephalus fetus confirmed the absence of cephalic structures. The perinatal mortality of the pump twin ranges from 35 to 55%; hence, it is essential to diagnose the presence of a pump twin at an early gestational age through improved imaging techniques, so that intervention can be planned early in the pregnancy for a better outcome of the pump twin.
Keywords
Magnetic resonance imaging
monochorionic twin pregnancy
pulsed Doppler
twin reversed arterial perfusion
ultrasonography

INTRODUCTION

Congenital anomalies are more common in multi-fetal pregnancy than in singleton pregnancy. Monozygotic twins increase the chance of anomaly because of reduced intrauterine space. One such congenital anomaly known as twin reversed arterial perfusion (TRAP) sequence is extremely rare. Although the first case was reported by Benedetti way back in 1533, very few cases have been reported in the literature since then.[1] The reported incidence is 1 in 35,000 births. Such complications arise in 1% of pregnancies with monozygotic twins.[1] The risk of recurrence is estimated to be 1:10,000.[2] TRAP sequence is characterized by a malformed fetus without a cardiac pump being perfused by a structurally normal pump twin via an artery-to-artery anastomosis in a reverse direction.[3] We report a case of a primigravida at 31 weeks of gestational age who came for a routine antenatal checkup to our hospital and underwent ultrasound and magnetic resonance imaging which revealed findings consistent with presence of a TRAP sequence twin.
CASE REPORT
A 22-year-old, 7-months pregnant primigravida visited the Department of Obstetrics and Gynecology of our hospital for routine antenatal checkup. Physical examination revealed distended abdomen with fundal height corresponding to 30–32 weeks of gestation. Multiple fetal parts were felt and a single fetal heart sound was auscultated below the umbilicus toward the left of midline. On per vaginal examination, the os was found to be closed with uneffaced cervix. Three months earlier, her first ultrasound scan taken at a peripheral hospital was misdiagnosed as a single live intrauterine fetus of 18 weeks gestational age. Later she was referred to the Department of Radiology, and the ultrasound images showed twin monochorionic, diamniotic intra-uterine pregnancy with a viable, normal-appearing first twin and amorphous structured second twin [Figure 1]. The placenta was located in the left lateral region of the upper uterine segment [Figure 1]. On further examination, the first twin showed normal morphology and growth with gestational age of 31 weeks in cephalic presentation. Fetal Doppler and echocardiography revealed normal parameters without any signs of cardiac failure in the first twin. The second twin showed disrupted growth and incomplete formation with absent head, upper limbs, heart, and thoracic structures. It had well-developed lower limbs and poorly developed lower abdomen with an abrupt ending at the top to form a blunt end. There was gross, diffuse soft tissue edema in the second twin [Figure 2]. Umbilical cord was seen entering the second twin with intact blood flow and pulsed Doppler study revealed reversal of the flow on the spectral pattern [Figure 3]. Ultrasound findings were consistent with TRAP sequence twin with an acardius acephalus which was confirmed on Magnetic Resonance Imaging. Magnetic resonance imaging showed twin monochorionic, diamniotic intrauterine pregnancy with the normally developed first twin in cephalic presentation on the left and malformed, small, grossly edematous second twin on the right with absent head, heart, upper limbs, and thoracic structures. The second twin had well-developed lower limbs and a part of lower abdomen with an abrupt ending at the top forming a blunt end. Also, a single placenta located in the left lateral region of the upper uterine segment was confirmed on Magnetic resonance imaging [Figure 4]. The patient was monitored with weekly ultrasonography, echocardiography, and Doppler examination for assessing the well-being of the pump twin. At no time during the follow-up did the fetal assessment demonstrate any evidence of complications like cardiac failure, hydrops, and polyhydramnios in the pump twin. She underwent cesarean section at 36 weeks of gestational age and delivered a normal live baby and another acardius acephalus twin. The acardius acephalus fetus was grossly edematous and showed tuft of coarse and lusterless hair in the midline at supraumbilical region [Figure 5]. Plain X-ray of the acardius acephalus fetus revealed normal lower limb bones, pelvic bone, lower vertebrae with the last four paired ribs, and an abrupt ending of bones above it confirming the absence of cephalic structures (i.e. head, heart, upper limbs, and thorax) [Figure 6].
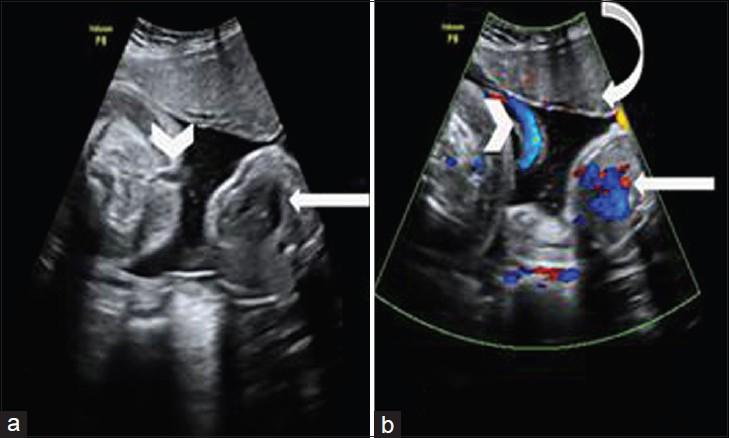
- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. (a) Transabdominal ultrasonography and (b) color flow US images reveal monochorionic, diamniotic twin gestation with a normal fetus showing heart (arrows) and the abnormal fetus showing umbilical cord (arrowheads) with a single placenta (curved arrow).
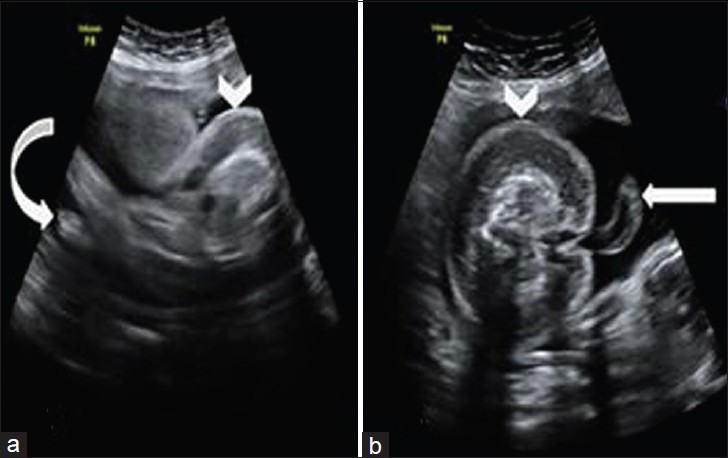
- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. Transabdominal ultrasonography scans (a) oblique and (b) axial views of abnormal fetus show well-developed lower limbs (curved arrow in a) with feet and umbilical cord (arrow in b), and diffuse, gross soft tissue edema (arrowheads).

- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. Pulsed Doppler ultrasound of the umbilical cord of the abnormal fetus shows flow reversal on the spectral pattern.

- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. (a and b) Magnetic Resonance Imaging T2-weighted coronal images of abdomen for fetal assessment show normal fetus (arrowheads) in cephalic presentation, with abnormal fetus demonstrating lower limbs with feet (arrows); absent head, upper limbs, thorax; and a single placenta (curved arrow) in the left lateral region of the upper uterine segment.
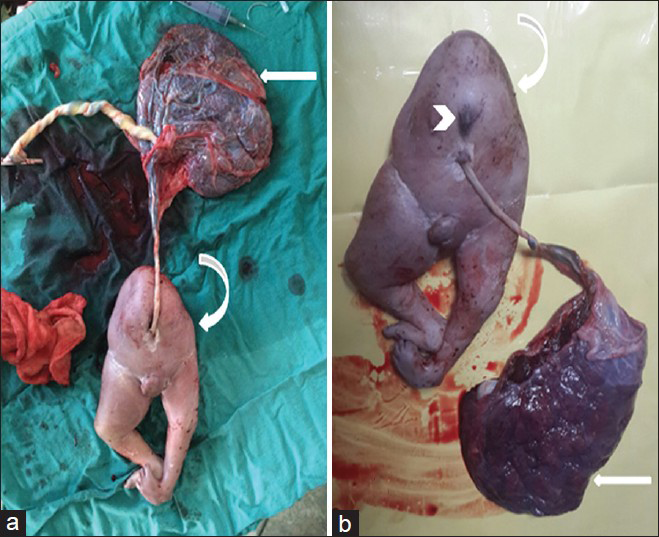
- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. (a and b) Post delivery day 1 photos of the acardius acephalus twin show the fetus with a single placenta (arrows) and two umbilical cords with grossly edematous, malformed fetus (curved arrows) showing tuft of coarse and lusterless hair in the midline at supraumbilical region (arrowhead).

- 22-year-old pregnant asymptomatic female who came for routine antenatal checkup, diagnosed with twin reversed arterial perfusion (TRAP) sequence pregnancy. Postoperative day 1 plain X-ray (infantogram) of acardius acephalus twin shows normal lower limb bones, pelvic bone, lower vertebrae, last four paired ribs (curved arrow) with absence of cephalic structures (head, heart, upper limbs, and thorax), and a single placenta (arrowhead).
DISCUSSION
TRAP sequence is an extremely rare congenital anomaly. It occurs once in 35,000 births.[1] It is also known as acardius or chorioangiopagus parasiticus, and is one of the forms of Twin-to-Twin Transfusion syndrome. TRAP results from artery-to-artery placental shunt and is often accompanied by a vein-to-vein shunt. The physiology behind the TRAP sequence is pumping of arterial blood in a retrograde fashion from the pump twin to the acardiac twin, rather than pumping into the placenta.[3] This poorly oxygenated blood preferentially perfuses the lower structures of the acardiac twin. Based on cephalic and truncal maldevelopment, the TRAP sequence is classified into four types. Acardiac acephalus is the most common type with no cephalic structures. Acardius anceps is the other type where some cranial structure and/or neural tissue are present. In acardius-acormus, cephalic structures are present without any truncal structures. Acardius amorphous is the least differentiated form with only a mass of tissue formed without any cephalic or truncal structure.[4] Various pathogenic theories have been proposed in the etiology of TRAP sequence, but the most widely accepted theory is the artery-to-artery anastomosis between the monochorionic twins in the first trimester causing abnormal circulation resulting in early tissue hypoxia leading to maldevelopment of the cardiovascular system in the recipient twin.[5] This diagnosis should be considered when during ultrasound imaging, there is monochorionic twin pregnancy and a fetus, which despite the absence of any definite cardiac activity, continues to grow. Lower extremities are well developed in contrast to upper extremities owing to perfusion by umbilical arteries. Arterial flow in the umbilical artery of acardiac twin makes the diagnosis certain. The pump twin may be normal or complicated with polyhydramnios, cardiac failure, or hydrops. The perinatal mortality of the pump twin has been reported to range from 35 to 55% owing to increased intrauterine volume leading to preterm delivery, cardiac failure, or intrauterine growth restriction due to hypoxia.[67] Needless to say, the rate of complications is directly proportional to the ratio of weight of acardiac twin to that of pump twin.
Several treatment modalities have been developed, with the recent trend being minimally invasive techniques targeting the vascular anastomosis between the twins under ultrasound guidance using fetoscopy or by hysterotomy. The vascular anastomosis can be interrupted by unipolar or bipolar diathermy, alcohol, cord coagulation, or cord embolization. Recently, intra-fetal laser therapy and radiofrequency ablation have been performed with reasonable success rates.[89] Though in the light of current available evidence it is difficult to determine the optimum management criteria, most authors still advocate prophylactic intervention early in the pregnancy for improved outcomes as there are many technical challenges in late intervention.[10]
CONCLUSION
TRAP sequence is an extremely rare congenital anomaly complicating monochorionic multiple gestation. Accurate and early antenatal diagnosis is absolutely essential for better prognosis. A radiologist should have a high index of suspicion during ultrasound imaging if there is monochorionic twin pregnancy with a fetus which, in spite of absence of cardiac activity, continues to grow. Modern imaging techniques like ultrasonography and transvaginal Doppler ultrasonography offer the advantage of diagnosing this rare entity even in the first trimester, thereby improving the prognosis. Though many patients can benefit from conservative treatment, recent trend toward using minimally invasive treatment modalities for the vascular anastomosis has been a boon in improving the outcome of the pump twin.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2015/5/1/9/152341
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Twin reversed arterial perfusion (TRAP) sequence: (Acardius Amorphous) a case report and review of literature. Int J Biol Med Res. 2012;3:1453-5.
- [Google Scholar]
- Twin reversed arterial perfusion (TRAP) sequence: A study of 14 twin pregnancies with acardius. Semin Perinatol. 1983;7:285-93.
- [Google Scholar]
- MRI findings in multifetal pregnancies complicated by twin reversed arterial perfusion sequence (TRAP) Pediatr Radiol. 2011;41:694-701.
- [Google Scholar]
- Twin reversed arterial perfusion sequence in twin- to-twin transfusion syndrome after the death of the donor co-twin in the second trimester. Ultrasound Obstet Gynecol. 2001;17:153-6.
- [Google Scholar]
- Perinatal outcome of forty-nine pregnancies complicated by acardiac twinning. Am J Obstet Gynecol. 1990;163:907-12.
- [Google Scholar]
- The outcome of twin reversed arterial perfusion sequence diagnosed in the first trimester. Am J Obstet Gynecol. 2010;203:e1-4.
- [Google Scholar]
- Intrafetal laser treatment for twin reversed arterial perfusion sequence: Cohort study and meta-analysis. Ultrasound Obstet Gynecol. 2013;42:6-14.
- [Google Scholar]
- The use of radiofrequency in the treatment of twin reversed arterial perfusion sequence: A case series and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2013;166:127-32.
- [Google Scholar]
- Early vs late intervention in twin reversed arterial perfusion sequence. Ultrasound Obstet Gynecol. 2014;43:60-4.
- [Google Scholar]




