
Translate this page into:
Limited Utility of Plain Abdominal Radiographs in Evaluating Intussusceptions Secondary to Long Indwelling Feeding Tubes
Address for correspondence: Dr. Chandana Lall, Department of Radiology, 101 The City Drive South Orange, CA, USA. E-mail: clall@uci.edu
-
Received: ,
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Adult intussusception (AI) is relatively rare and can be a difficult clinical diagnosis, often requiring cross-sectional imaging for confirmation. Unfortunately, intussusceptions in the setting of indwelling long enteral feeding tubes have been predominantly characterized in the pediatric population with minimal investigation in adults. We report three cases of AI in patients with long feeding catheters serving as anatomic lead points leading to intussusception diagnosed on cross-sectional imaging. We highlight the limited utility of the supine plain films for detection of AI, and it behooves the radiologist to hold a high index of suspicion if the patient has a long enteral catheter. Since the majority of these patients tend to be fairly ill and unable to stand for upright abdominal radiographs, in the setting of percutaneous feeding tubes, decubitus abdominal radiographs should always be obtained. These cases also highlight the importance of having a high clinical suspicion of intussusceptions in a patient presenting with abdominal pain in the setting of an enteral feeding tube. In post-operative patients, other factors can predispose the patient to intussusception, including adhesions. Another interesting feature in tube related AI is the reverse intussusception that may be seen with indwelling enteral tubes. Reverse intussusception is where the distal bowel telescopes into the proximal segment over the tube.
Keywords
Adult intussusceptions
gastrojejunostomy tubes
percutaneous jejunostomy

INTRODUCTION

- Albert Yang
Intussusception refers to the telescoping of a segment of intestine into the adjoining intestinal lumen. The portion of the intestine that invaginates into the other is termed the “intussusceptum,” whereas the portion that envelopes is called the “intussuscipiens.” In most intussusceptions, the proximal bowel segment telescopes into the distal segment due to the motion of the peristaltic wave pushing forward whereas reverse intussusception may be seen with indwelling enteral tubes i.e., the distal bowel telescoping into the proximal segment over the enteral tube.
Intussusception is largely thought to be a pediatric entity, but up to 5% of cases occur in adults.[1] Pediatric cases often are idiopathic, as compared to adults, where intussusception typically results from mucosal, intramural, or extrinsic lead points.[2] Organic lesions are found roughly in 70-90% of cases in adults.[3] Diagnosis of intussusceptions in adults is difficult due to the fact that clinical presentation may be nonspecific, often prompting further evaluation with abdominal films and computed tomography (CT). A retrospective review of adult intussusceptions (AI) illustrated that 20% of patients were asymptomatic and the most common presenting symptom in 72% of patients was abdominal pain.[4] Though AIs are mostly associated with anatomic lead points, rarely post-operative functional intussusceptions can occur in up to 0.08-0.5% of laparatomies. The mechanism is principally thought to be due to differential motility between intestinal segments recovering from ileus.[5]
CASE REPORTS
Case 1
A 74-year-old male with history of pancreatitis initially presented with jaundice, abdominal pain, distention, and diarrhea. Abdominal ultrasound and CT indicated a prominent pancreatic head, but no definite mass was demonstrated. An endoscopic ultrasound and endoscopic retrograde cholangiopancreatography showed evidence of a pancreatic head mass measuring about 3.3 cm with dilated pancreatic and common bile ducts. Fine needle aspiration showed adenocarcinoma. Endoscopic staging of pancreatic adenocarcinoma was T3N0Mx. The patient subsequently received neoadjuvant chemotherapy and a Whipple procedure. A feeding gastrojejunostomy tube was placed post-operatively. Initially the patient was recovering well, until he developed emesis, profound electrolyte abnormalities, and increased tube outputs. Sequential kidney, ureters, and bladder radiographs in the intensive care unit showed only mild proximal small bowel dilatation, and reported a probable ileus pattern likely due to pain medication [Figure 1]. With escalation of symptoms, CT scan was performed, which showed long segment entero-enteric intussusception with the gastrojejunal feeding tube acting as a lead point [Figure 2]. This prompted immediate exploratory laparotomy. The surgeon did not find evidence for necrotic bowel upon exploration and the tube was then removed. An intra-operative image shows the unreduced intussusception with tube still in place [Figure 3].
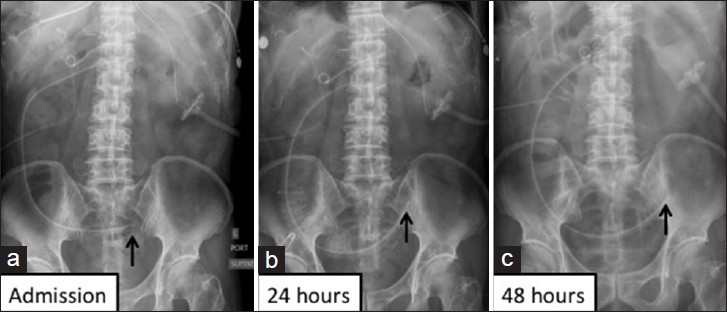
- Case 1: Sequential abdominal radiographs show mild proximal small bowel dilatation reported as post-operative ileus: (a) On admission, (b) 24 hours later and (c) 48 hours later. Black arrow indicates the distal tip of the percutaneous jejunostomy feeding tube in all sequential radiographs.
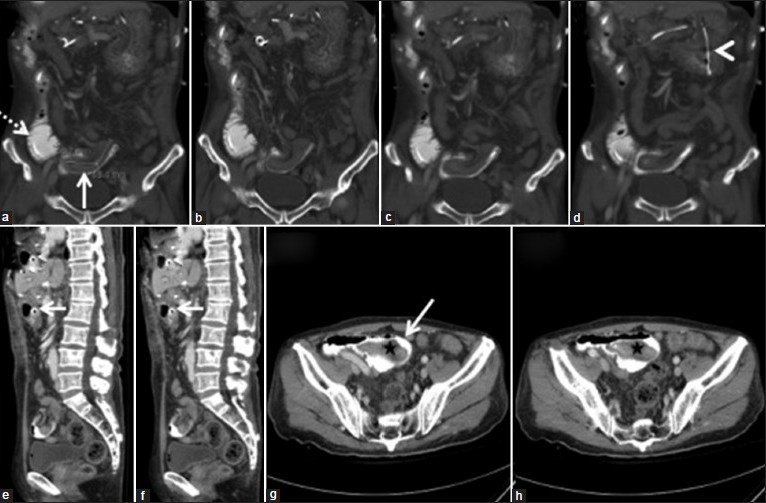
- Case 1: (a - d) Coronal CT slices with contrast via feeding tube, progressing from posterior to anterior of the patient, demonstrating the intussusception with the GJ tube as an anatomic lead point (Figure 2a, dashed white line). The white solid line (Figure 2a) depicts the distal portion of the intussusception and arrowhead in d points to the tube. (e and f) Sagittal images that show intussusception in the distal small bowel. (g and h) Axial CT images of the abdomen that show a loop of distal small bowel (star) engulfed within another segment (Figure g, white arrow).
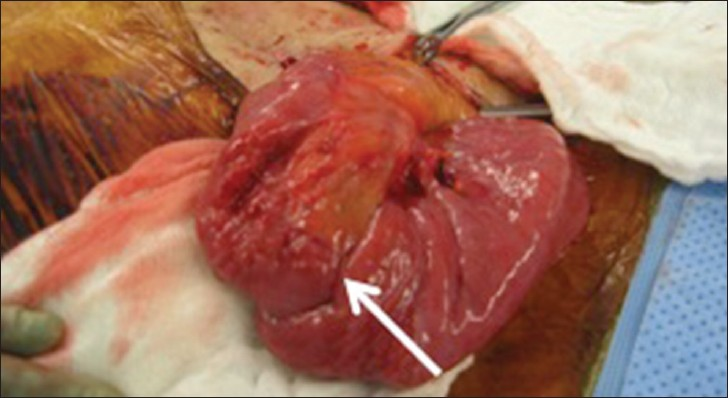
- Case 1: Gross specimen shows a reverse long segment intussusception with distal bowel telescoping into a proximal segment (white arrow).
Case 2
A 55-year-old male with initial presentation of dysphagia, weight loss, nausea, and a long history of smoking was diagnosed with distal esophageal adenocarcinoma. He was treated with surgical resection and gastric pull-up procedure. A percutaneous jejunostomy feeding tube was placed post-operatively. The patient was tolerating tube feeds well until about 2 months later when he presented with diffuse abdominal pain. No palpable masses were felt on physical exam. Abdominal radiographs showed no features of obstruction [Figure 4]. Since symptoms were progressive, CT imaging was ordered and showed the distal tip of the percutaneous jejunostomy tube acting as an anatomic lead point for longer length intussusceptions [Figure 5a and b]. The tube was subsequently removed by surgery.
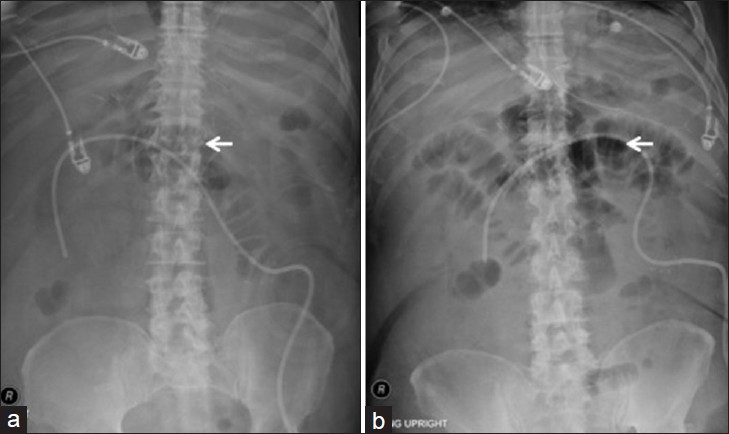
- Case 2: (a) Supine and (b) semi-upright abdominal radiographs demonstrate scattered, mildly dilated small bowel loops without significant air fluid levels. Radiographs read as mild ileus pattern. Due to progression of abdominal pain, CT of the abdomen and pelvis was ordered, which illustrated a long loop intussusception over the percutaneous jejunostomy feeding tube. The feeding tube was a Kendel 12 French feeding jejunostomy tube.
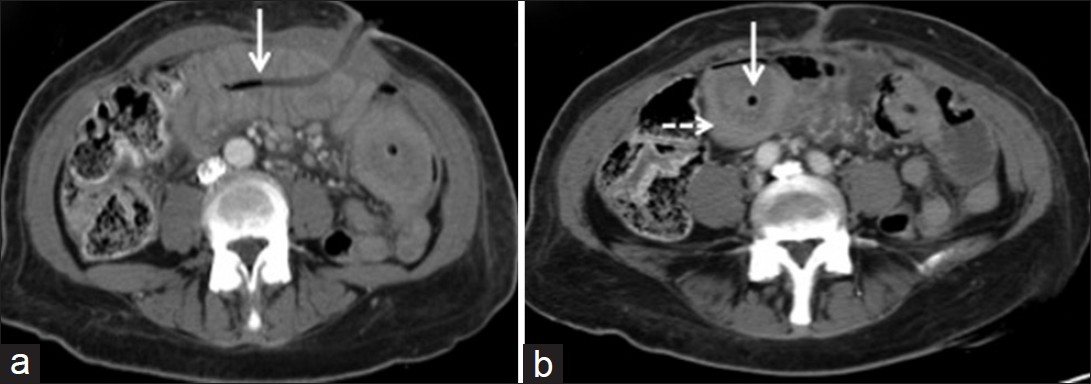
- Case 2: (a and b) Axial CT images, with IV contrast introduced peripherally and without bowel contrast. CT images of the patient demonstrate distal tip of the percutaneous jejunostomy tube (white arrow) within the distal small bowel. Figure 5b illustrates a lower attenuating surrounding area around the tip (white arrow). Encircling that focal area is a larger bowel segment (intussuscipiens) with higher attenuation (dashed white arrow).
Case 3
A 73-year-old male with numerous prior abdominal surgeries for bladder adenocarcinoma developed poor nutritional status in a nursing home facility. Patient initially had a gastrostomy tube, which then became subject to “buried bumper syndrome” with overgrowing gastric mucosa and subsequently received a percutaneous jejunostomy tube for nutritional purposes. Patient presented with abdominal pain and had a portable supine abdominal radiograph [Figure 6a], which showed presence of a percutaneous feeding jejunostomy catheter without significant bowel dilatation. Due to persistent patient discomfort, a CT scan of the abdomen and pelvis was performed with introduction of bowel contrast via jejunostomy tube [Figure 6b–e]. This showed a long segment intussusception over with the jejunostomy tube acting as the lead point [Figure 6c, black arrow indicating tip of J tube]. This feeding tube was a 9 French Kimberly-Clark jejunostomy feeding tube. This patient also had the feeding tube subsequently removed via surgery.
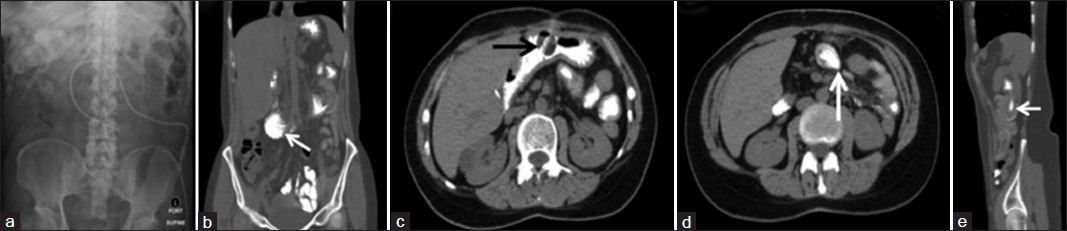
- Case 3: (a) Supine abdominal film, shows mildly dilated small bowel in the left upper abdomen. (b) Coronal CT image depicts the percutaneous tube within a distal segment of small bowel. (c and d) Axial CT images of the abdomen. Figure 6c shows the intussusception (black arrow). Figure 6d (white arrow) shows the tube at a higher level. (e) Sagittal CT characterize the intussusception again (note that in this sagittal image the abdominal entry point of the tube is not visualized).
DISCUSSION
There is a noticeable difference between adult proximal versus adult distal small bowel intussusceptions. 80-90% of cases of distal small bowel intussusceptions are predominantly related to anatomic lead points. Examples of these lead point lesions include benign polyps, lipomas, carcinoids, a Meckel diverticulum, gastrointestinal stromal tumor, lymphoma, and melanoma metastases. Conversely, intussusceptions in the proximal small bowel tend to be short segment and transient, usually requiring no specific treatment and occurring without a lead point mass.
Studies have elucidated upon the clinically insignificant, incidental finding of asymptomatic short segment enteric intussusception upon CT imaging, which frequently resolved without intervention.[6] Out of 26 reported patients, 22 resolved spontaneously and upon follow-up imaging no intussusception persisted. Past studies warn against aggressive intervention for incidental findings of AI due to an often seen transient nature. Moreover, these case reports did not have a probable lead point or etiology and were deemed as idiopathic by their authors. In contrast to these findings, we propose that the threshold for recommendation to treat should be lowered if the patient has an indwelling feeding tube. We base this upon these three cases, which demonstrated persistence of intussusception as long as the tube was in place with resolution upon removal.
In the setting of long feeding enteral catheters, the feeding tube acts as anatomical lead point for intussusception. These intussusceptions are long length and generally irreversible, typically requiring surgical intervention. Studies state that there is a positive correlation between increasing caliber of the tube and the probability of intussusceptions.[7] The most common complication limiting the use of gastrojejunal feeding tubes is distal tip migration, which can play a significant factor in initiating the intussusception. AIs may manifest clinically with intermittent abdominal pain and minimal physical findings.
Plain abdominal radiographs may actually downplay the severity of the process, confounded by the fact that most post-operative patients are on high-dose pain medication and tend to have electrolyte abnormalities leading to an erroneous diagnosis of small bowel ileus as in these cases. In these cases, overt obstructive features and significant intestinal distention were not present.[8]
This case series reveals the ambiguity and scarce plain film findings in AI, limiting the utility of this study in adults. We demonstrate that intussusception in adults potentially requires meticulous evaluation with CT, even without findings on abdominal plain films due to the inability to make the diagnosis on plain films. This is in contrast to reports in pediatrics that claim plain radiography as a viable modality for evaluation of intussusceptions, especially in the setting of ischemia.[910]
CONCLUSION
AIs have been poorly characterized especially in the setting of indwelling intestinal catheters as compared to the pediatric population. Unclear and minimal plain film findings were exhibited in these cases and provide a lesson to radiologists to carry a higher index of suspicion when evaluating these films in the presence of existing long feeding enteral tubes. Furthermore, we question the utility of the plain film, in light of a more definitive diagnosis provided with CT in all three cases. Radiologists also should be cognizant that indwelling catheters often migrate, which can allow interval resolution of intussusception, thereby minimizing symptoms and radiographic findings as well. Additionally, we theorize that a post-operative patient with a feeding tube may have higher predisposition for development of intussusceptions due to altered peristalsis, electrolyte derangements with motility issues and adhesions, which increase the risk of this process.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/1/9/107994
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Radiology case of the month: Two adults with intermittent abdominal pain. J La State Med Soc. 2012;164:160-1. 163
- [Google Scholar]
- Intussusception in adults: What radiologists should know. Emerg Radiol. 2012;19:89-101.
- [Google Scholar]
- Adult intussusception: Presentation, management, and outcomes of 148 patients. J Emerg Med. 2012;43:1-6.
- [Google Scholar]
- A special type of postoperative intussusception: Ileoileal intussusception after surgical reduction of ileocolic intussusception in infants and children. J Pediatr Surg. 2009;44:755-8.
- [Google Scholar]
- Proximal small bowel intussusceptions in adults: CT appearance and clinical significance. Abdom Imaging. 2004;29:653-7.
- [Google Scholar]
- Further report of small-bowel intussusceptions related to gastrojejunostomy tubes. Pediatr Radiol. 2000;30:614-7.
- [Google Scholar]
- Limitations and uses of gastrojejunal feeding tubes. Arch Dis Child. 2002;86:134-7.
- [Google Scholar]
- The role of plain radiography in assessing intussusception with vascular compromise in children. Arch Med Sci. 2011;7:877-81.
- [Google Scholar]
- The role of abdominal x-rays in the diagnosis and management of intussusception. Pediatr Emerg Care. 1992;8:325-7.
- [Google Scholar]




