
Translate this page into:
Large Vallecular Masses; Differential Diagnosis and Imaging Features
Address for correspondence: Dr. Ashim Kumar Lahiri, Department of Radiology, Worcestershire Royal Hospital, WR5 1DD, UK. E-mail: ashim_lahiri@hotmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Large vallecular masses are an uncommon disease entity which includes a wide spectrum of rare pathologies. These masses may present as purely vallecular in location or appear as an extension from adjacent anatomical sites like tongue base including lingual tonsils, epiglottis, palatine tonsils, epiglottis, and the remainder of supraglottis. Literature review reveals very rare conditions presenting as vallecular mass lesions. The imaging features are generally diagnostic for characterization. However, these masses can exhibit indeterminate appearance at imaging. We present a series of five cases which includes two rare presentations: a case of low-grade cribriform adenocarcinoma of the base of tongue and a vallecular lipoma. The other three cases presented for differential diagnosis including benign vallecular cysts and two cases to show that malignant masses arising from neighboring anatomical sites such as tongue base or supraglottic larynx can exhibit significant vallecular component.
Keywords
Cysts
magnetic resonance imaging
masses
vallecula


INTRODUCTION
The valleculae are essentially potential spaces seen anterior to the epiglottis which contains mainly lymphoid or glandular tissues. The benign mucous retention cysts are the most common vallecular lesions encountered which are generally small, mostly detected incidentally and remain asymptomatic. However, predominantly, large vallecular masses are rare presentations which include uncommon types of large mucous (ductal) cysts and malignant masses originating from tongue base or supraglottis. The other causes include a group of very rare low-grade malignant lesions of minor salivary glands, uncommon benign developmental vascular anomalies, lipomas, dermoid, and epidermoid.[12] These patients can remain asymptomatic or rarely manifest with serious acute airway obstruction. Computed tomography (CT) and magnetic resonance imaging (MRI) are the main imaging modalities to characterize these lesions, to establish the origin of the tumor, and to delineate the extent of disease. MRI is significantly more sensitive and accurate in soft-tissue characterization.[3] The purpose of this article is to illustrate that extreme uncommon varieties of malignant masses and some benign tumors can present as large vallecular masses and to reveal that oropharyngeal and laryngeal malignancies can as well show significant component of tumor in the vallecular spaces.
CASE REPORTS
Case 1
A middle aged patient previous smoker, presented with a hoarse voice and high dysphagia. Endoscopy revealed left vallecular mass displacing epiglottis. MRI neck with contrast revealed a large well-defined left vallecular mass (45 mm × 30 mm) with the intermediate signal on T1-weighted, homogeneously hyperintense on T2-weighted images (arrows). There was no diffusion restriction or appreciable contrast enhancement. This mass was seen slightly focally abutting the tongue base and distorting the epiglottis. There were no other sinister features or cervical lymphadenopathy. MRI findings were considered possibly benign. Histopathology confirmed low-grade cribriform adenocarcinoma of tongue base [Figure 1].
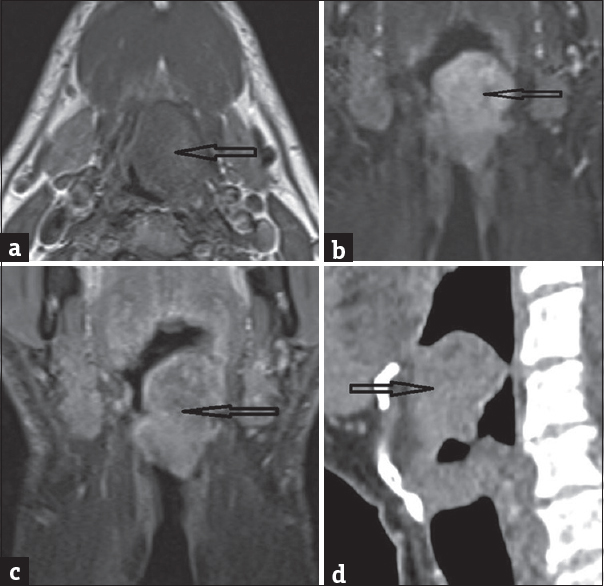
- A 63-year-old male patient presented with a history of hoarseness of voice and dysphagia. This mass appears well circumscribed shows the intermediate signal onT1W axial image (a), hyperintense at T2-short tau inversion recovery coronal image (b), no contrast-enhancement at the post-contrast fat-saturated image (c) and sagittal computed tomography shows mass separate from tongue base (d).
Case 2
An elderly nonsmoker patient presented with few months history of altered voice and dysphagia. ENT examination showed a huge cyst on the posterior aspect of tongue/laryngeal inlet region. MRI neck with contrast showed a large pure fat density mass lesion (40 mm × 36 mm) involving the vallecula with tubular extensions into the floor of the mouth. This mass showed uniform suppression of high signal at the T1 fat-saturated image, did not reveal any edema, contrast enhancement or diffusion restriction. The imaging findings were consistent with a large vallecular lipoma [Figure 2]. The patient did not opt for surgery due to other comorbidities and is stable under follow-up.
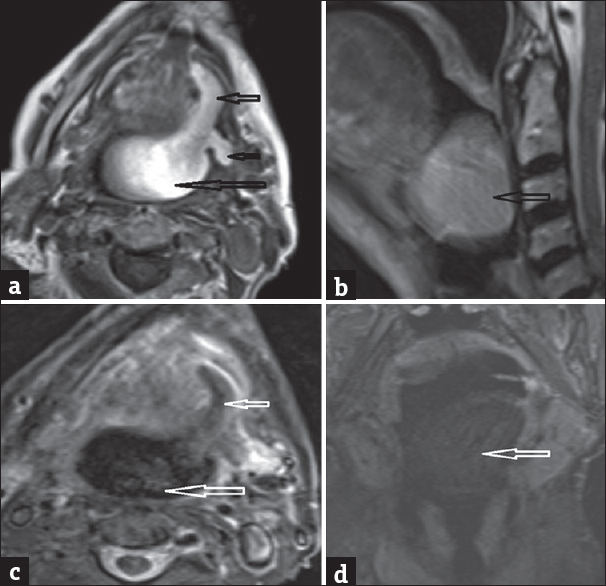
- An 84-year-old female patient presented with altered voice and dysphagia. Magnetic resonance imaging neck with contrast demonstrates a well-demarcated lesion with uniform hyperintensity on axial T1-weighted (a), homogeneous hyperintensity at T2-weighted sagittal (b) (arrows), suppression of signal on T2-short tau inversion recovery axial (c) and no contrast-enhancement with fat suppression on post-contrast coronal fat-saturated T1-weighted coronal (d).
Case 3
An elderly patient underwent MRI neck for the evaluation of a parotid lump which revealed an incidental 20-mm left vallecular cyst and a 10-mm right vallecular cyst. Both showed features of the benign cyst without any diffusion restriction or contrast-enhancement [Figure 3]. The patient was asymptomatic without any obstructive features.

- An 80-year-old male patient was referred for magnetic resonance imaging neck which showed an incidental 20 large vallecular cyst on the left and a 10-mm cyst on the right (arrows). This lesion appears well defined, reveals intermediate signal on T1-weighted axial image (a), homogeneous hyperintensity on T2-weighted axial (b) and T2-weighted coronal (c) and no contrast enhancement was revealed (d).
Case 4
A middle aged patient chronic smoker presented with few months history of progressive soreness of the throat and right-sided throat pain. ENT examination revealed a large supraglottic tumor, predominantly involving the vallecula and epiglottis extending to the aryepiglottic fold. MRI neck with contrast showed a large supraglottic tumor, primarily involving the epiglottis and vallecula. The inferior component of the tumor is seen involving the right aryepiglottic fold with obliteration of the right piriform sinus [Figure 4]. Subsequently, histopathology confirmed squamous cell carcinoma.

- A 54-year-old female chronic smoker presented with few months history of progressive soreness of throat and right-sided throat pain. magnetic resonance imaging neck with contrast reveals a supraglottic tumor (47 mm × 20 mm × 30 mm) with large right vallecular component and supraglottic involvement with obliteration of right piriform sinus (arrows) on T2-weighted axial (a), marked infiltration with thickening of the epiglottis on T2-weighted sagittal (b), thickening of right aryepiglottic fold and tumor enhancement at post-contrast coronal fat-saturated T1 coronal (c).
Case 5
A middle aged patient presented with left neck lump and examination revealed a large vallecular mass with suspected tongue base malignancy. Subsequently, MRI revealed a large left vallecular mass crossing to the right. The mass is seen originating from the tongue base with the bulk of the tumor appears exophytic. Large left neck metastatic nodes also seen [Figure 5]. Histopathology confirmed squamous cell carcinoma.

- A 52-year-old male presented with left neck lump and examination revealed a large vallecular mass with suspected tongue base malignancy. Axial T1-weighted (a), axial T2-short tau inversion recovery (b) and postcontrast fat-suppressed image (c) demonstrate large left vallecular mass arising from tongue base (arrows). Note of large left level-II lymph node (star).
DISCUSSION
The valleculae are essentially potential spaces, seen as depressions anterior to the epiglottis, forming the floor of the oropharynx and serve to collect the saliva. The median glossoepiglottic fold separates the two, and laterally, the valleculae are bound by the lateral glossoepiglottic folds.[34] The literature describes the vallecula as an anatomic term for a crevice, furrow, or depression. However, when used alone, the term “;valleculae” also indicates epiglottic valleculae. MRI and CT are the two most important and most widely used imaging techniques to investigate these oropharyngeal masses. MRI is extremely sensitive in tissue characterization, assessing the submucosal soft tissues, perineural spread, early bone marrow infiltration, intracranial spread, and to detect recurrence.[13]. The MRI and CT protocols followed in our institution are shown in Table 1.
Vallecular mass lesions are uncommon disease entities with benign cysts being the most commonly encountered vallecular lesion by the otolaryngologists. The vallecular cysts are also called ductal cysts, laryngeal cysts, lymphoepithelial cysts, and mucous retention cysts.[56] These supraglottic cysts account for 10%–20% of all laryngeal cysts which generally arise from the lingual surface of the epiglottis and are thought to develop due to blockage of submucosal ducts as the vallecula show abundant lymphoid and glandular tissues. These cysts are often symptomatic in childhood with the likelihood of serious complications causing obstructive stridor or feeding problems. The airway management in this scenario may be a challenge to the anesthesiologist regarding intubation.[56] In adults, these cysts are often bilateral, mostly small, generally remain asymptomatic and are detected incidentally at imaging or during clinical examination. Imaging reveals characteristic well defined, unilocular nonenhancing, fluid-density benign cysts without any invasive features [Table 2]. Rarely, even in adults, these cysts can attain large size and cause respiratory obstructive symptoms. Case-3 of our series reveals a fairly large benign left vallecular cyst which was detected incidentally at MR imaging [Figure 3].
The other very rare causes of benign vallecular masses include lingual thyroid cysts, thyroglossal cysts, and mass lesions originating from tongue base; minor salivary gland tumors, schwannoma, lipoma, lymphangioma, hemangiomas, dermoid, and epidermoid. Similarly, wide range of rare granulomatous, infectious, and neoplastic conditions of epiglottis can manifest as vallecular mass lesions.[127]
Vallecula is an extremely rare site of lipoma, and very few cases are reported in the literature. Overall, the oropharyngeal lipomas constitute 1%–4% of this condition and mostly seen to involve cheek, lips, and floor of mouth, rarely at the vallecula. These are characteristically slow-growing lesions with rare possibility of malignant transformation, and large lipomas carry the risk of airway obstruction.[8] Case-2 of our series shows a typical large vallecular lipoma which showed characteristic features at MR imaging with homogeneous pure fat signal [Figure 3]. The diagnosis was straightforward as this mass did not reveal any restriction of diffusion which is a feature of epidermoid, it lacked typical cystic features of a vascular malformation, lacked typical features of a nerve-related tumor and there were no suggestive malignant findings.
Overall, malignant mass lesion presenting predominantly as a vallecular mass is an uncommon condition, and these malignant masses mostly originate from tongue base and uncommonly also arise from supraglottis including epiglottis. More commonly, the vallecular tumor component is likely to coexist with the primary oropharyngeal or laryngeal tumor without posing any diagnostic challenge.[34] The fourth and fifth cases of this series illustrate primary squamous cell carcinoma arising from base of tongue and supraglottis, respectively, presenting as significant dominant vallecular mass components.
The very rare malignant vallecular masses reported in the literature include cribriform adenocarcinoma of tongue base and minor salivary glands which was first described about 18 years ago and was defined as a possible variant of polymorphous low-grade adenocarcinoma.[910] This abnormality presents as a mass at the base of the tongue with early spread to lymph nodes, but without the potential for distant metastases. Our first case reveals an interesting case of low-grade cribriform adenocarcinoma of the base of tongue, presenting as a large nonenhancing vallecular mass without any sinister features or lymphadenopathy at imaging. This mass was suspected to represent a likely benign entity, but histopathology revealed an extremely rare disease condition. Other similar infrequent types of malignant vallecular mass lesions described in the literature include clear cell carcinoma and myoepithelial carcinoma of minor salivary glands.[2] The MR imaging features were diagnostic which accurately revealed the extent of disease. The typical imaging feature of various vallecular masses is described in Table 2.
CONCLUSION
Large, purely valleculla-based mass lesions are a rare disease entity. Understanding the various differential diagnoses and interpreting the imaging findings are crucial for diagnosis and treatment planning. Extreme uncommon varieties of low-grade malignant tumors of the minor salivary gland can reveal more benign features.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2018/8/1/26/235510.
REFERENCES
- Clear cell carcinoma of the base of the tongue: MR imaging findings. AJNR Am J Neuroradiol. 2007;28:127-8.
- [Google Scholar]
- Epiglottic masses identified on CT imaging: A case report and review of the broad differential diagnosis. Neuroradiol J. 2015;28:347-53.
- [Google Scholar]
- Oral cavity and oropharyngeal squamous cell cancer: Key imaging findings for staging and treatment planning. Radiographics. 2011;31:339-54.
- [Google Scholar]
- A case report of a vallecular cyst and literature review. J Oral Maxillofac Surg. 2015;73:1766e1-4.
- [Google Scholar]
- Bilateral vallecular cysts as a cause of dysphagia: Case report and literature review. Int J Otolaryngol. 2010;2010:697583.
- [Google Scholar]
- Tongue base schwannoma: Differential diagnosis and imaging features with a case presentation. Radiol Case Rep. 2016;11:336-40.
- [Google Scholar]
- Lipoma of vallecula – A case report. 2016. BJR Case Rep. 2 Available from: https://doiorg/101259/bjrcr20150460
- [Google Scholar]
- Cribriform adenocarcinoma of the tongue and minor salivary gland: Transoral robotic surgical resection. ORL J Otorhinolaryngol Relat Spec. 2015;77:87-92.
- [Google Scholar]
- Cribriform adenocarcinoma of the tongue and minor salivary glands: A review. Head Neck Pathol. 2013;7(Suppl 1):S3-11.
- [Google Scholar]




