
Translate this page into:
Lingual Foramina and Canals of the Mandible: Anatomic Variations in a Lebanese Population
Address for correspondence: Dr. Georges Aoun, Department of Oral Pathology and Diagnosis, Faculty of Dental Medicine, Lebanese University, Beirut, Lebanon. E-mail: aoungeorges@yahoo.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
The aim of this study was to evaluate the mandibular lingual foramina (LF) and canals and their anatomic variations using cone-beam computed tomography (CBCT) technology in a Lebanese population.
Materials and Methods:
In this study, we analyzed CBCT images of 90 adult Lebanese patients (41 males and 49 females). We assessed the number and location of the LF. In additional, we measured: (a) The distance from both the alveolar crest and the inferior border of the mandible to the LF and (b) the length of the lingual canals (LCs). The data obtained was analyzed statistically using Shapiro–Wilk normality test, t-test, Chi-square, and Fisher's exact tests. Statistical significance was set at 0.05.
Results:
In our sample, the LF and canals were present in 93.33% of the CBCT analyzed, and the majority (76.64%) was located above the genial tubercles. The distance from the foramen of the superior and the inferior LCs to the alveolar crest was 16.24 ± 2.82 mm and 25.49 ± 2.43 mm, respectively. The distance from the foramen of the superior canal to the inferior border of the mandible was 14 ± 2.32 mm. The mean length of the superior canal was 5.81 ± 1.6 mm and 4.25 ± 1.2 mm for the inferior one. There were no gender-related differences in the anatomic characteristics of the LF and canals except for the distance measured from the superior canal foramina to the alveolar crest where the measurement was significantly greater in males compared to females. Neither the number of canals nor the positions of the foramina were different between males and females.
Conclusion:
Within the limits of this study, we concluded that in our sample of Lebanese adults, there was substantial variability in the LF and canals anatomy and location.
Keywords
Cone-beam computed tomography
Lebanese
lingual foramen
population


Introduction
The lingual foramina (LF) and their bony canals (LCs) are located at the internal surface of the anterior region of the mandible.[1] Studies conducted on cadavers have shown that branches from the sublingual and/or submental arteries go through these anatomic structures.[2] Therefore, despite being generally considered as a safe area when performing surgical procedures, this mandibular region may present real life-threatening hemorrhage from the above cited arterial branches following the lingual cortical plate trauma.[3]
In fact, many authors reported a wide hematoma with a large swelling of the floor of the mouth leading to a serious upper airways obstruction during implants placement in the anterior region of the mandible; this condition being related to the lingual cortex rupture/perforation.[4567]
In this respect, it is essential to assess carefully the said region by a good preoperative clinical examination including radiological imaging taking advantage of the technological advancement represented by the cone-beam computed tomography (CBCT) which provides a more accurate evaluation.
The aim of this study was to evaluate the LF and the LCs of the mandible and their anatomic variations in a Lebanese population.
Materials and Methods
This was a retrospective study which analyzed CBCT scans of Lebanese adult patients performed at a specialized maxillofacial imaging center in Beirut, Lebanon.
All volumes were taken before implant placement as a part of the patients’ treatment plan.
Patients were informed that the images might be anonymously used for research purposes at a later stage and their consent were obtained. The study got the approval of the Center Institutional Board.
The CBCT scans were acquired using the PaX-Zenith3D© machine (Vatech, Co., Ltd., Yongin-Si, Republic of Korea). The technical parameters ranged between 70–100 kVp and 7–15 mA, with an exposure time of 20 s and field of views (FOVs) were restricted to the zone of interest according to the clinical case, with respect to the “As Low as Reasonably Achievable” principle. The same FOV (80 mm × 60 mm) was used to have the same resolution on all data sets and minimize its influence on LF and canals detection.
The inclusion criteria in this study included the age of 18 years and above and the absence of any deformities in the mandible.
Ninety CBCT images of 41 males and 49 females with age ranging from 18 to 72 years meeting the inclusion criteria were selected and enrolled in the study.
The images were reviewed by two oral and maxillofacial radiologists with more than 15 years of experience. Before the study, the two observers shared software instructions and repeated appropriate manipulations for proper calibration of data collection. The evaluation procedure extended over four sessions spaced by a week.
To assess errors, all measurements were repeated by the same examiners 3 weeks after the first round without having in hands the initial results. In the case of any disagreements, the mean of the two values were taken into consideration.
For the observations, anterior cross-sections were obtained and analyzed for the following:
-
Number of LF: 0, 1 or more [Figure 1]
-
Location of LF: Above or below the genial tubercles [Figure 1]
-
Distance measurements from the LF to the inferior border of the mandible [Figure 2] and the alveolar crest [Figure 3]
-
Distance measurements from the inferior LF (if present) to the alveolar crest [Figure 4]
-
Length measurements of the LCs [Figure 5].
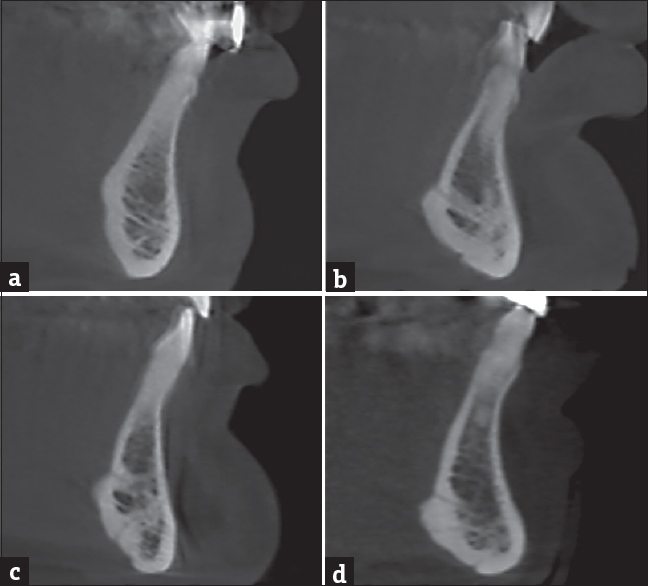
- A cross-sectional cone-beam computed tomography images at the level of the anterior mandibular region of four different patients. (a) A 25-year-old female with absence of the lingual foramen; (b) a 35-year-old female with one lingual foramen located above the genial tubercles; (c) a 40-year-old male with two lingual foramina located above and below the genial tubercles; (d) a 25-year-old female with three lingual foramina, one of them located above the genial tubercles and the two others below.
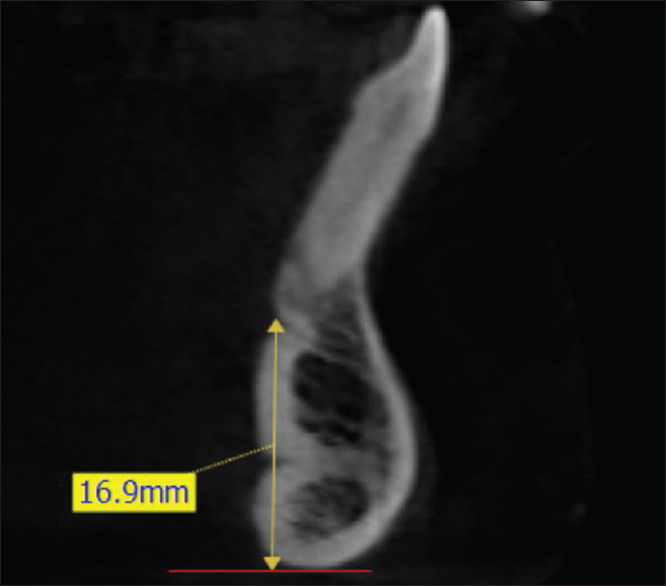
- A cross-sectional cone-beam computed tomography image at the level of the anterior mandibular region of a 36-year-old female, illustrating the method of measuring the distance between the superior lingual foramen and the inferior border of the mandible as considered by this study. One horizontal/tangent line (in red) to the inferior border of the mandible was traced; measurement in millimeters was made by drawing a vertical line (in yellow) to this horizontal line.
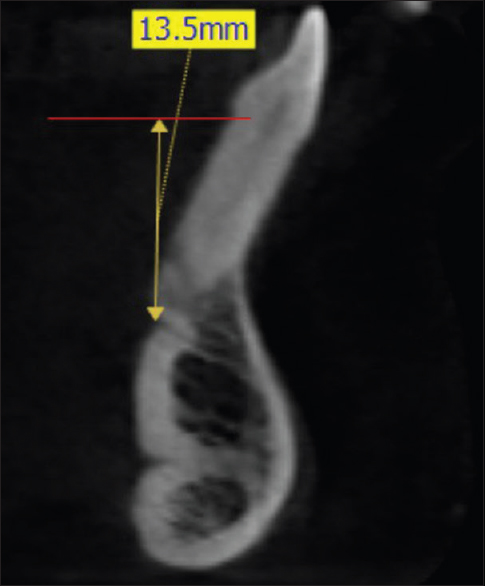
- A cross-sectional cone-beam computed tomography image at the level of the anterior mandibular region of a 36-year-old female, illustrating the method of measuring the distance between the superior lingual foramen and the alveolar crest as considered by this study. One horizontal/tangent line (in red) to the alveolar crest was traced; measurement in millimeters was made by drawing a vertical line (in yellow) to this horizontal line.

- A cross-sectional cone-beam computed tomography image at the level of the anterior mandibular region of a 36-year-old female, illustrating the method of measuring the distance between the inferior lingual foramen and the alveolar crest as considered by this study. One horizontal/tangent line (in red) to the alveolar crest was traced; measurement in millimeters was made by drawing a vertical line (in yellow) to this horizontal line.

- A cross-sectional cone-beam computed tomography image at the level of the anterior mandibular region of a 36-year-old female, illustrating the method of measuring the length of the lingual canals as considered by this study. In this case two lingual canals were detected and measured in millimeters.
Measurements were made with a thickness cut of 0.5 mm and an interval between the cuts of 0.5 mm.
For distance measurements, one tangent line to the alveolar crest and another one to the inferior border of the mandible were traced; measurements in millimeters were made by drawing a vertical line to these horizontal lines [Figures 2–4].
Statistical analyses
An initial assessment of the measured variables using Shapiro–Wilk normality tests revealed that the data, stratified in the gender groups, followed a normal distribution and subsequently, allowed the use of parametric tests.
Descriptive statistics of the outcome variables were performed to generate minimum, maximum, mean, and standard deviation of the continuous variables. In addition, the frequency and percentage were computed for the categorical variables.
An independent-samples t-test was run to determine if there were differences in the LF-LCs anatomic characteristics between males and females. The difference between genders in the categorical outcome measures related to the foramina position was assessed using the Chi-square test for association, replaced by Fisher's exact test when the expected cell count was below 5.
The IBM® SPSS® 20.0 (USA) statistical package was used to carry out all statistical analyses. Statistical significance was set at 0.05.
Results
Descriptive statistics
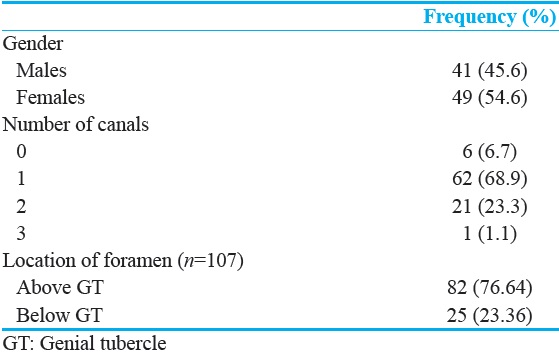
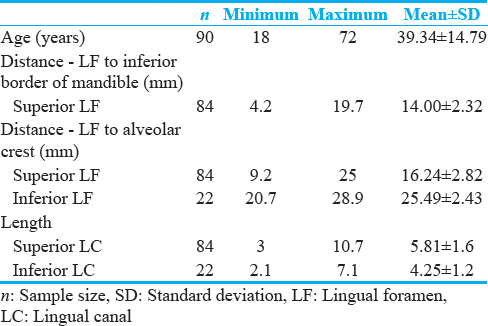
The sample included 90 CBCT radiographs of 41 males (45.6%) and 49 females (54.6%), where 107 foramina-canals were identified [Table 1].
The mean age was 39.34 ± 14.79, ranging from 18 to 72 years [Table 2].
The age was similarly distributed between males and females (P = 0.919) [Table 3].
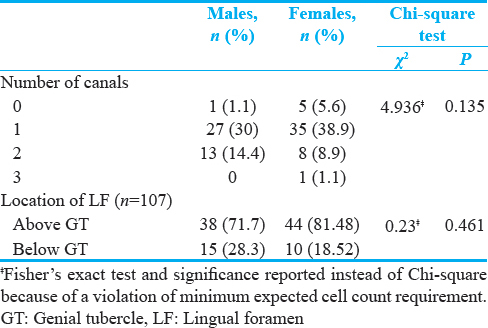
In 6 out of the 90 investigated mandibles (6.7%), the LF-LC could not be located. The remaining individuals presented with either one foramen-canal (68.9%) or two (23.3%). Only one female patient had three foramina-canals (1.1%) [Table 1].
The majority of the LF (76.64%) was located above the genial tubercles, and the remaining 25 (out of 107) were located below the tubercles [Table 1].
The anatomic characteristics of the LF varied across the total sample. The distance from the LF (the superior) to the alveolar crest ranged from a minimum of 9.2 mm to a maximum of 25 mm, with an average of 16.24 mm (16.24 ± 2.82 mm) and the similar distance measured to the second LF (the inferior), if present, was 25.49 ± 2.43 mm [Table 2].
The distance from the LF (the superior) to the inferior border of the mandible was 14 ± 2.32 mm [Table 2].
Values for the length of the LCs lied between 3 and 10.7 mm for the superior and 2.1–7.1 mm for the inferior one. The mean length of both the superior and inferior canals was 5.81 ± 1.6 mm and 4.25 ± 1.2 mm, respectively [Table 2].
Gender differences
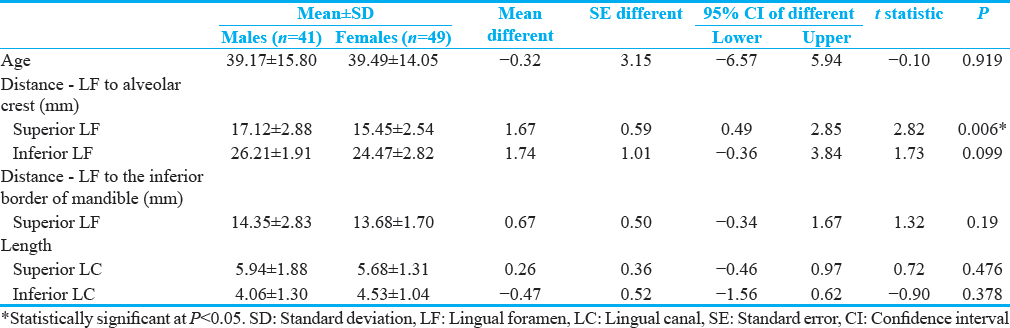
There were no gender-related differences in the anatomic characteristics of the LF-LCs except for the distance measured from the superior canal foramina to the alveolar crest (P = 0.006). This measurement was significantly greater in males (17.12 ± 2.88 mm) than females (15.45 ± 2.54 mm) [Table 3].
Neither the number of canals (χ2 = 4.936, P = 0.135) nor the position of the foramina (χ2 = 0.23, P = 0.461) were different between males and females [Table 4].
Discussion
Nowadays, dental implants are considered as the preferred line of treatment for the prosthetic rehabilitation of edentulous patients. When performed in the anterior region of the mandible, these procedures can result in the lingual cortical perforation leading to a life-threatening hemorrhage from the arteries of the LCs. Thus, knowledge of the region anatomy could be essential to prevent per- and/or post-operative complications.
Many researchers studied the anatomic variations of the LF-LCs in different populations;[28910] in the present study, we investigated them in a Lebanese population.
Presence of lingual foramina-lingual canals
In our sample, 84 out of 90 CBCT (93.33%) showed at least one LF. Our findings disagree with what has been reported by Sheikhi et al.,[8] Tepper et al.,[11] and Babiuc et al.,[12] who suggested that LF were found in 100% of the cases examined. This difference may be due to ethnicity reason or to the limited samples’ size of Tepper et al., (n = 70), and Babiuc et al., (n = 36).
On the other hand, Longoni et al.,[3] found at least one LF in 80% of dry skull mandibles and 60% of CT scans examined.
According to Jacobs et al.,[13] 82% of LF were noticed in 230 spiral CT scans. One possible interpretation for this disagreement is the imaging technique used; in this study, the thickness cut was set to 0.5 mm and an interval of 0.5 mm between the cuts unlike the 1 mm thickness used by Jacobs et al., which masks smaller bony structures.
Number and location of lingual foramina
In this study, the single LF was the most frequent (68.90%) followed by 2 LF (23.3%). Only one female patient had 3 LF (1.1%). The study results corroborate those of Tepper et al.,[11] Babiuc et al.,[12] and Liang et al.,[14] but disagree with the findings of Sheikhi et al.,[8] who noticed that double foramina are the most frequent (52.9%), and Choi et al., (40%).[10]
Interestingly, Sheikhi et al.,[8] and Choi et al.,[10] detected 4 foramina in, respectively, 3 out of 102 (2.9%) and 3 out of 20 (15%) mandibles assessed. Similarly, 5 LF were observed by Gahleitner et al.[15]
As for the LF location, in this study, the majority (76.64%) was found above the genial tubercles; among these all the single LF-LC. Furthermore, when there were two or more LF, they were located above and below the tubercles. Consequently, our results support those of Sheikhi et al.,[8] and Babiuc et al.[12]
As for gender difference, neither the position of the LF (χ2 = 0.23, P = 0.461) nor their number (χ2 = 4.936, P = 0.135) were statistically different among males and females.
Distance between the lingual foramina and the inferior border of the mandible and the alveolar crest
The distance separating LF from the alveolar crest is an essential factor to be taken into consideration to avoid per-operative complications. Consequently, the aforementioned canals must be correctly investigated before any implant placement.
In this study, the average distance between the superior LF and the alveolar crest was 16.24 ± 2.82 mm. These results corroborate those of Sheikhi et al.,[8] and Babiuc et al.,[12] who noticed for this distance a mean of 18 ± 5.63 mm and 14.2 ± 4.34 mm, respectively. From a clinical view, this leads to carefully choose the implant length, especially in atrophied mandibles.[816]
As for the average distance from the superior LF to the inferior border of the mandible, in this study, it was found to be 14 ± 2.32 mm. Our result was slightly superior when compared to that of Sheikhi et al.,[8] Choi et al.,[10] Babiuc et al.,[12] and Liang et al.,[14] who noted respective distances of 10.08 ± 2.06 mm, 12.58 ± 2.49 mm, 11.2 ± 3.1 mm, and 11.5 ± 2.8 mm.
In addition, regarding the distance between the inferior LF and the alveolar crest, in our sample, the measurements ranged from 20.7 to 28.9 mm (25.49 ± 2.43 mm).
Statically, there were no gender-related differences in all the distances measured except for the distance measured from the superior LF to the alveolar crest (P = 0.006) which turned out to be significantly greater in males (17.12 ± 2.88 mm) than that of females (15.45 ± 2.54 mm).
Length of the lingual canals
In another concern, the mean length of both, the superior and inferior LCs, was 5.81 ± 1.6 mm and 4.25 ± 1.2 mm, respectively. As a result, this shows that in our study, the length of LC was slightly lesser than those of Sheikhi et al., (7.83 ± 2.25 mm for the superior and 6.33 ± 1.65 mm for the inferior LCs),[8] and Liang et al., (6.8 ± 2.3 mm for the superior LCs and 6.1 ± 2.6 mm for the inferior ones).[14]
Finally, as a matter of fact, this study aiming to assess the LF-LCs in a Lebanese population is not without limitations. Although most measurements were taken with high reliability, the limited number of canals assessed makes necessary the investigation on a larger group of patients which lead to more accurate results.
Conclusion
In our sample of Lebanese adults, there was a significant variability in the mandibular LF and their bony canals anatomy and location. Given the serious risk in case of underestimation, these structures must be taken into consideration before implant placement procedures in the region to prevent possible complications such as extensive life-threatening hemorrhage. In this respect and for safety reasons and higher success rates, a preoperative CBCT is highly recommended.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2017/7/1/16/205175
References
- Lingual foramina and canals. In: Clinical Oral Anatomy. Switzerland: Springer International Publishing; 2016. p. :463-87.
- [Google Scholar]
- Classification of the lingual foramina and their bony canals in the median region of the mandible: Cone beam computed tomography observations of dry Japanese mandibles. Oral Radiol. 2007;23:42-8.
- [Google Scholar]
- Lingual vascular canals of the mandible: The risk of bleeding complications during implant procedures. Implant Dent. 2007;16:131-8.
- [Google Scholar]
- Hematoma of the floor of the mouth and airway obstruction during mandibular dental implant placement: A case report. Oral Maxillofac Surg. 2008;12:223-6.
- [Google Scholar]
- Hemorrhaging associated with endosseous implant placement in the anterior mandible: A review of the literature. J Periodontol. 2004;75:631-45.
- [Google Scholar]
- Floor of mouth haemorrhage and life-threatening airway obstruction during immediate implant placement in the anterior mandible. Int J Oral Maxillofac Surg. 2006;35:961-4.
- [Google Scholar]
- Clinical assessment and surgical implications of anatomic challenges in the anterior mandible. Clin Implant Dent Relat Res. 2003;5:219-25.
- [Google Scholar]
- Assessing the anatomical variations of lingual foramen and its bony canals with CBCT taken from 102 patients in Isfahan. Dent Res J (Isfahan). 2012;9(Suppl 1):S45-51.
- [Google Scholar]
- Assessment of the appearance, location and morphology of mandibular lingual foramina using cone beam computed tomography. Int Dent J. 2016;66:272-9.
- [Google Scholar]
- Topography of the lingual foramen using micro-computed tomography for improving safety during implant placement of anterior mandibular region. J Craniofac Surg. 2013;24:1403-7.
- [Google Scholar]
- Computed tomographic diagnosis and localization of bone canals in the mandibular interforaminal region for prevention of bleeding complications during implant surgery. Int J Oral Maxillofac Implants. 2001;16:68-72.
- [Google Scholar]
- Cone beam computed tomography observations of the lingual foramina and their bony canals in the median region of the mandible. Rom J Morphol Embryol. 2011;52:827-9.
- [Google Scholar]
- Appearance, location, course, and morphology of the mandibular incisive canal: An assessment on spiral CT scan. Dentomaxillofac Radiol. 2002;31:322-7.
- [Google Scholar]
- Lingual foramina on the mandibular midline revisited: A macroanatomical study. Clin Anat. 2007;20:246-51.
- [Google Scholar]
- Lingual vascular canals of the mandible: Evaluation with dental CT. Radiology. 2001;220:186-9.
- [Google Scholar]
- Patient selection and preparation. Chicago: Quintessence; 1985. p. :199-209.




